
Abstract
Abstract
Background:
Laparoscopic inguinal hernia repair (LIHR) is increasingly widely accepted in pediatric surgery. However, reoperation risks remain unknown. We summarized our single-center experience with reoperations after laparoscopic percutaneous extraperitoneal closure (LPEC) and single-incision LPEC (SILPEC).
Materials and Methods:
We retrospectively reviewed reoperation cases of hernia repair greater than or equal to two times between 2000 and 2018, wherein the first hernia repair was performed laparoscopically. Primary outcomes were recurrence type and screening sufficiency for contralateral patent processus vaginalis (cPPV). Secondary outcomes were associated with details of recurrences.
Results:
Of the 2112 patients who underwent LPEC/SILPEC, 14 (recurrence rate = 0.7%) showed recurrences after treatment and 8 (incidence rate = 0.4%) showed contralateral metachronous inguinal hernia (CMIH). Concerning the primary outcome of recurrence type, the orifice was inside the previous ligation (Inside group), suggesting loosened first ligation, in 6 (42.9%) patients and outside the previous ligation (Outside group) in 7 (50.0%); and 1 (7.1%) patient showed no orifice. Regarding CMIH, 3 (37.5%) patients were suspected of insufficient screening for cPPV, 1 (12.5%) underwent sufficient screening, and 1 (12.5%) had cPPV but treatment was deemed unnecessary. Concerning secondary outcomes, 4 (66.7%) and 6 (85.7%) patients from the Inside and Outside groups were treated with single ligation, respectively. One patient from the Outside group (14.3%) had a massive peritoneum injury during the first operation.
Conclusions:
Some preventable factors, such as loosened ligation, torn peritoneum, and use of single ligation in recurrences and insufficient screening for cPPV in CMIH, were observed. These should be taken care to prevent reoperations in LIHR.
Introduction
Inguinal hernia repair is one of the most common procedures in pediatric surgery, and laparoscopic repair is increasingly gaining popularity in pediatric surgery. Various procedures are now reported. We adopted laparoscopic percutaneous extraperitoneal closure (LPEC) 1 at our institution in 2007, and single-incision LPEC (SILPEC) 2 has become a standard procedure since 2009.
The recurrence rate after laparoscopic inguinal hernia repair (LIHR) in children is 0.2%–5%.3,4 Several studies have reviewed the risks of recurrences,5,6 but specific solutions remain unknown.
The objective of this study was to summarize our single-center experience with reoperations after LPEC and SILPEC in children and evaluate the causes.
Materials and Methods
Study design
We retrospectively reviewed hernia repair cases between 2000 and 2018 and searched for reoperation cases wherein repair was performed two times or more at the Saitama Children's Medical Center. We included the cases wherein the first hernia repair was performed laparoscopically. Reoperation cases from other hospitals, that is, cases where the first operation was performed in other hospitals, were excluded.
The study protocol complied with the Declaration of Helsinki and was approved by the Research Ethics Committee of Saitama Children's Medical Center. The requirement for written informed consent was waived because of the retrospective nature of the study.
Surgical procedures
We adopted LPEC or SILPEC as LIHR procedures.
LPEC was introduced by Takehara in 1995 and reported in 2006. 1 Because of its simplicity and effectiveness, LPEC is accepted widely in Japan 3 and was introduced at our center in 2007. Under general anesthesia, we first introduced the first trocar in the umbilicus by the open method. 7 After this, we insert another trocar below and outside the umbilicus. Using a 19-gauge LPEC needle (Lapaherclosure™; Hakko Medical Co., Nagano, Japan) with assisting laparoscopic forceps, we encircled the hernial orifice extraperitoneally with a nonabsorbable braided suture (2-0 polyester fibers; Wayolax, Matsuda Ika Kogyo Company, Tokyo, Japan), ensuring to avoid involving the vas deferens and spermatic vessels in male patients.
SILPEC was developed to reduce the invasiveness of LPEC. 2 Unlike LPEC, in SILPEC, we made a stab wound to pass through the muscle layer through the same umbilical incision just below the first trocar. We then inserted 3 mm curved laparoscopic forceps through the stab wound directly without a trocar. SILPEC was introduced at our institute in 2009; since then, we have been performing SILPEC as a standard therapy for inguinal hernia in children.
LPEC or SILPEC were performed for both inguinal hernia and hydrocele. In hydrocele cases, the hydroceles were punctured from the scrotum for drainage after the operation, if necessary.
