
Abstract
Aim:
To assess nonoperative management (NOM) of uncomplicated appendicitis (UC-appy) in children to determine factors influencing prognosis and review the literature.
Materials and Methods:
All UC-appy cases presenting younger than 16 years between 2015 and 2018 who had NOM (one dose of intravenous analgesia and intravenous piperacillin/tazobactam 112.5 mg/kg 8 hourly) and were followed up for at least 3 months were reviewed prospectively (n = 146). Perceived pain and fever were assessed 12 hourly, biochemistry daily. If predetermined cutoff results were not achieved at each assessment, NOM was abandoned and urgent laparoscopic appendectomy (ULA) performed.
Results:
NOM succeeded in 48.6% (S-NOM; n = 71) and failed in 51.4% (F-NOM; n = 75). Mean age at presentation (10.7 ± 2.5 versus 8.6 ± 3.7 years old; P < .0001) and duration of preadmission fever (1.0 ± 0.9 versus 2.1 ± 1.2 days; P < .0001) were the only significantly different criteria between S-NOM and F-NOM. Optimal cutoff values using receiver operating characteristic curve analysis were 7.0 years old (32% sensitivity and 93% specificity) and 1.0 day (95% sensitivity and 25% specificity), respectively. NOM was abandoned for persistent pain, prolonged fever, or raised white blood count at 12 hours in 20/75 (26.7%), 24 hours in 31/75 (41.3%), 36 hours in 14/75 (18.7%), and 48–72 hours in 10/75 (13.3%). At ULA, perforation was identified in 14/75 (18.7%). Complications arising within 3 months of ULA were residual abscess (n = 7/75; 9.3%) and transient ileus (n = 1/75; 1.3%).
Conclusion:
It would appear that surgery may be more appropriate for children with UC-appy when they are younger and febrile before admission for longer.
Introduction
Reported success rates of nonoperative management (NOM) for uncomplicated appendicitis (UC-appy) in adults have approached 90% in the short term and 75% overall, with no long-term sequelae and minimal reported risk for perforation.1,2 In fact, several recent European randomized controlled trials have even concluded that therapy with antibiotics alone is a safe treatment option for UC-appy in adults.2–4 However, while initial NOM for perforated appendicitis has been well reported in children, and has been shown to be equivalent to more conventional treatment in efficacy, NOM for early UC-appy in children has not been the subject of specific research until very recently.
We report a study of UC-appy in children to establish the type of patient best suited for NOM and assess factors that may influence outcome.
Materials and Methods
All children younger than 16 years who presented with clinical signs and symptoms of acute UC-appy between 2015 and 2018 and followed up for at least 3 months after treatment were eligible for enrollment in this trial. Exclusion criteria included presence of any complication of acute appendicitis, such as abscess formation, or evidence of perforation on imaging studies such as ultrasonography (US) and computed tomography (CT), as well as presence of significant comorbidities.
Diagnosis of appendicitis was made by using a combination of “basic” strategies: history taking, physical examination, blood tests, and abdominal US. If a definitive diagnosis could not be made using basic strategies, a CT scan was performed. All US examinations were performed by pediatric radiologists using a maximum diameter of >6 mm as the diagnostic criterion for acute appendicitis.
All patients diagnosed with UC-appy were admitted to the surgical ward for NOM (one dose of intravenous analgesia after assessment and then piperacillin/tazobactam: 112.5 mg/kg administered intravenously 8 hourly). Oral intake was not restricted specifically. Blood samples were taken every 24 hours. Progress of NOM was determined by assessing standard clinical criteria and if there was no improvement, NOM was abandoned and urgent laparoscopic appendectomy (ULA) was performed within 6 hours. Clinical criteria used were as follows: perceived abdominal pain assessed every 12 hours using a scale where 10 was the level of pain at presentation; body temperature assessed every 12 hours; and laboratory data assessed every 24 hours (Table 1). Any recurrences after successful NOM (S-NOM) had emergency LA (ELA). Outcome in all patients was assessed at least 3 months after S-NOM or failed NOM (F-NOM).
Criteria Determining Failure of Nonoperative Management
NA, not available; WBC, white blood count.
All data were collected prospectively, and were analyzed using standard statistical methods. Frequency tables for categorical variables were calculated, along with the mean ± standard deviation or the median (interquartile range) for continuous variables. Logarithmic transformation was applied to clinical data, such as white blood count (WBC) and C-reactive protein level for comparison. We used the t-test for comparison of two groups with continuous variables, and the Fisher exact test was applied for categorical variables. Because pain and duration of fever were not distributed normally, a nonparametric test, the Mann–Whitney U test, was used. Failure or success of antibiotic treatment was categorized as a binary event. The receiver operating characteristic (ROC) curve analysis and the area under the ROC curve (AUC), a measure of a test's diagnostic accuracy were conducted. The diagonal line is called “line of no information” as it reflects a sensitivity and specificity of 50% point. The Youden Index was used to determine different cutoff values. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated. All analyses were conducted using SAS 9.4 (Cary, NC). This study was approved by the institutional review board of Juntendo University School of Medicine.
