
Abstract
Abstract
Introduction:
Pancreatico-colonic fistula (PCF) is a rare adverse effect secondary to severe acute or chronic pancreatitis and potentially life-threatening because of abdominal sepsis. Over-the-scope clip (OTSC®) system is a recently developed endoscopic device and has been successfully used for bleeding and perforations of the gastrointestinal tract. We hereby report a series of patients with PCFs in whom OTSC was used.
Materials and Methods:
From January 2011 to December 2018, we retrospectively collected data on cases of PCFs with endoscopic treatment using the OTSC system. After conservative management, the endoscopic intervention was carried out on patients in deep sedation by single skilled operators.
Results:
A total of 9 patients were enrolled and patients were treated with 14/6 t-type OTSC. PCF occurred secondary to chronic (n = 5) and acute pancreatitis (n = 4). There were no adverse effects related to the endoscopic procedure itself. Further endoscopic evaluation was performed 8 weeks later and revealed a successful fistula closure in 4 patients with chronic pancreatitis (80%) and in 2 patients with acute pancreatitis (50%). An insufficient fistula closure was observed in 3 cases because of dislocation of the OTSC and an additional surgical procedure was required.
Conclusion:
The OTSC system seems to be safe and effective in short-term management of PCFs because of acute or chronic pancreatitis in addition to the already established nonsurgical therapy. However, the OTSC closure of PCFs in patients with acute pancreatitis seems to be associated with a higher failure rate. To sum up, more evidence and long-term studies are needed to determine the criteria for the use of OTSC in closure of PCFs owing to acute or chronic pancreatitis.
Introduction
Acute pancreatitis is an inflammatory condition of the pancreas, whereas chronic pancreatitis is a progressive fibroinflammatory process that results in permanent structural damage. Both entities can be life-threatening because of systemic or local adverse effects. Gastrointestinal (GI) fistula is one of the well-recognized adverse effects secondary to severe acute or chronic pancreatitis. 1 Pancreatico-colonic fistula (PCF) is a rare adverse event, but a mortality rate of up to 37% was observed. 2 A spontaneous fistula closure is rare and owing to life-threatening abdominal sepsis PCF early diagnosis and treatment is required. In the past, traditional treatment of PCF has been surgical repair 3 and nonsurgical treatments include endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic sphincterotomy and pancreatic duct (PD) stenting. 4 Recently, technological advances in endoscopic devices had provided an alternative approach. One of the recently established devices is the over-the-scope clip (OTSC®) system (Ovesco AG, Tübingen, Germany) that has been developed for hemostasis of GI bleeding and closure of iatrogenic or foreign body perforations of the colon.5,6 To the best of our knowledge, no studies have investigated the use of OTSC for the management of PCFs.
Materials and Methods
In this retrospective single-center case series we analyzed data of all OTSC applications from our Division of Interdisciplinary Endoscopy at Universitätsmedizin Greifswald (Germany) from January 2011 to December 2018. We collected data on 9 patients with PCF secondary to acute (n = 4) or chronic pancreatitis (n = 5), in whom OTSC closure was performed. In detail, our case series included only those patients with a PCF referred by the surgeon for a conservative attempt to avoid high-risk surgical intervention. PCF was defined as an abnormal connection between the pancreas or necrosis cavern and the colon occurring owing to an acute or chronic pancreatitis. After conservative management, OTSC closure was recommended and carried out. A written informed consent was obtained in all cases. The endoscopic intervention was performed on patients in deep sedation by single skilled operators. Demographic data are given in Table 1. Primary treatment successful outcome was defined as a satisfactory application of the OTSC on target site and/or resolution of PCF confirmed by a leak test. In contrast, failure was defined as unsatisfactory application of the OTSC and/or failure of resolution of fistula.
Demographic Data, Indications and Outcomes
COPD, chronic obstructive pulmonary disease; CT, computed tomography; IDDM, insulin dependent diabetes mellitus; NIDDM, non-insulin dependent diabetes mellitus; M, male; OTSC®, over-the-scope clip; PCF, pancreatico-colonic fistula; PD, pancreatic duct.
Results
A total of 9 male patients were enrolled (ages 50–74 years, mean age 62 years). PCF occurred secondary to acute (n = 4) and chronic pancreatitis (n = 5). Age, indications, comorbidities, medications, and outcomes of patients are given in Table 1. All 9 patients began standard conservative management of PCF: no oral food intake, total parenteral nutrition, and antibiotics. Percutaneous catheter drains were present in 7 patients and a PD stent was placed using ERCP in 4 patients before fistula diagnosis.
