
Abstract
Abstract
Background:
Self-expanding metal stents (SEMSs) in different geometric shapes are well established treatment options in diseases of the esophagus. Mechanical properties and stent design may have an impact on patient comfort, migration rate, and removability. In this in vitro study, we evaluated mechanical properties of three segmented SEMSs (segSEMSs) for the esophagus with regard to distinct stent sections.
Materials and Methods:
Radial forces were measured using a testing method distinguishing between circumferential radial and local radial force. The center parts of the segSEMSs were measured for circumferential radial forces without being affected by the flared ends. Axial forces were measured at 20° bending.
Results:
Circumferential radial force measurements over the full stent length showed substantial differences against measurements of the center parts of the stents as the flared ends falsify test results by up to 53%. Although circumferential radial forces of the center parts were about the same (<10% variances) for all segSEMSs, local radial forces showed considerable differences of up to 26%. One segSEMS showed high axial forces, whereas the other two only needed half of the force (up to 53%) to be bent to 20°.
Conclusion:
Flared ends of segSEMSs have a substantial impact on radial force measurements and therefore alter test results, confirmed by our separated center part test of segSEMSs. Our innovative setup whereby we compressed the stent in an asymmetric manner (local radial force) and evaluated sections of stents separately, indeed revealed differences to circumferential measurements, leading to a more in-depth knowledge of stent characteristics.
Introduction
Self-expanding metal stents (SEMSs) are available in different geometric shapes and covers, and offer a well-established treatment option in both benign and malignant diseases of the esophagus.1–3 Mechanical properties and stent design have an impact on patient comfort, migration rate, and removability, and have gone through a developmental evolution process over the last 20 years. 2 First, in vitro studies evaluating stents and their mechanical properties were published in 1999 by Chan et al. and followed by another study by Moon et al. in 2001.4,5 They described the importance of in vitro biophysical stent characterizations to understand their behavior in vivo, which should be considered to select the optimal stent with a maximum of clinical efficacy in the individual patient. In 2013, Hirdes et al. published a detailed study about the radial and axial force characteristics of still available and currently used esophageal stents. 6 However, the author concluded that the results were not sufficient as a single parameter to understand their clinical effectiveness.
The mechanical functions of esophageal SEMSs are complex and differ with regard to the therapeutic indication. Every stent consists of different sections that perform different tasks: the proximal and distal end (flared ends) should align with the esophageal contour to provide sealing and prevent migration whereas the center parts, placed across the site of obstruction, expand the stenosis and consequently diminish dysphagia and obstruction. Further, we assumed that the flared ends may have a substantial impact on test results. Therefore, flared ends were taken off and measured separately. So far, there are no data available concerning a separate evaluation of the different sections (flared end versus shaft). In addition, only limited in vitro data exist concerning the physical properties of SEMSs for esophageal placement in general.
The aim of this study was to evaluate mechanical properties of commercially available segmented SEMSs (segSEMSs) for the esophagus with regard to distinct stent sections.
Materials and Methods
In the study period (December 2017–March 2018) only three companies provided segSEMSs in Germany (Choostent®; M.I. Tech, Korea; ESO; Endo-Flex, Germany; ST71; Micro-Tech, China). For our study we choose segSEMSs with the same length of the center part (Fig. 1). All three segSEMSs are made of braided nitinol, a nickel-titanium alloy, and were either fully or partially covered. The connection of the individual segments consists of braided yarn (ESO and ST71) or the nitinol wire continues from one to the next segment (Choostent). Lengths ranged between 100–140 mm with comparable diameters between 20–22 mm (body) and 26–28 mm (flared end) when stents are fully expanded. We removed all crowns by separating the connection of the individual segments resulting in three equally long and straight segments of 75 mm. Stent characteristics are summarized in Table 1. The wire diameter did not differ between stents (0.2 mm). The wire numbers per circumference were 16 with the Choostent and 24 with the ESO and ST71 stent. Finally, all test measurements for each segSEMSs were performed five times.