Results
In total, 146 subjects were enrolled in this study. NOM was successful (S-NOM) in 48.6% (n = 71) and failed (F-NOM) in 51.4% (n = 75). Gender ratios (S-NOM versus F-NOM; 61.9% male versus 53.3% male); mean maximum fever: 38.1 ± 0.7°C versus 38.1 ± 0.7°C; presence of rebound tenderness: 67.6% versus 66.6%; WBC: 14,950 (range: 11,250–17,020) versus 14,000 (range: 11,300–17,200)/μL; CRP: 4.1 (range: 2–8) versus 5.4 (range: 2.5–9.3) mg/dL; size of the appendix: 9.4 ± 2.9 versus 9.6 ± 2.8 mm; presence of an appendicolith: 41.4% versus 41.3%; and duration of preadmission pain: 1.9 ± 1.1 versus 1.8 ± 0.9 days, were similar for both groups. Only differences in mean age at presentation and duration of preadmission fever were statistically significant; 10.7 ± 2.5 years old (S-NOM) versus 8.6 ± 3.7 years (F-NOM) and 1.0 ± 0.9 days (S-NOM) versus 2.1 ± 1.2 days (F-NOM) (P < .0001, respectively) (Table 2). ROC curve analysis showed that 7.0 years old (32% sensitivity and 93% specificity) and 1.0 day (95% sensitivity and 25% specificity) were the optimal cut off values for age at presentation and duration of preadmission fever, respectively. The AUC for Youden index was 0.587 (95% confidence interval [CI]: 0.493–0.681) and 0.599 (95% CI: 0.511–0.688) for age at presentation and the duration of fever, respectively as in shown in Figure 1.
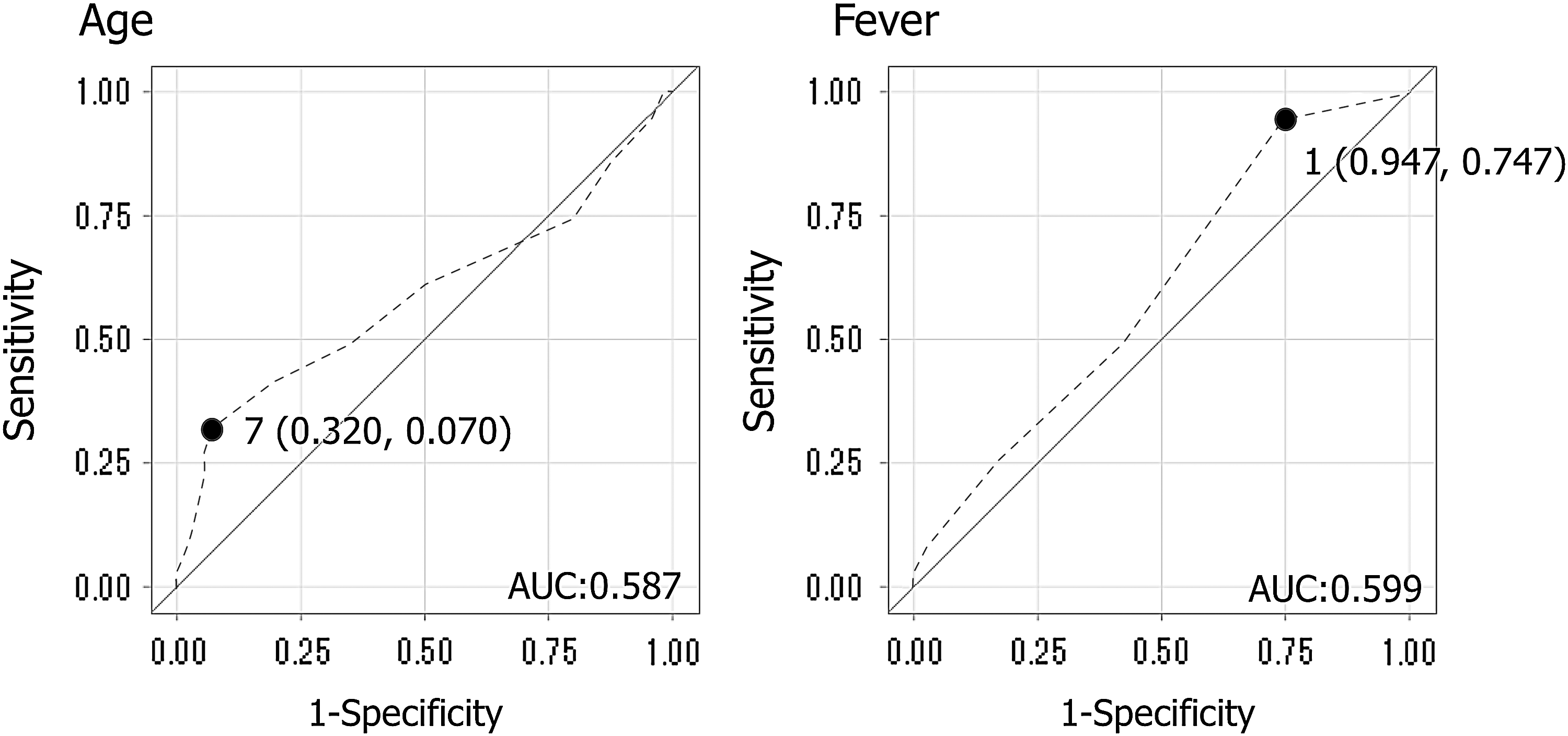
ROC curves for predictive factors in patients with suspected acute appendicitis. The cutoff value is given in parentheses. ROC curve analysis showed that 7.0 years old (32% sensitivity and 93% specificity) and 1.0 day (95% sensitivity and 25% specificity) were the optimal cut off values for age at presentation and duration of preadmission fever, respectively. The area under the ROC curve was calculated as the Youden Index; 0.587 and 0.599 for age at presentation and duration of fever, respectively. ROC, receiver operating characteristic.
A Comparison of Factors Affecting the Outcome of Nonoperative Management in Uncomplicated Appendicitis Cases (n = 146)
CRP, C-reactive protein; NOM, nonoperative management; WBC, white blood count.
In F-NOM, NOM was abandoned at 12 hours in 20/75 (26.7%) for pain in 20/20, at 24 hours in 34/75 (45.3%; for persistent pain in 26/34 and raised WBC in 8/34), at 36 hours in 11/75 (14.6%; for persistent pain in 7/11 and prolonged fever in 4/11), at 48 hours in 4/75 (5.3%; for persistent pain in 1/4, prolonged fever in 2/4, and raised WBC in 1/4), at 60 hours in 2/75 (2.6%; for persistent pain in 