Because of signs of abdominal sepsis, the patients were further investigated at first with a computed tomography (CT) scan and secondary with a lower endoscopy and GI tract X-ray with contrast. Examples of PCFs on CT scan and colonoscopy are given in Figures 1 and 2, respectively. The mean diameter of the PCFs was 22 mm (range = 10–30 mm) and was measured by comparison with a foreign body retrieval grasper (diameter of 6 mm in an open position). The edges of fistula were edematous in 7 cases and fibrotic in 2 cases. All patients were treated with 14/6 t-type OTSC (Ovesco AG; Fig. 3). A twin-grasper forceps (Ovesco AG) was used in 5 cases to facilitate the approximation of gaping edges of the fistula before release of the OTSC. In all cases one OTSC for fistula closure was used. The average time between the onset of signs of abdominal sepsis and OTSC placement was 6 days. There were no complications related to the endoscopic intervention and no complications from the anesthesiologic perspective. In 3 patients with enclosed percutaneous catheter drains a subsequent fluoroscopy was performed and it showed no contrastographic spreading through the wall (Fig. 4). In all cases, we observed patients clinically well and after a few days, oral food intake was resumed and drain withdrawal was started. The average hospital stay after the OTSC treatment was 10 days. A follow-up colonoscopy and basic clinical examination was performed 8 weeks later and there was successful fistula closure in 4 patients with chronic pancreatitis (80%) and in 2 patients with acute pancreatitis (50%). In 1 patient with chronic and 2 patients with acute pancreatitis fistula recurrence was observed owing to dislocation of the OTSC and an additional procedure in terms of a surgical hemicolectomy was required.

Coronal computed tomography image depicting a left-sided pancreatico-colonic fistula (arrow) involving the splenic flexure of the colon (C) and an area of walled-off pancreatic necrosis (N).
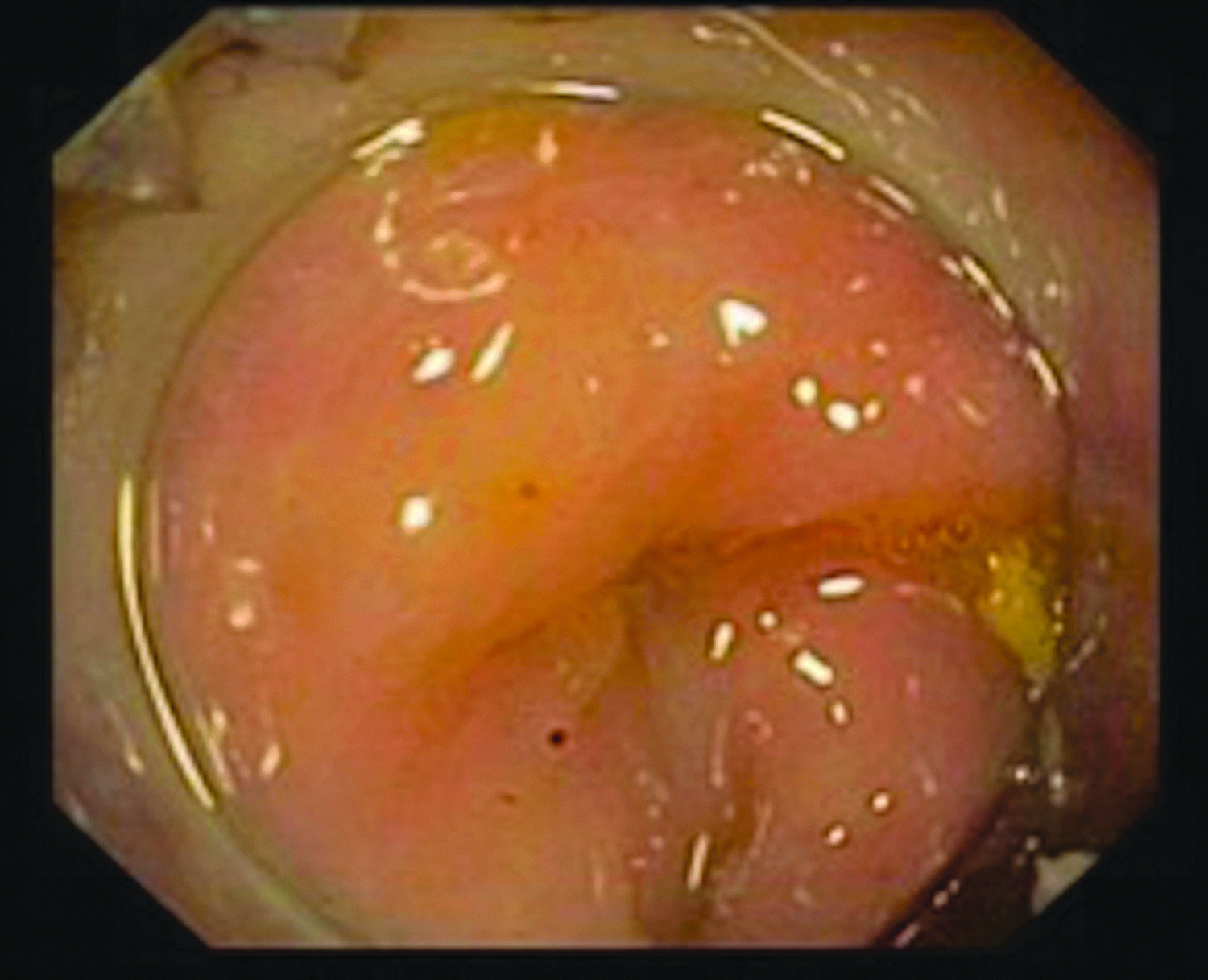
Endoscopic image of pancreatico-colonic fistula from the colonic side.