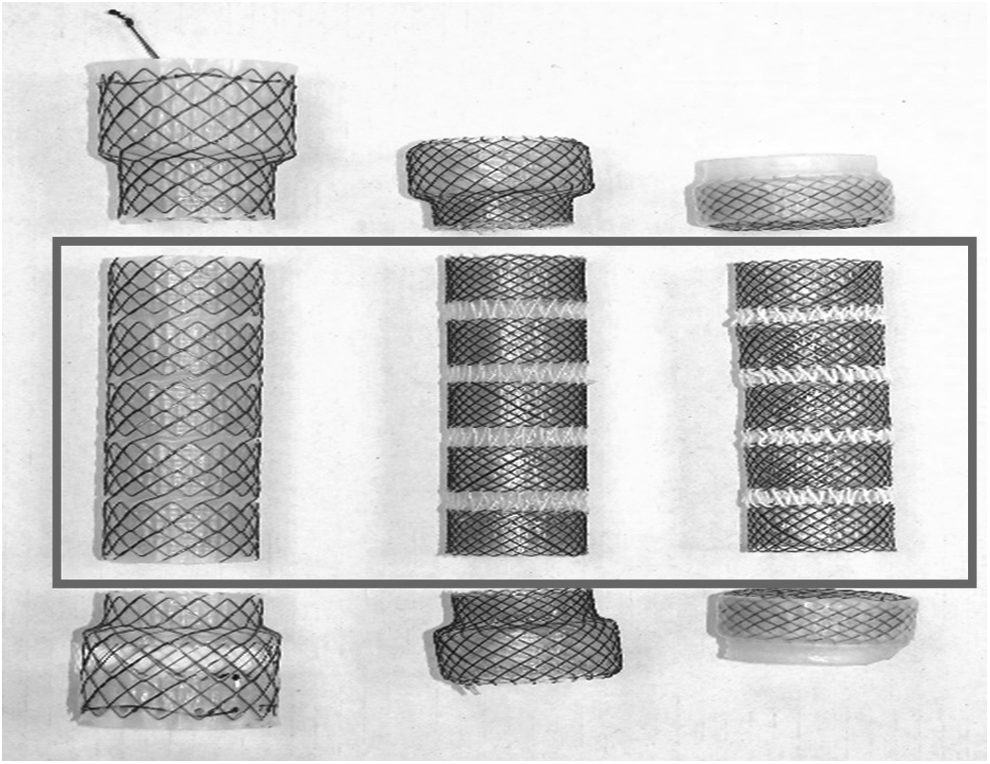
Tested segSEMSs with the same length of center parts (75 mm, red box). segSEMS, segmented self-expanding metal stent.
Technical Characteristics and Specifications of Tested Segmented Self-Expanding Metal Stent
Circumferential radial force measurement
In the case of radial force, a distinction must be made between an external force that causes the stent to reduce its diameter (radial resistance force), and the restoring force of the stent with which it tries to increase to its nominal diameter (chronic outward force). In this study, circumferential radial force measurements complies a circular compression of the complete stent circumference. In our radial force measurements, we focused on expansion force, since this is the determining force each stent needs to dilate the targeted stenosis in the esophagus. We compared forces at 15 mm and shape of expansion curves.
A stent crimping machine able to measure radial forces (CR-240-SA; Medical Production Technologies BV; NR Leek, The Netherlands) comparable to the RX500 (Machine Solutions, Flagstaff, Arizona) used by Hirdes et al. and Isayama et al. was used to measure circumferential radial resistance force and expansion force (Fig. 2).6,7 The machine provides a crimping head with a length of 240 mm and a maximum diameter of 32 mm, which can be reduced to less than 1 mm while recording the radial force as a function of the diameter. Each test sample was fully positioned in the crimping machine. Subsequently, they were compressed to a diameter of 9 mm and the radial resistance force of each test sample was recorded while compressing. Afterward, the crimp head completely opened while recording the expansion force of the stent. To ensure comparability with previous studies on esophageal stents, the outward force for all samples was compared at a crimp head diameter of 15 mm during the expansion phase.
