
Abstract
Abstract
Background:
Although previous studies have evaluated whether use of irrigation decreases postoperative intraabdominal abscess (PO-IAA) formation, these studies treated irrigation as a dichotomous variable and concluded that no irrigation resulted in a decreased incidence of PO-IAA formation. However, a recent study found decreased incidence with small aliquots to a total volume of 6 L. We hypothesized that higher volumes of irrigation would result in a lower incidence of PO-IAA.
Materials and Methods:
A postoperative template was developed as a quality improvement initiative and included descriptors for complex appendicitis and volume of irrigation. Data were prospectively collected from February 2016 to December 2018. Patients with complex appendicitis (fibropurulent exudate, extraluminal fecalith, well-formed abscess, visible hole in the appendix) were identified and analyzed by using standard statistical analysis. Volume of irrigation was categorized for analysis.
Results:
Two thousand three hundred six appendicitis patients were identified; 408 had complex appendicitis (17.7%). Three hundred eighty-four patients with complex appendicitis had documented irrigation volumes. The overall incidence of PO-IAA was 13.8%. Irrigation was commonly used (92.7%). The median amount of irrigation was 1000 mL (500 mL, 2500 mL), but it ranged from none to 9000 mL. There was no overall difference in the volume of irrigation used between those who developed a PO-IAA and those who did not (P = .34). No specific intraoperative finding was associated with the development of PO-IAA. Increasing volume of irrigation did not lower PO-IAA incidence (P = .24).
Conclusions:
The volume of irrigation did not appear to affect the rate of PO-IAA formation. The use of irrigation should be left to the discretion of the operating surgeon.
Introduction
Acute appendicitis is the most common reason for emergent abdominal surgery in children, with one-third of these patients presenting with a complex, or ruptured, appendicitis. 1 Many of these patients have a prolonged hospital course and upward of 18% will develop a postoperative intraabdominal abscess (PO-IAA). 2 This complication results in an estimated additional week of hospitalization and additional invasive procedures. 3
The surgical dogma of “dilution is the solution to pollution” has often been prescribed as a way to decrease the bacterial load within the abdomen, thus decreasing the overall incidence of PO-IAA formation. 4 However, within the past few decades, an increasing amount of attention has been focused on minimizing the amount of irrigation during the operation, or removing irrigation completely from practice. Within the adult patient population, studies were conducted that showed an increased rate of PO-IAA after irrigation in perforated appendicitis.5,6 Following these studies, pediatric-specific studies began to hint at the same association or found no relationship between irrigation and abscess formation.7–9 However, a recent study by LaPlant et al. introduced a technique of serial small aliquot irrigations (50 mL) with immediate aspiration for a total of 6 L of irrigation 10 ; this irrigation was specifically focused on the right lower quadrant, pelvis, and above the liver. With this technique, they found a significant reduction in PO-IAA; specifically, no patients undergoing this technique developed a PO-IAA.
It is unclear, however, whether it was this specific technique or rather whether the volume of irrigation was the driving force that resulted in the decreased incidence of PO-IAA. In addition, no large-volume studies have specifically addressed whether volume of irrigation has an effect on development of PO-IAA, and most studies uniformly treat irrigation as a dichotomous variable. A small case series from Japan did find that irrigation of 6 L completely eradicated the intraperitoneal bacterial load in patients being treated for perforated appendicitis. 11 Therefore, we hypothesize that the volume of irrigation utilized is important and, specifically, that higher volumes of irrigation will result in a lower incidence of PO-IAA.
Materials and Methods
A standardized postoperative template was developed as part of a quality improvement initiative at our quaternary freestanding children's hospital. This template (Fig. 1) was included in the postappendectomy brief operative note and consisted of multiple designators to determine whether the patient had simple or complex appendicitis. The four designators for complex appendicitis (known as “complex components”) were: diffuse fibropurulent exudate within the abdomen, an extraluminal fecalith, a well-formed abscess, or a visible hole in the appendix. In addition, this template included the amount of irrigation used during the operation. The designation of simple or complex appendicitis dictated a specific postoperative care pathway. 12 The template data, as well as age, gender, height, weight, surgeon, and operative time were collected into a database prospectively starting in February 2016. In addition, as part of the quality improvement, these patients were followed for length of stay, readmissions, development of PO-IAA, and, if present, the need for abscess drainage.