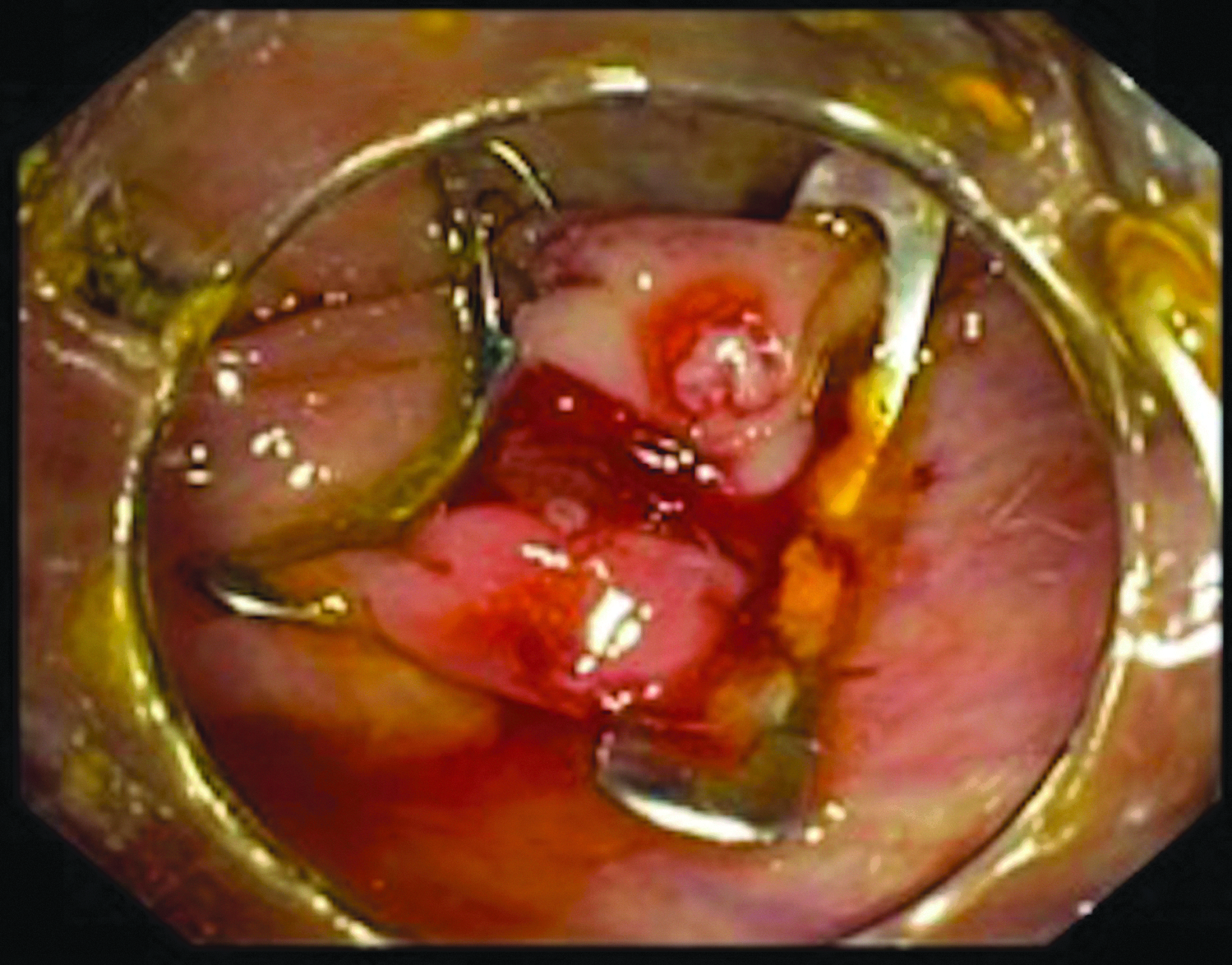
Endoscopic view of the deployed over-the-scope clip and successful closure of the pancreatico-colonic fistula.