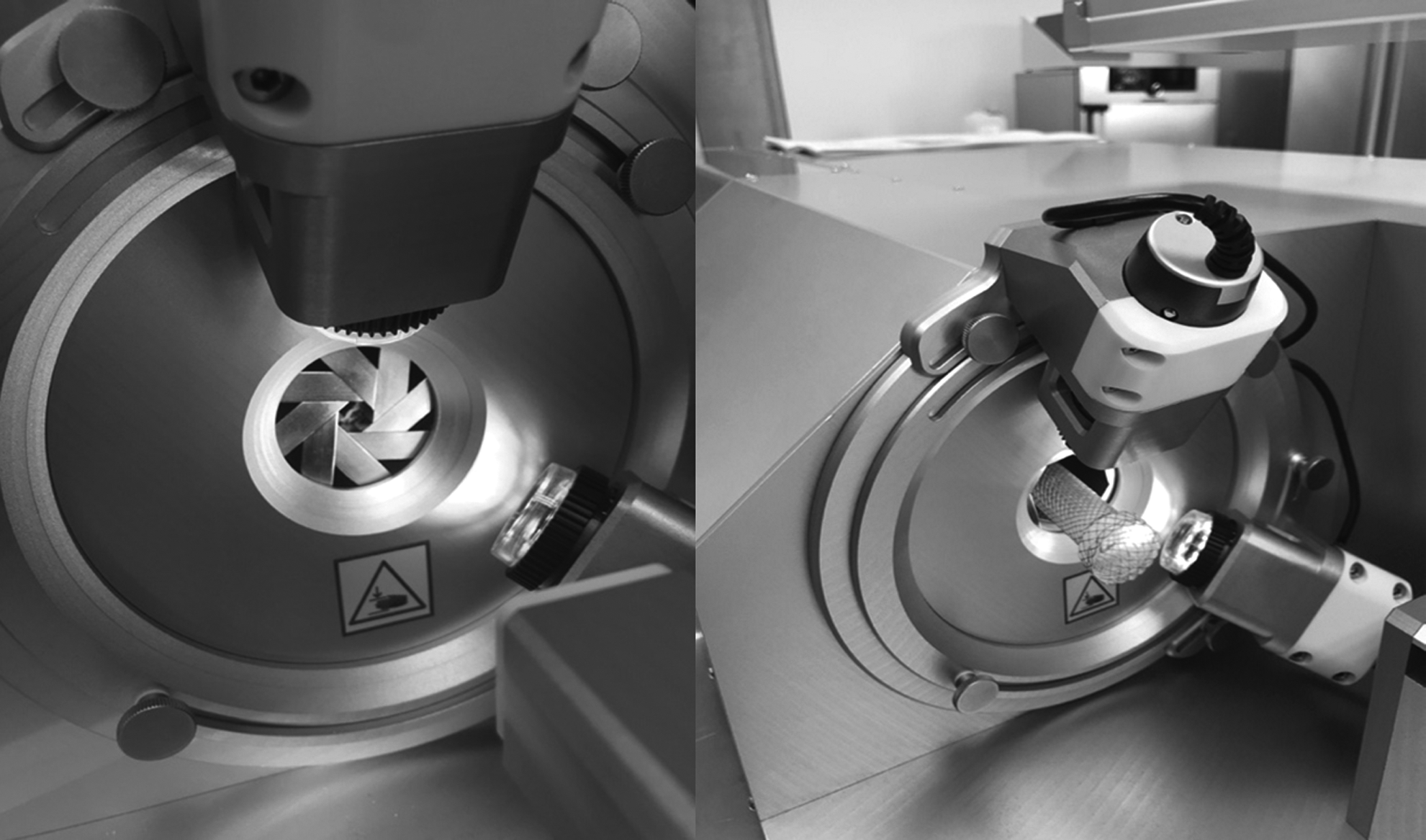
Crimping machine (CR-240-SA; Medical Production Technologies BV; NR Leek, The Netherlands).
Circumferential radial force measurement of center parts and flared ends
Flared ends and center parts were then measured individually according to the previously described radial force measurement.