Single ligation was used in patients with inguinal hernia aged <5 years. Double ligation was used in patients with inguinal hernia aged >5 years and patients of any age with hydrocele. Some patients aged <5 years with inguinal hernia who were suspected to be at a high risk of recurrence by the surgical team were treated with double ligation; however, we did not have strict criteria for the treatment.
We also observed the inguinal ring on the asymptomatic side to detect contralateral patent processus vaginalis (cPPV). In case we found cPPV, we performed prophylactic surgery to prevent contralateral metachronous inguinal hernia (CMIH).
All operations were performed with at least 1 attending pediatric surgeon. We did not usually use prophylactic antibiotics in LPEC and SILPEC, other than for some patients with special considerations of infections, such as patients with congenital heart disease, those using steroids, and those with immunodeficiency.
Data collection
We collected data on clinical characteristics of patients including age, sex, symptoms, comorbidities, and postoperative complications. Available surgical videos were checked for operative management. Laterality, number of ligations, types of sutures, and sufficiency of screening for cPPV were assessed using the videos of the first operation, and the videos of reoperations were used to check for the types of recurrence. For recurrent cases, we measured the width of the hernial orifice during the first operation by a comparison with the width of laparoscopic forceps (3 mm in diameter) through the videos, and defined the orifice as enlarged when it was assumed to be larger than four times the width of the forceps, 12 mm. In addition, we evaluated major peritoneum injury defined as a large peritoneal laceration that could not be repaired.
With regard to screening for cPPV, all authors checked the surgical videos to determine whether the screening was performed sufficiently.
The primary outcomes were type of recurrence and sufficiency of screening for cPPV. Types of recurrence were judged through the videos of reoperations and sufficiency of screening for cPPV was evaluated through videos of the first operation. The secondary outcomes included the details of the recurrent cases.
Statistical methods
Categorical variables are presented as number (%) and continuous variables are presented as median (range). Because there were few previous reports or sufficient hypotheses to test, we aimed to observe and report our surgical experience. Therefore, we did not test a specific hypothesis or compare the results. Statistical analyses were performed using R ver3.3.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 2112 patients underwent LPEC or SILPEC at our hospital. Bilateral symptomatic inguinal hernia and repair were found in 135 patients, whereas 1977 patients had unilateral symptomatic inguinal hernia, of which 783 (39.6%) had cPPV and underwent prophylactic repair. Twenty-two cases (1.0%) were judged as reoperation cases: 14 cases (recurrence rate = 0.7%) showed recurrences after treatment for the preoperative symptomatic side and 8 (incidence rate = 0.4%) showed CMIH, which was not treated during the first hernia repair. Recurrence after treatment for cPPV was not observed.
Patient characteristics are given in Table 1. Of the 14 recurrence cases, the male-to-female ratio was 10:4 (71.4%/28.6%), the median age during the first repair was 27.5 (8–143) months, and the median period from the first repair to recurrence was 6.5 (1–19) months. One patient (7.1%) had a history of incarceration. Emergency surgery was not performed in any patient. For the 8 CMIH cases, the median period from the first repair to reoperation was 29.5 (18–72) months. Emergency surgery was performed in 1 patient (12.5%) in this group.
Patient Characteristics for Reoperation
In this case, the surgery was performed by the open method at another hospital first, and the patient was then referred to our hospital because of accidental resection of the urinary bladder misidentified as the hernial sac.
CMIH, contralateral metachronous inguinal hernia.
Primary outcomes have are summarized in Table 2. With regard to the type of recurrence, the orifice was inside the previous ligation (Inside group), suggesting loosened first ligation, in 6 (42.9%) cases and outside the previous ligation (Outside group) in 7 (50.0%) cases. Only 1 patient (7.1%) showed no orifice (noncommunicating hydrocele). Visual findings of the Inside and Outside groups are given in Figures 1 and 2, respectively. With regard to CMIH, initial operation videos for 3 patients (37.5%) were unavailable. Three patients (37.5%) were suspected of insufficient screening for cPPV, 1 (12.5%) was sufficiently screened, and 1 (12.5%) showed a diagnosis of cPPV but was judged as unnecessary to treat. All CMIH patients underwent their first operation before 2015, and when we renewed, the system of scope and resolution was improved.