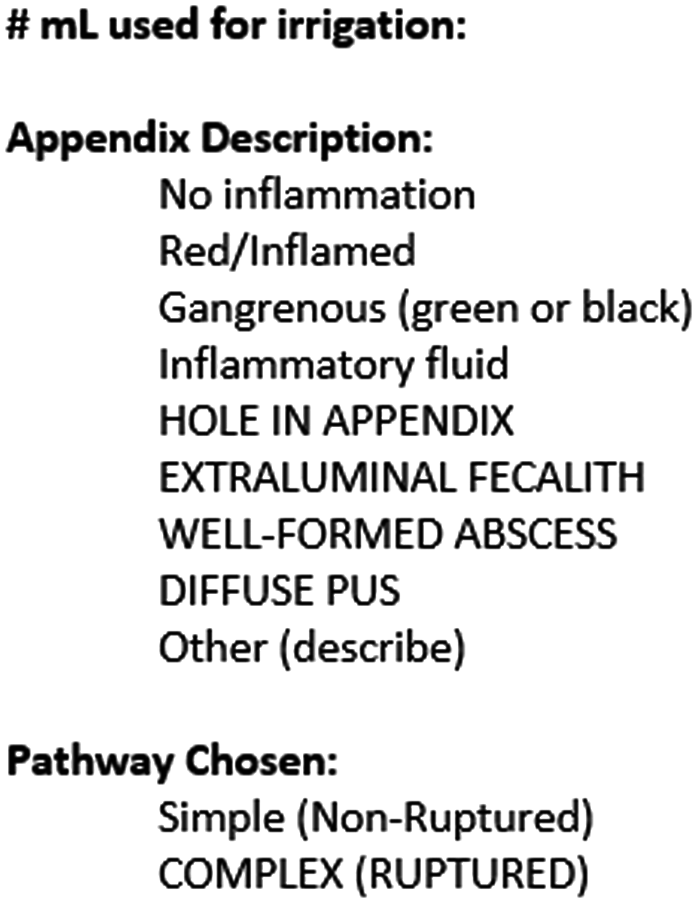
Postoperative appendicitis template. Bolded elements are to direct the operating surgeon to select the correct postoperative pathway.
We queried this database to identify all patients younger than 18 years of age with complex appendicitis from February 2016 to December 2018. We retrospectively reviewed the operative reports for patients in whom the template components were missing to minimize missing data elements. If volume of irrigation remained a missing element, we removed the patient from the dataset. Any patient undergoing interval appendectomy for complex appendicitis was also removed. This study was deemed exempt from Institutional Review Board review, as it is part of an ongoing quality improvement initiative.
Within our institution, the volume of irrigation fluid used and the technique utilized for irrigation is left to the discretion of the operating surgeon. However, most of the surgeons prefer localized irrigation of the right lower quadrant, pelvis, and above the liver.
Univariate analysis, including box and whiskers plots, was utilized to determine significant outliers and normality of continuous variables. Normally distributed continuous data were analyzed by using parametric tests (i.e., Student t-test). Non-normally continuous data were analyzed with nonparametric tests (i.e., Wilcoxon rank-sum test, Kruskal–Walis test). Categorical variables were compared with a chi-square analysis. Volume of irrigation was divided into categories based on 500-mL increases and analyzed with a Cochran–Mantel–Haeszel test to assess for trends. In addition, the number of complex components chosen was calculated to determine whether the increasing number of elements resulted in an increased incidence of PO-IAA. A P-chart was developed to compare the incidence of PO-IAA by surgeons with the overall mean incidence while accounting for their individual case load to assess whether they were within the institutional normal range.
Statistical significance was set as a P-value of .05. Variables with a P-value of .2 were included in initial multivariable models and assessed for collinearity. Where present, collinear variables were reduced. Backward step-wise regression was performed to finalize the multivariable model, with only variables maintaining a statistical significance of ≤.05 being included. All statistical analysis was performed by using SAS 9.4© (SAS Institute Inc., Cary, NC, USA).