Local radial force measurement of center parts
If stents are not straight and homogeneous in their design, they can be divided into zones with different functions. To determine the differences between stents within a certain zone according to radial force resistance, a different test method is necessary rather than testing the stent over the whole length in a crimping head. This was achieved through a local compression with a spherical stem placed in the middle of the stent (test machine: MultiTest 2.5-xt [Mecmesin Limited, UK] with 100 N load cell). In the local radial force test setup each stent was positioned on a 90° v-shaped holder supporting only the center area of the stent, leaving both ends free without movement restrictions (Fig. 3). A stem with a diameter of 10 mm and a spherically formed tip was driven perpendicularly to the holder against each stent reducing the diameter down to 9 mm (diameter of the SEMS release instrument) while recording the radial resistance force. After that, the stem was completely retracted from the stent while recording the local radial force of the stent. For a meaningful comparison against previous studies, the local radial force for all samples was compared at a stent diameter of 15 mm during the expansion phase.

Technical drawing of setup for local radial force measurement of center parts.
Axial force measurements
For axial force measurements (test machine: MultiTest 2.5-xt [Mecmesin Limited] with 100 N load cell), each test sample was positioned on a rod that fits the inner diameter of the stent. About one-third of the stent was seated on the rod and the remaining end stayed flexible without support. A ring that fits to the outer diameter of each sample was slipped over the stent to clamp it down to the rod. The front side of the ring was aligned to the front side of the rod, (Fig. 4). At a distance of 20 mm from the front side of ring and rod an axial force was exerted perpendicularly on each test sample to bend it until an angle of 20° was reached. The force needed to bend the stent was continuously recorded. This setup is comparable to the procedures described by Hirdes et al. and Isayama et al.6,7
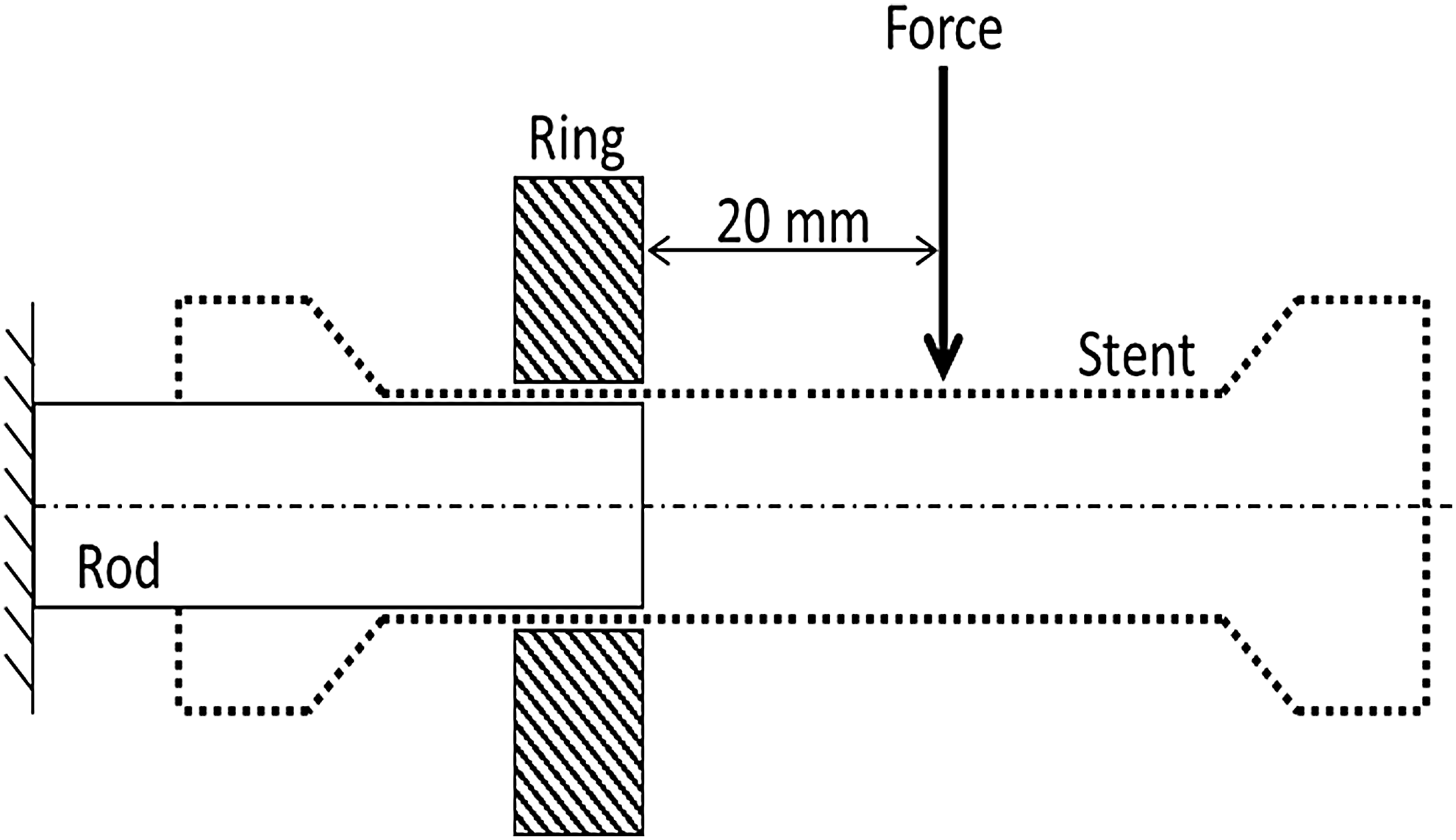
Technical drawing of setup for axial force measurement.
Results
The five times row measurement of each segSEMSs in our study showed following same test results in each setup:
Circumferential radial force
Measuring the circumferential radial force over the full length of each stent, the ESO (45.2 N) shows a lower result at the 15 mm expansion diameter against the Choostent (67.6 N) and the ST71 (63.4 N), although the ESO and the ST71 have a similar construction. The curves of the expansion forces show linear decrease between a stent diameter of about 12 and 18 mm. At a stent diameter below 12 mm the forces increase more as the stent is compressed close to its minimal diameter. Above 18 mm the force drops depending on the real nominal diameter of each stent (Fig. 5).