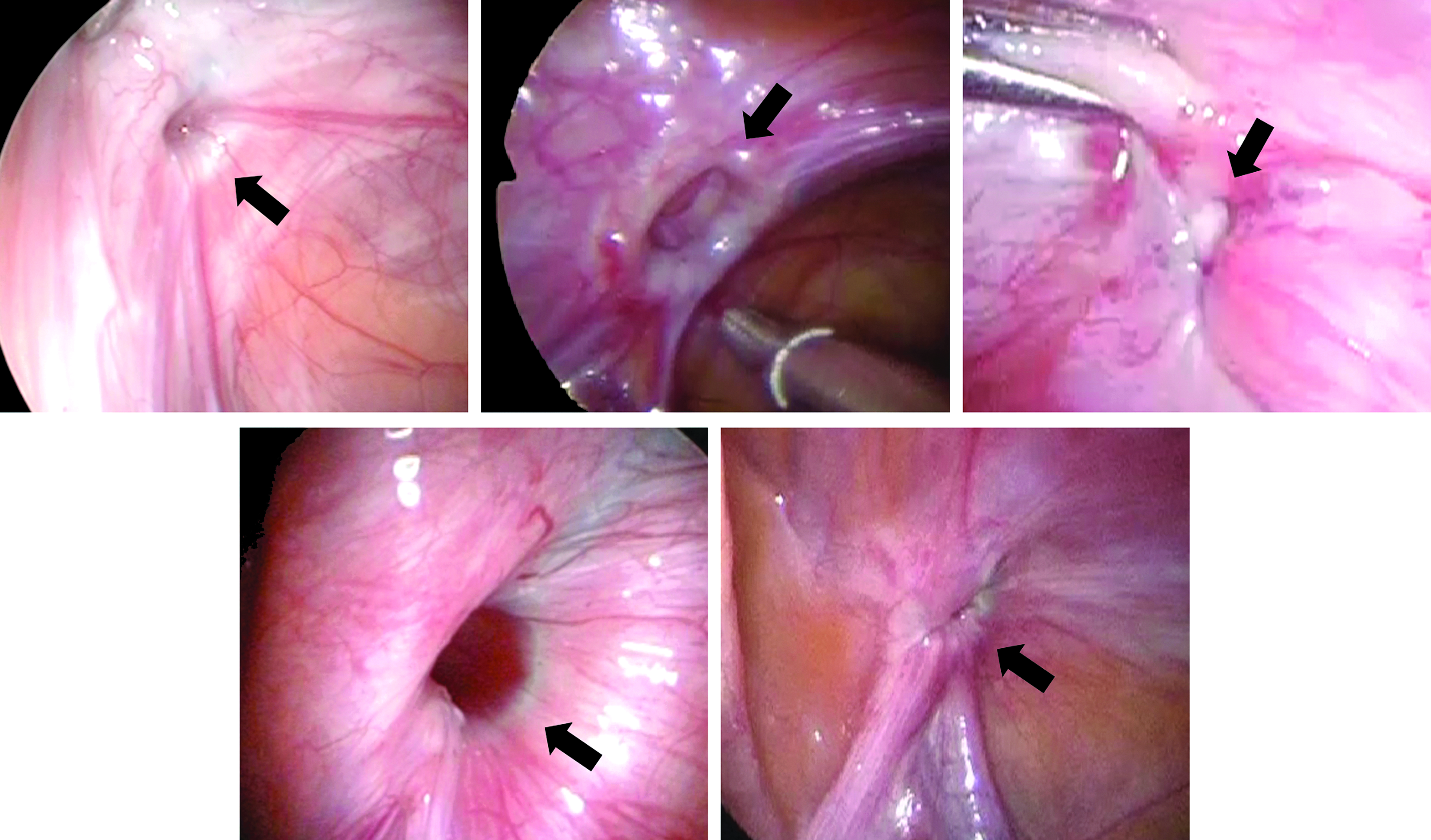
Hernial orifice found inside the previous ligation (arrows).