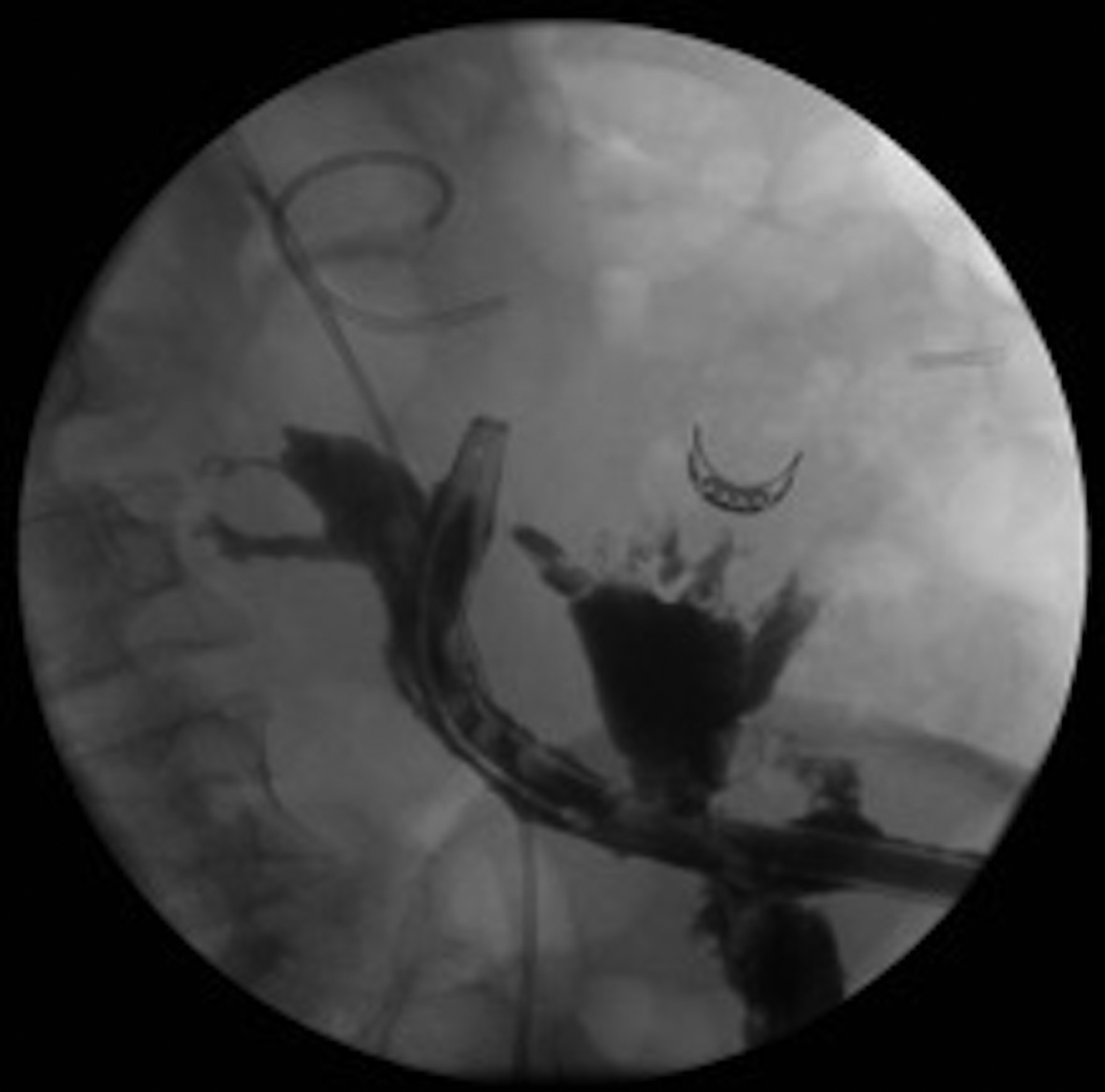
Subsequent fluoroscopy after over-the-scope clip placement.