Circumferential radial force diagrams of complete segSEMS with flared ends (top), center part of segSEMS (middle), and the flared ends of each segSEMS (bottom) at 15 mm expansion force. segSEMS, segmented self-expanding metal stent.
Measuring the circumferential radial force over the center part of each stent only, there are only minor differences between the segSEMSs with radial forces at 15 mm expansion diameter of 33.1 N for the Choostent, 34.3 N for the ESO, and 36.4 N for the ST71. The curves are similar to the previous curves over the complete stent but at a lower scale.
As expected, the curves for the flared ends start and end at a higher diameter compared with the center parts, but they show a similar progression to the previous curves. The ESO (8.9 N) again shows a lower result at 15 mm expansion diameter against the Choostent (17.4 N) and the ST71 (15.3 N), as determined during the measurements over the full length.
Local radial force
All graphs showed nearly linear curves with compression and expansion forces close by (Fig. 6). The local radial force during expansion at a remaining stent diameter of 15 mm was highest for the Choostent (1.61 N), followed by the ST71 (1.39 N) and the ESO (1.19 N).

Local radial force test results of segSEMSs. segSEMS, segmented self-expanding metal stent.
Axial force
Results of axial force measurements are shown in Figure 7. Similar forces were measured for the ESO and the ST71 with 0.76 N and 0.70 N. In contrast, the Choostent needed more than twice the force (1.51 N) to bend to 20°.

Axial force test results of segSEMSs. segSEMS, segmented self-expanding metal stent.
The results of all previous test methods are summarized in Table 2.
Measured Forces Including all Test Methods of all Evaluated segSEMSs
segSEMS, segmented self-expanding metal stent.
Discussion
Esophageal stents are successfully used prostheses to treat strictures and endoluminal obstructions, of both benign and malignant origin. Furthermore, they are utilized to treat fistulas, leaks, and perforations. 8 Through their segmented structure, segSEMSs are assumed to provide better adaptation, especially to the contour of tortuous esophageal lumens. To achieve the highest treatment efficacy, mechanical properties should be considered before stent deployment. However, studies evaluating stent characteristics (in vitro and in vivo) are limited. To our knowledge this is the first in vitro study focusing on mechanical properties of distinct functional stent sections and thus providing a deep insight into interactions and influences between different stent parts.