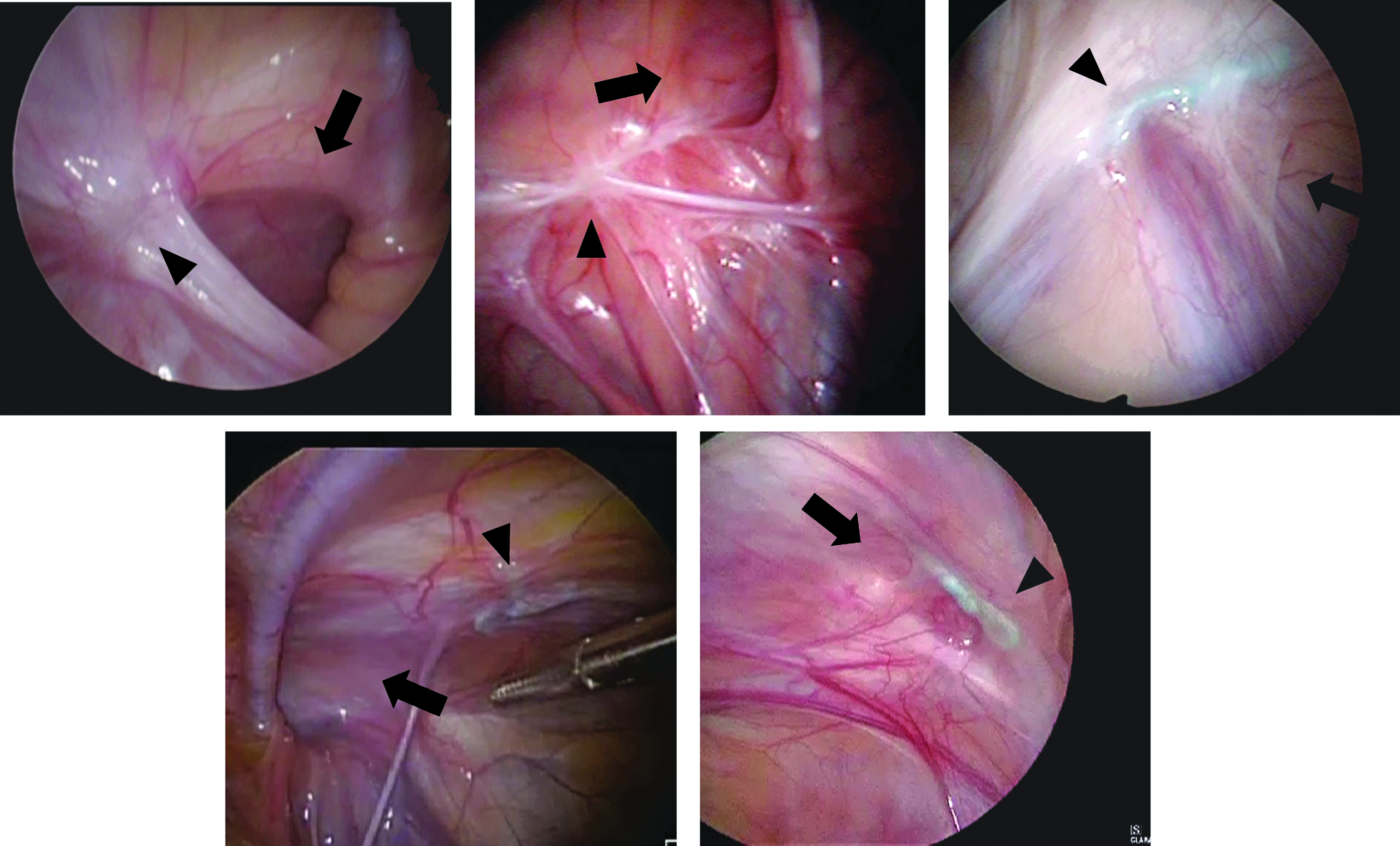
Hernial orifice (arrows) found outside the previous ligation (arrowheads).
Clinical Factors of Reoperation
One of these cases resulted from a massive injury of the peritoneum.
cPPV was found but judged as unnecessary to treat.
Videos of the first operation were unavailable for 3 patients.
CMIH, contralateral metachronous inguinal hernia; cPPV, contralateral patent processus vaginalis.