Results
Univariate analysis
A total of 2306 appendicitis patients were identified within the database during the study. Of these, 408 (17.7%) were designated as complex appendicitis patients, with 384 patients with irrigation volumes recorded. The average age of the cohort was 10.3 ± 4.0 years (Table 1). A majority of the patients were male (63%). The average body mass index (BMI) was 18.3 (interquartile range, IQR: 15.8–23.3) with a body surface area (BSA) of 1.2 (IQR: 1.0–1.6).
Unadjusted Comparison of Patients Who Developed an Abscess Versus Those Who Did Not Develop an Abscess
Cochran–Mantel–Haenzel trend P-value.
BMI, body mass index; BSA, body surface area.
With regards to the complex components, the most commonly found component was a hole in the appendix (271 patients, 77.4%), followed by diffuse fibropurulent exudate (170 patients, 44.3%). A majority of the patients were found to have either one or two of the complex components (173 patients and 170 patients, respectively). Most patients (92.7%) were irrigated at the time of their operation with an average volume of 1000 mL (IQR: 500–2500).
Fifty-three patients developed a PO-IAA for an overall incidence of 13.8%. Forty percent of patients with a PO-IAA were diagnosed by computed tomography alone, 33% by ultrasonography, and 27% underwent both ultrasonography and computed tomography as part of their diagnostic evaluation for PO-IAA. Of these, 31 patients (59.6%) underwent interventional procedures for drainage of their PO-IAA. No patients required a return to the operating room for drainage or any other complications or sequela.