1/2 and prolonged fever in 1/2), and at 72 hours in 4/75 (5.3%; for persistent pain in 2/4, persistent fever in 1/2, and raised WBC in 1/2). If multiple cause of failure was identified, the most severe factor was chosen as the cause of failure. All F-NOM had ULA. Of these, 14/75 (18.7%) were found to be perforated at ULA. Post-ULA sequelae arising within 3 months were as follows: residual abscess (n = 7/75; 9.3%) and transient ileus (n = 1/75; 1.3%). Two residual abscess required CT-guided percutaneous drainage; the rest resolved spontaneously. One S-NOM case required emergency LA 2 months after S-NOM.
A summary of a review of the English language literature for studies evaluating NOM for UC-appy in children is shown in Table 3.5–17 The success rate of NOM in this study (48.6%) was lower than in other reports (83.3%–98.7%). There were no reports that presented detailed protocols for NOM or antibiotic administration with clear definitions of success or failure apart from our study. In fact, four reports were just presentations of protocols, and if these were excluded, there was only one study that included every noncomplicated appendicitis patient assessed. Every other study excluded patients arbitrarily, for example, for being symptomatic for a too long time before presentation, because of appendicolith, because of severe signs of inflammation, or because of large diameter appendixes.
Literature Review of Studies About Nonoperative Treatment for Uncomplicated Appendicitis in Children
Preclinical trial study presenting a planned protocol.
ABPC/SBT, ampicillin/sulbactam; AMPC/CVA, amoxicillin/clavulanic acid; ABTx, antibiotics; BSA, broad spectrum ABTx; CAZ, ceftazidime; CMZ, cefmetazole; CPFX, ciprofloxacin; CPZ, cefoperazone; CTRX, ceftriaxone; GM, gentamicin; IMPM/CS, imipenem/cilastain; MEPM, meropenem; MNZ, metronidazole; NA, not available; PIPC/TAZ, piperacillin/tazobactam; UNK, unknown.
Discussion
In contrast to reports about adult NOM, there are very few reports assessing NOM for UC-appy in children, which is one reason we chose to conduct this study. On the other hand, studies of NOM for perforated appendicitis in children are extremely optimistic, reporting lower complication rates, fewer abscesses, and a trend for shorter hospitalization 18 ; Nazarey et al. 19 reported that, almost 90% of their subjects completed NOM; other published series have reported success rates of 62%–95%.18,20,21 Thus, it would appear that most patients with perforated appendicitis respond very well to NOM.