Secondary outcomes are given in Table 3. Details of recurrences were reviewed. Thirteen patients (92.9%) showed inguinal hernias and 1 patient (7.1%) showed hydrocele as their symptoms during the first operation. Eight and 6 patients (57.1% and 42.9%) had recurrences on the right and left sides, respectively. The 1 patient with no orifice was treated at the age of 143 months and presented with hydrocele at the first operation. The patients in the Inside group were treated at median 27.5 months (8–126 months), and 4 patients (66.7%) were treated with single ligation in this group; however, the patients in the Outside group were treated at 21 months (13–57 months), and 6 patients (85.7%) were treated with single ligation in this group. Four patients each in the Inside and Outside groups (66.7% and 57.1%, respectively) presented with inguinal hernia at recurrence. The median duration between the first operation and recurrence was 3 months (1–19) and 9 months (6–13) in the Inside and Outside groups, respectively. One patient in the Outside group had a massive peritoneum injury during the first operation, but the other 6 patients did not have major peritoneum injuries. Of the 6 patients, 4 had a new hernial orifice lateral to the previous ligation and 2 had a new orifice medial to the previous ligation, but all of them were outside the hypogastric vessels, that is, all were indirect hernias. Only 2 patients (28.6%) in the Outside group showed an enlarged hernial orifice at the first operation.
Details of Recurrence
Inside group: hernia orifice was found inside the previous ligation.
Outside group: hernia orifice was found outside the previous ligation.
Discussion
Summary of the results
In this study, we summarized our experience with reoperations after LIHR in children. Reoperations were divided into two groups: recurrences and CMIH. More than half of the recurrences and CMIHs were reported in male patients. The duration between first operation and reoperations seemed to be shorter in recurrences than in CMIHs. The etiologies of recurrences were categorized within the following three types: the orifice inside the previous ligation (Inside group; n = 6), the orifice outside the previous ligation (Outside group; n = 7), and no orifice (n = 1). The orifice within the previous ligation (Inside group) was thought to be caused by a loosened previous ligation. One case in the Outside group (14.3%) seemed to have been resulted from a major peritoneum injury. Many patients in the Inside and Outside groups were with single ligations. Enlarged hernial orifice was not common. With regard to CMIH, 3 cases resulted from insufficient screening. No cases on CMIH occurred after we renewed the system of scope.
Types of operative procedures (feasibility of LPEC or SILPEC)
Various procedures are reported for LIHR in children, and they are mainly divided into two approaches: intraperitoneal and extraperitoneal. Intraperitoneal procedures include the use of Z-stitches, 8 purse-string stitchs, 9 flip-flap hernioplasty, 10 division and resection of the hernia sac with 11 or without closure of peritoneal edge, 12 or inversion and ligation technique for girls. 13 Extraperitoneal approaches mainly include encircling the internal ring with sutures and percutaneous ligation. Procedures with specially designed devices to pass sutures, 14 procedures using a commercially available curved “awl,” 15 subcutaneous endoscopically assisted ligation technique (SEAL), 16 and percutaneous internal ring suturing technique (PIRS) 17 are examples of the extraperitoneal approach. The recurrence rate of laparoscopic inguinal hernia is reported as 0.2%–5%, although some studies have reported a much higher rate.3,4 One study comparing intraperitoneal and extraperitoneal procedures reported that the recurrence rates for intraperitoneal and extraperitoneal procedures were 4% and 1.3%, respectively, and were not significantly different, which was compatible with the results of other previous reports. 18 The recurrence rate decreases as surgeons gain experience with each procedure; however, extraperitoneal procedures tend to have relatively lower recurrence rates and are technically less demanding than intraperitoneal procedures.19–21
LPEC and SILPEC are extraperitoneal procedures reported to have low recurrence risks,1,3,5,22 consistent with the findings of this study (recurrence rate = 0.7%). Because all extraperitoneal approach procedures have a similar concept, the present review of reoperation cases may be meaningful for pediatric surgeons performing any extraperitoneal procedure.
Possible causes of recurrence
Although the follow-up period is short, a previous study showed no significant difference between LPEC and SILPEC with regard to recurrence. 23 Some studies reported about the risk factors of recurrence after LPEC or SILPEC. Male sex or age <1 year is reported as a risk factor for recurrence. 5 We cannot comment of male sex being a risk factor because we did not compare recurrence and nonrecurrence cases, but majority of our patients with recurrence were male patients. Our study did not show that patients younger than 1 year are more likely to have recurrence. Another previous study showed that enlarged hernial orifice or persistently elevated abdominal pressure, as observed in cough, constipation, or diarrhea, are risk factors, 6 but this study did not find enlarged hernial orifice to be a risk factor.
Our study showed that half of the patients with recurrences were categorized in the Inside group. The duration from the first operation to recurrence in the Inside group is relatively short (median duration, 3 months). Therefore, some technical errors such as loosening of the previous ligation or fat involvement may be suspected. Single ligation was followed in 66% cases in the Inside group. Double ligation may be one of the options to avoid loosening of the ligation.