The average length of stay for complex appendicitis patients was 4.8 days (IQR: 3.1–6.5). Seventeen patients were readmitted (5.1%), of whom 8 had a readmission diagnosis of PO-IAA. The second most common reason for readmission was persistent abdominal pain.
Bivariate analysis
When comparing individuals who developed an abscess with those who did not, there was no difference in age, gender, or BSA (Table 1); however, the abscess cohort had a higher BMI (20.3 versus 17.8, P = .05). No individual complex component reached significance for the development of a PO-IAA.
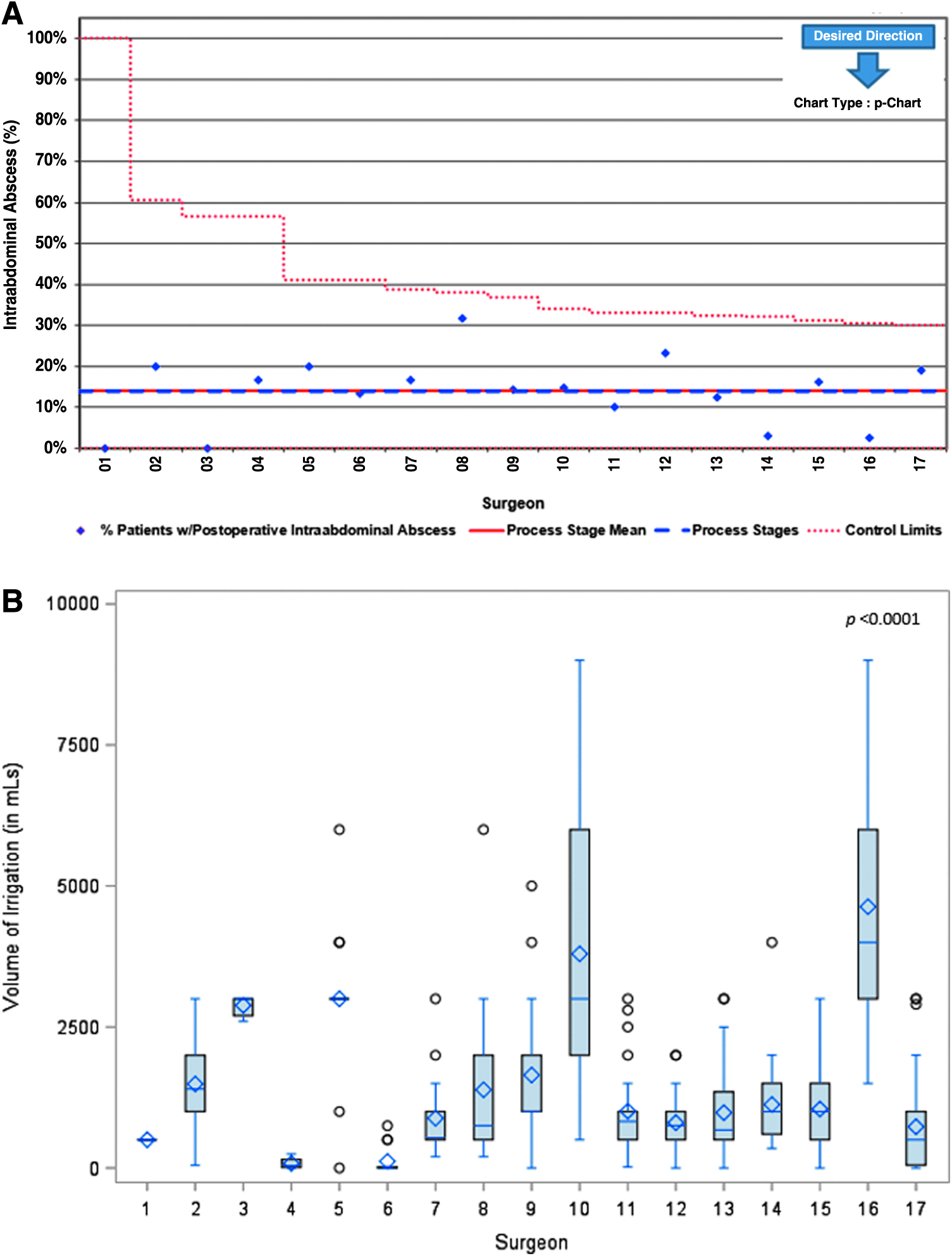
There was a significant correlation between a visualized hole in the appendix and both the presence of an extraluminal fecalith (P = .03) and the presence of a well-formed abscess (P < .0001). The presence of a well-formed abscess was also highly correlated with the presence of diffuse fibropurulent exudate (P < .0001). There was no trend for increased incidence of PO-IAA formation, with an increasing number of complexity components found at the index operation (P = .33). The operating surgeon was not associated with the development of PO-IAA (P = .32; Fig. 2).
The use of any irrigation did not correlate with the development of PO-IAA (P = .97) and neither did the volume of irrigation utilized (P = .34; Fig. 3). This did not change when the volume of irrigation was assessed as milliliters per BMI or milliliters per BSA. There was no significant difference in the incidence of PO-IAA formation based on volume of irrigation when accounting for total number of complex components present (P = .30; Fig. 4).