Obviously, if there is evidence that NOM is effective in children, there could be savings made on health care costs as well as less reliance on emergency surgery as the primary form of surgical intervention. Several centers have embarked on pilot studies in the last few years based on successful adult studies, with encouraging results, such as NOM being successful for treating UC-appy in 93.7%, 83.3%, 93.3%, and 98.7%, including pediatric patients, respectively.13,16,22,23 However, the success rate of NOM for UC-appy in this study in children was lower than expected and we postulate that this may be related to the fact that there is usually some degree of delayed presentation with children either because children cannot explain themselves adequately or parents are hoping for the best and leave things to the last minute. Thus, in contrast to adult studies, children tend to take longer to present after the first onset of symptoms, and the stress this causes is clearly shown by the statistically longer duration of preadmission fever in the F-NOM group compared with S-NOM, yet duration of abdominal pain was similar for both groups. This would suggest that fever, which is an objective evaluation factor, more accurately reflects the clinical status of a child than pain, which is a subjective evaluation factor.
The success of NOM and whether it is valid to continue it in uncertain cases depend entirely on the protocol used to choose patients for NOM and abandon NOM when it is failing. A protocol must be based on strictly defined cutoff levels for test results and clinical symptoms and signs to enhance recovery in patients who are responding and identify patients who are deteriorating before they are seriously unwell and not likely to tolerate surgery. Some may argue that our protocol is too rigorous, but we believe a protocol should be strict with no room for interpretation, otherwise consistency varies. Sadot et al. emphasized the importance of acquiring an accurate history, including the exact time symptoms began. 24 We also believed this to be important and placed strong emphasis on preadmission status because the longer a child is not treated before presentation means more physical/psychological stress and less reserve. Perceived perception of abdominal pain is a valid criterion and 24–72 hours should be the maximum time to observe a child to determine if NOM is to be continued or abandoned.25,26 Thus, our protocol includes presence or absence of fever, quality of pain, and laboratory data as basic criteria for reviewing clinical status 12 hourly after admission in all cases.
All published studies to date have serious shortcomings; such as ambiguous definitions for success/failure of NOM for UC-appy, not presenting NOM protocols in detail, changing antibiotics without good reason, and excluding some UC-appy cases because they “appeared” worse than their clinical data that indicated they were suitable for NOM. Typical of excluded cases were children who had been symptomatic for an extended period before presentation, children with an appendicolith, blood test results that were “better” than expected from the clinical assessment, or a hugely dilated appendix (Table 3). The better success rates in the literature may be related to these exclusions. In other words, other studies were conducted using “selected” patients, whereas our study involved “all” UC-appy patients.
Although recent publications have reported on the safety of antibiotics as first-line treatment for appendicitis, they insist that there are independent risk factors for deterioration in appendiceal pathology, including younger age, elevated body temperature, and delayed medical attention (i.e., more than 48 hours from the onset of symptoms to presentation or more than 24 hours from urgent admission to surgery).2,27 Whyte and Tran determined that the white cell band count on presentation, body temperature response during the first 24 hours of admission were most helpful for predicting the initial risk for problems with NOM. 28 Interestingly, our study showed a similar pattern with 68.0% of F-NOM patients having NOM abandoned between 12 and 24 hours after admission because of deterioration in perceived abdominal pain or prolonged fever, while only 13.3% of F-NOM patients had NOM abandoned 48 hours after admission. In other words, the reaction to NOM was early in both groups, with S-NOM patients who did well tending to respond early to NOM and F-NOM patients who did not do well, deteriorating early as well. In contrast, there were fewer patients in F-NOM who had NOM abandoned after 48 or 72 hours.
Parents were extremely interested in this study, with 100% of families agreeing to participate when asked. Because all participating families were enthusiastic about this study, we believe the data obtained are accurate and our findings reliable. The design of this study, where all patients had NOM, actually minimized selection bias and contributed to the validity of our results by controlling variables. Thus, differences in outcome could be attributed directly to patient status.
In conclusion, duration of preadmission fever and age at presentation were significantly different in F-NOM, so by triaging only children with UC-appy older than 7 years or who were febrile for <2 days for NOM, and children 6 or younger or who were febrile for more than 2 days for surgery, we may have a simple way to manage UC-appy objectively.
Future research will use the findings of this study to create different groups of UC-appy patients, classified according to age at presentation and duration of preadmission fever to assess what extra factors may be relevant to help improve the failure rate of NOM.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.