In contrast, 1 case of recurrence in the Outside group was suspected to have resulted from a major peritoneum injury during the first operation because the hernial orifice during the second operation was found at the site where the peritoneum was injured during the first operation. LPEC or SILPEC inevitably result in a few small pinhole peritoneal lacerations, and these are usually not repaired. Therefore, small lacerations may not be a risk for recurrence, but massive peritoneum injury may cause recurrence. However, massive peritoneum injury leading to recurrence was only observed in 1 case; thus, massive peritoneum injury may be a rare cause of recurrence. Further studies concerning the size and frequency of peritoneal lacerations may be required for detailed understanding. For the other 6 patients, sliding of the peritoneum from the previous knot was suspected; 4 patients had a new hernial orifice lateral to the previous ligation and 2 had a new orifice medial to the previous ligation, but all of them were lateral to the inferior hypogastric vessels. Except for 1 recurrence case resulting from a massive peritoneum injury, all other cases indicated single ligation. For the Outside group and the Inside group, using double ligation may be an option to avoid recurrence. Contrary to our suspicion, only 2 cases showed a large hernial orifice in the Outside group. Whether large inguinal rings are a risk factor and require repair to prevent recurrences remain unconcluded. However, a very large number of cases with large hernial orifice will be required to evaluate this risk because the incidence of recurrence in cases with large hernial orifice is not common, and is therefore very hard to prove.
Owing to the nature of the procedure, LIHR by LPEC or SILPEC was thought of increasing the recurrence rate of hydrocele, but its recurrence rate is reported to be very low,24,25 and our study followed this trend. Only 1 case of noncommunicating hydrocele was noted; therefore, percutaneous drainage of the hydrocele at the end of the operation, if required, may be sufficient to prevent recurrence with noncommunicating hydrocele.
All recurrences occurred in a relatively short duration, median 6.5 months (1–19 months), after operation. This information may be useful for surgeons and patients when deciding follow-up periods.
Prevention of CMIH
Although the importance of repairing cPPV to prevent CMIH is still controversial,20,26,27 easy evaluation of cPPV and preventive operation for CMIH are benefits of LIHR. At our institution, we routinely perform evaluation of cPPV and perform prophylactic operations for it. Therefore, we believe that the occurrence of CMIH should be minimized and preventive measures are warranted.
Although initial operation videos for 3 of 8 CMIH patients were unavailable, 3 were thought to have undergone insufficient screening for cPPV at the first operation and 1 was diagnosed with cPPV but was judged as unnecessary to treat. These 4 cases were preventable. Insistent screening has previously been reported to decrease the incidence of CMIH. 28 Although the observation period of the previous study was 3 years at most, which is not enough considering that the median duration from the first operation to CMIH occurrence in our study was 29.5 months (18–72 months), insistent screening for cPPV is an important measure to prevent CMIH. In addition, no CMIH cases have been reported since we renewed the scope system to a higher resolution in 2015. The follow-up period is not sufficiently long, but the resolution of scope may be an important factor for diagnosing cPPV and preventing CMIH.
Limitations
This study has several limitations. First, this was a retrospective observational study. We did not compare or test any hypotheses; therefore, we cannot draw major conclusions only from this study. Further studies are needed, although conducting prospective studies may be difficult because of the extremely low incidence rate. In addition, registry studies handling large amounts of data are growing but are unable to evaluate specific causes. Thus, retrospective observational studies are still important. Second, some clinical factors were raised as possible risk factors for reoperation, such as number of ligations or sex ratio, but there may be some confounding. We need many more reoperation cases to analyze as the recurrence rates through multivariate analysis or stratified analysis.
Conclusions
We have summarized our experience with reoperations after LIHR in children through LPEC or SILPEC. Some preventable risk factors, such as loosened ligation, torn peritoneum, and use of single ligation in recurrences and insufficient screening for cPPV in CMIH, were found.
Footnotes
Acknowledgments
The authors thank the other pediatric surgery team members of our hospital: Takahisa Tainaka, Wataru Sumida, Tomo Kakihara, Reiko Kato, Tomohiro Aoyama, and Kanako Omata. The authors also thank the allied health professional teams taking care of our patients at Saitama Children's Medical Center.
Disclosure Statement
No competing financial interests exist.