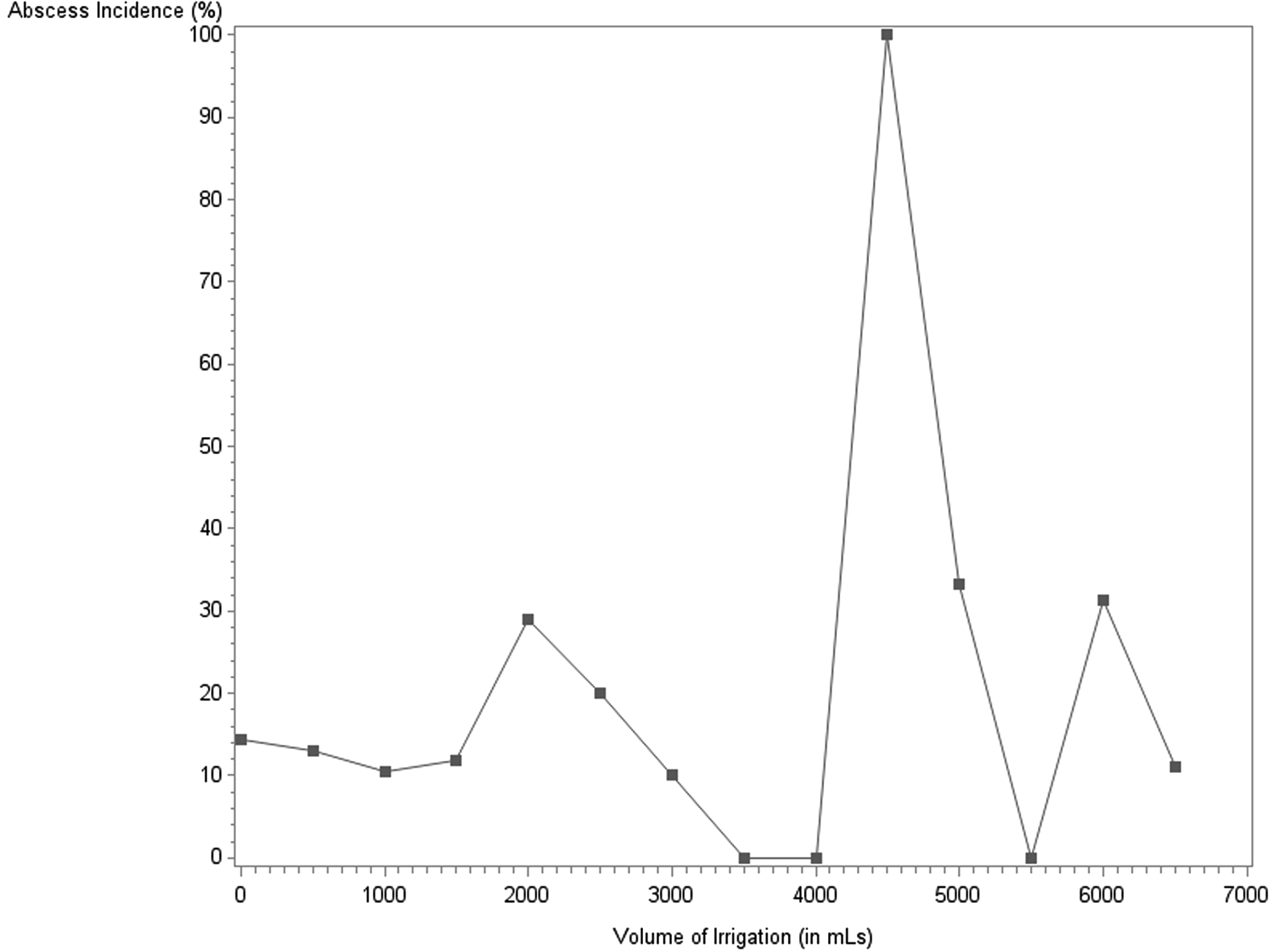
Incidence of postoperative intraabdominal abscess formation by volume of irrigation (in mL) used at the time of surgery. It should be noted that only two individuals had irrigation volumes of 4500 mL, both of whom developed an abscess; this value is not outside the expected due to the low number of cases within this category.
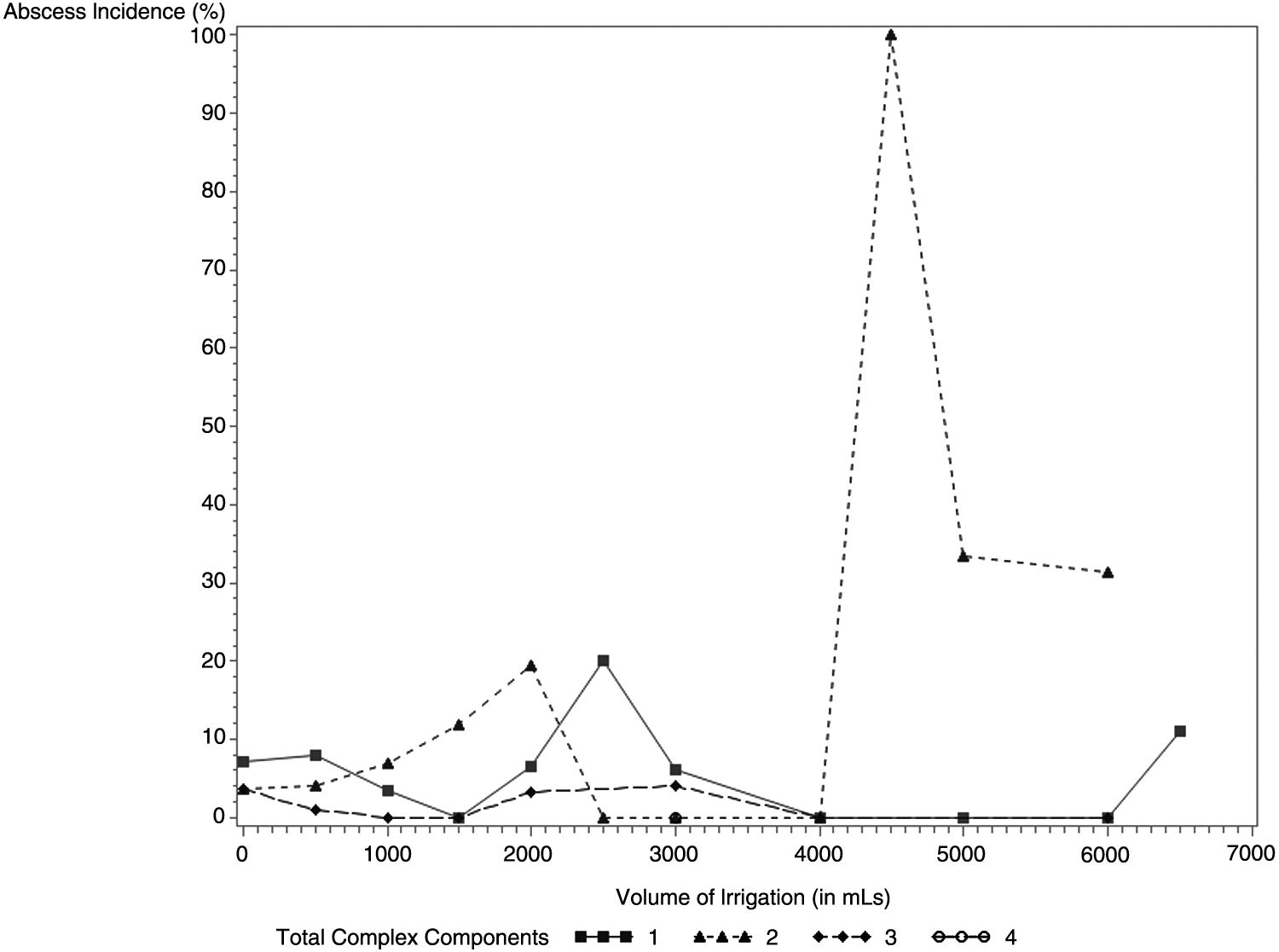
Incidence of postoperative intraabdominal abscess formation by volume of irrigation (in mL) used at the time of surgery, when accounting for the number of complex components present.
Length of stay was significantly longer in those patients who developed a PO-IAA (10.1 days versus 4.3 days, P < .0001). In addition, they had a higher incidence of readmission (17% versus 2.5%, P < .0001), with 63.6% being readmitted due to abscess formation versus 12.5% of those without a PO-IAA (P = .03).
Factors associated with volume of irrigation
The presence of diffuse fibropurulent exudate found at the time of the index operation was significantly associated with higher volumes of irrigation (1500 mL versus 1000 mL, P = .002). In addition, as the total number of complex components increased, the volume of irrigation increased from 1000 L if only one or two complex components were present to 2900 mL if all four were present (P = .03). Increasing age was associated with increasing volumes of irrigation (P = .05); however, increasing BMI and BSA were not (P = .33 and P = .08, respectively). The only other variable significantly associated with volume of irrigation was operating surgeon (P < .0001) and was found to be highly variable (Fig. 4). In a multivariable linear regression model, the variables just mentioned remained significantly associated with volume of irrigation (P < .0001).
Discussion
We were unable to find any correlation between development of PO-IAA and any variable. Specifically, we found no correlation between the presence of an extraluminal fecalith and PO-IAA. This is in contrast to a study by Henry et al. that found the presence of an extraluminal fecalith and preoperative diarrhea to be the only factors associated with PO-IAA formation. 1 Further, we did not find that increasing contamination, as calculated by total number of complex components selected, was associated with an increased incidence of PO-IAA. Anandalwar et al. recently reported that increasing complexity was associated with increased risk of postoperative surgical site infection based on merged National Surgical Quality Improvement Project (NSQIP) and the Pediatric Health Information System (PHIS) data; they used the same four variables to define complexity. 13 In their study, they found that the presence of all four variables resulted in a 27.2% risk of developing a PO-IAA as compared with a 7.5% risk for the presence of a fecalith alone.