We hypothesized a possible influence of the flared ends on the radial forces. When measuring the complete segSEMS, including the flared ends similar to Hirdes et al. and Isayama et al., first test results showed that one stent shows a lower result (45.2 N) at a 15 mm expansion diameter against the two other (67.6 and 63.4 N), where the major difference in design was the flared end.6,7 To prove our hypothesis, we removed all flared ends by separating the connection of the individual segments to compare three equally long and straight center parts of 75 mm. After that, we measured radial forces again resulting in different test outcomes: all three stents showed similar radial forces of center parts between 33 and 36 N when flared ends were not interfering with the measurement and not altering test results up to a substantial 52%. Since flared ends are placed proximally and distally to the site of the esophageal obstruction 9 and are therefore not involved in expanding the obstruction, in vitro measurements including the flared ends are falsified in test results when it comes to the in vivo radial expansion force of stent center parts. Flared ends alter test results to the extent of their own radial force results.
To bring our test results closer to an in vivo situation, we created a new test setup to our in vitro evaluation: the local radial force test method. This setup meets the requirements proposed by Moon et al. who recommended a test setup mimicking an occlusion that is not circumferential and compressing the stent in an asymmetric manner. 5 It should also be applicable for nonsegmented stents with flared ends that cannot be cut off. Considering only the radial force results, all three segSEMSs seemed to be equal with regard to their expansion potential in vivo. By contrast, local radial force also showed considerable differences up to 26%. We assume that the local radial force should be considered one of the main mechanical properties, probably more important than radial force (if measured with flared ends) in terms of clinical outcome and stent occlusion rate.
Concerning the axial forces, the Choostent showed high axial forces of 1.51 N, whereas the other two only needed half the force (up to 53%; 0.70 and 0.76 N) to bend at 20°. This can be explained due to the type of connector between the individual segments. In the Choostent, the nitinol wire continues from one segment to the next and thus represents the connector. For this reason, the Choostent's axial resistance against kinking of the stent is higher but it also leads to a higher local radial force (compare with the previous paragraph). Brought into the context of the study conducted by Hirdes et al., the Choostent would fall into a moderate category and both the other segSEMSs into a low axial force category. 6 We assume that the stent potential to align to the contour of a tortuously obstructed lumen behaves reciprocally to the required axial force.
There are several limitations in our study. First, the currently limited variety of available segSEMSs in the German market. Second, the setting of an in vitro evaluation, and finally a lack of currently available clinical trials and experimental ex vivo setups to compare our study results.
In our study, we were able to demonstrate different mechanical properties of all currently available segSEMSs in Germany. Furthermore, our study reveals the tremendous impact of the stent flared-ends with regard to radial force that might have led to an overestimation of reported radial expansion forces in earlier in vitro studies. Therefore, we agree with Moon et al. that the biophysical characterization of stents is only the first step toward understanding their in vivo behavior. 5 However, this also implies a need for new and innovative in vitro testing methods to evaluate mechanical properties, since stents are mostly compressed in vivo in an asymmetric manner. 5 We addressed this need with a new test technique (local radial force) as demanded by Moon et al. and proved them right by actually finding different results as would be expected by comparing radial force and local radial force and furthermore discovering impacts and interactions of distinct stent parts. 5
From an in vitro perspective, segSEMSs with a high radial, high local radial, and a low axial force may be a preferred stent of choice in the treatment of malignant lumen opposing conditions in the esophagus. In vivo studies are needed to confirm our hypothesis.
Footnotes
Acknowledgments
We would like to thank Bess Pro GmbH (Berlin, Germany) for their technical support and providing us the technical equipment. We thank Ms. Claire Cahm for proofreading.
Disclosure Statement
S.L. is coworker of the Bess Pro GmbH, Germany. All other authors declare that no competing financial interests exist.