Discussion
Spontaneous fistulae from the pancreas to neighboring organs because of acute and chronic pancreatitis are a well-established complication and potentially life-threatening. The etiology of pancreatitis associated with PCFs in this case series is similar to the overall causes of pancreatitis, with gallstones accounting for >50%. 7
Diagnosis of PCFs is difficult and may be suggested by symptoms such as diarrhea, fever, hematochezia, and abdominal pain. 8 In this series, symptoms tended to be nonspecific, and diagnosis was made by colonoscopy in 5 patients (55%), followed by contrast-enhanced CT scan in 3 patients (33%) and fluoroscopic percutaneous tube-check imaging of an existing drain in 1 patient (11%).
According to a literature review from Abcarian et al., 8 the most frequently sites of fistulization were the transverse (52%) and the left colon (44%), whereas Heeter et al. 9 showed PCFs localized to the left colon in 85% of 20 analyzed cases. In this study, the main site of fistulization was the left colon, accounting for 78% of cases. However, the association with unique colon sections is a result of the close approximation of the left colon to the body or tail of the pancreas. Therefore, we recommend particular attention to this area when PCF is suspected.
In the past, standard treatment of PCFs has been surgery, as spontaneous closure is rare, and abdominal sepsis can be lethal. 3 A retrospective study by Kochhar et al. 1 showed that all patients admitted to their unit over a 4-year period with acute pancreatitis and fistulization to the colon underwent surgery. A published report from 1986 showed a high mortality rate of >50% of nonsurgically treated PCFs related to massive hemorrhage or overwhelming sepsis, compared with 15% in patients treated surgically. 10
Nonsurgical treatments for PCF include ERCP with pancreatic sphincterotomy and PD stenting, 4 application of fibrin glue, 11 percutaneous drainage, 9 and endoscopic techniques using several devices such as transenteric drainage, hemoclips, endoloops, and rubber bands.12–14 Success rate varies between 55% and 69% and additional surgical management is often required. 15
One of the recently established technological advances in endoscopic devices is the OTSC system. A retrospective review by Law et al. 16 of 47 patients who underwent OTSC placement for closure of GI fistula reported an initial technical success of 89%, but long-term clinical success was achieved in only 53%.
The management strategy for PCFs is still based on the patients' clinical picture and local expertise and, therefore, is based on poor evidence. The OTSC system has been reported to be effective for the management of post-pancreaticogastrostomy pancreatic fistula in a prospective study including 7 patients 17 and for the closure of PCFs, reported at unique case reports.18,19 In our experience, the following indications seem suitable for applying an OTSC after nonsurgical therapy to avoid high-risk surgical intervention: (1) chronic, small fistulas (diameter <30 mm), (2) no massive fibrosis of the fistula, and (3) no infected cavity that would be left undrained after fistula closure.
In this case series, technical and short-term success of additional OTSC placement after nonsurgical treatment with PD stenting and/or percutaneous catheter drainage was achieved in 4 cases with chronic pancreatitis (80%) and in 2 cases with acute pancreatitis (50%). The OTSC placement reduced the length of hospital stay and decreased the costs of treatment and also the necessity for additional procedures that can cause life-threatening complications. Moreover, the OTSC system is fully biocompatible, may stay in place indefinitely, and does not contraindicate magnetic resonance imaging. 20
However, the retrospective design, low number of cases, and heterogeneity of patients are a strong limitation of this study. There may be bias related to carrying out the procedures in a center experienced in using OTSC for other indications. In addition, the consistency of PCF has a decisive influence on the success of OTSC treatment. Severe fibrosis and the stage of an acute pancreatitis may limit the ability to draw tissue into the applicator cap, precluding successful OTSC deployment and feasibility. As the edge of PCF was fibrotic in only 2 cases in the present series, more studies are needed focusing on this issue.
In conclusion, this single-center retrospective series suggests that PCFs secondary to acute or chronic pancreatitis can be managed effectively and safely by using the OTSC system in addition to the already established nonsurgical therapy. However, an interdisciplinary collaboration among the surgeon, gastroenterologist, radiologist, and nutritional staff is required to correctly manage these patients. To our knowledge, this is the first case series of use of OTSC for endoscopic closure of PCF. Nonetheless, prospective, randomized, and long-term studies comparing surgery, nonsurgical treatment, and endoscopic intervention are needed to determine the criteria for use of OTSC and to define the exact place within treatment algorithms of PCF owing to acute and chronic pancreatitis.
Footnotes
Disclosure Statement
The applied OTSC® system was provided by Ovesco AG, Tübingen, Germany. Ovesco AG has not verified, and is not responsible for, the validity of the data analysis or the conclusions derived by the authors. No competing financial interests exist.