Interestingly, we did find that increasing complexity was associated with increased volume of irrigation. Since volume of irrigation does not affect the incidence of PO-IAA, this leads us to believe that surgeons tend to irrigate with higher volumes when the field appears more infected.
In spite of the finding by Ohno et al. that 6 L of irrigation effectively eradicated the intraperitoneal bacterial load and the findings by LaPlant et al. that irrigation of a small aliquot up to 6 L resulted in no PO-IAA formation, we were unable to find a correlation between the volume of irrigation and PO-IAA.10,11 This may be due to theories that have been previously put forth and nicely summarized by St. Peter et al. that irrigation is ineffective due to the adherence of the organisms to the peritoneal lining, that fecal contamination is resistant to intraperitoneal lavage, and that irrigation can lead to remote inoculation.2,14–16 In addition, they related that although previous studies had shown that irrigation may remove or dilute phagocytes from the peritoneal lining, there has been no documented decrease in overall activity of the phagocytes.17,18 Therefore, they felt that irrigation only led to a transient decrease in bacterial load within the peritoneal cavity and did not affect the eventual formation of intraabdominal abscess.
In addition, we found that nearly 93% of all our complex appendicitis patients underwent some degree of irrigation. This is very consistent with the findings of Muehlstedt et al., who found in their survey of U.S. pediatric surgeons that 91% reported using irrigation during an operation for appendicitis. 19 Interestingly, this study was performed after previous studies showing either increased abscess formation or equivocal findings.5–9 This leads us to believe that the bias to the historical teaching of irrigation continues to permeate our present treatment.
One of the limitations of this study is the missing data. Although the missing data are minimal, it is our view that the missing data within this study are missing completely at random and are independent of the observed and unobserved data; therefore, it should not lead to bias within the analysis. Further, although the volume of irrigation was available through our template postoperative notes, this does not capture the technique of irrigation; these data were not readily available in a majority of the operative reports and are not standardized at our institution. Therefore, it is impossible to determine whether technique of irrigation has an impact on PO-IAA formation. In addition, due to confounding of the volume of irrigation and the number of complex components, it is difficult to elucidate the true relationship between irrigation and the development of PO-IAA in these complex patients and what the effect of no irrigation would have.
Another limitation to the study is that although our institution used the standard NSQIP definitions for complex appendicitis, the designated components to determine complexity are selected by the surgeon and open to interpretation. Although the presence of a fecalith and a visible hole in the appendix are relatively objective findings, the determination of a well-formed abscess and diffuse fibropurulent exudate are more subjective. However, Anandalwar et al. postulated that diffuse fibropurulent exudate was likely due to a greater extent of peritoneal contamination, and thus a higher burden of residual biofilm postoperatively. 13 They also stated that well-formed abscesses represented a longer duration of disease, and thus a more established biofilm.
Therefore, it is possible that the high collinearity between these variables is a product of not only the subjective nature of description but also the duration of the illness. It is feasible that patients with a longer duration of disease initially had diffuse fibropurulent exudate, which is evident on initial exploration, but that it was also more likely for areas of this exudate to coalesce into well-formed abscesses. However, the reason for the correlation between these two findings remains speculative and the pathophysiology is not truly defined.
In conclusion, the volume of irrigation is highly associated with the surgeon performing the operation, the presence of diffuse purulent fluid found intraoperatively, and the age of the patient. However, volume of irrigation does not impact the development of PO-IAA and the use of irrigation should be deferred to the operating surgeon.
Footnotes
Authors' Contributions
Study design: K.B.S., B.D.K.; Data collection: K.B.S., R.S., M.W.D.; Data analysis: K.B.S.; Data interpretation: K.B.S., B.D.K.; Drafting of the original article: K.B.S., B.D.K.; Article revisions: K.B.S., R.S., M.W.D., K.A.D., G.E.B., B.D.K.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.