
Abstract
Abstract
Aim:
In children, the diameter at the hepaticojejunostomy anastomosis (HJA) can range from 10 mm to less than 5 mm, irrespective of the type of choledochal cyst (CC). We developed a maneuver that involves everting the mucosa (EM) of the Roux-en-Y loop jejunum and the common hepatic duct mucosa circumferentially, to facilitate suturing during laparoscopic HJA (lap-HJA). Otherwise, it is extremely difficult to distinguish between the lumen and the mucosa on the jejunal side.
Methods:
We used EM to treat 18 consecutive children with CC between 2016 and 2018. After transumbilical, extracorporeal Roux-en-Y loop-plasty, the closed end of the jejunum was incised with a scalpel and bleeding points were coagulated with bipolar diathermy. During lap-HJA, the mucosa at the incision was everted circumferentially by using 7/0 absorbable sutures and anastomosed securely to the common hepatic duct by using 5/0 or 6/0 absorbable sutures.
Results:
Mean age at surgery was 4.0 years old. HJA diameters were <5 mm (n = 4), 5–9 mm (n = 11), and >9 mm (n = 3). In all cases, EM allowed the lumen at the incision in the Roux-en-Y loop jejunum to be distinguished readily, and suturing proceeded smoothly. After follow-up of a mean of 1.5 years (range 0.5–3.0), no anastomotic leakages or stenoses have been reported.
Conclusions:
EM greatly facilitated secure anastomosis during lap-HJA, even when the diameter at the anastomosis was <5 mm. The safety and efficiency of lap-HJA in children with CC could be improved by this simple maneuver.
Introduction
Minimally invasive surgery (MIS) and open surgery for choledochal cyst (CC) in children share the same purpose; that is, complete excision of the CC, and secure/safe reconstruction to allow bile to be excreted freely; but MIS has additional advantages such as superior cosmesis, less postoperative pain, and rapid postoperative recovery. Although the laparoscopic approach to treating CC has become increasing popular in the past two decades, advanced technical skills are required compared with conventional laparotomy,1–3 especially for the hepaticojejunostomy anastomosis (HJA). As the diameter of the common hepatic duct in children can be very small, laparoscopic HJA (lap-HJA) is technically challenging, and the likelihood of anastomosis stricture is high.4,5
Consequently, every effort must be exerted to prevent anastomosis-related sequelae. One of the co-authors (A.Y.) considered whether everting the mucosa (EM) of the Roux-en-Y loop jejunum circumferentially during HJA might facilitate suturing and prevent complications. We present our EM maneuver for critical appraisal.
Materials and Surgical Technique
Since 2016, we have treated 18 consecutive children with CC by using laparoscopic repair for CC. All surgery was performed directly by 1 of 2 board-certified pediatric surgeons (H.K. or A.Y.), both with full accreditation for endoscopic surgery by the Japan Society for Endoscopic Surgery, or under their direct supervision, according to a technique previously described elsewhere.6,7 Briefly, the CC is dissected carefully free close to the common channel and opened. A fine ureteroscope equipped with a light source at its tip is inserted into the opened CC. Its tip is then inserted into the common channel to wash away any protein plugs under direct ureteroscopic view. The laparoscopic surgeon then measures the distance from the point where dissection is ceased at the CC end, to the common channel and the CC s dissected further distally for this distance. Measurement and dissection are repeated until the measured length is less than 5 mm when the CC is excised and ligated with an Endoloop (Ethicon, OH). After excision of the intra pancreatic CC, a Roux-en-Y jejunojejunostomy is constructed extracorporeally by extending the umbilical port incision.
Eversion of the mucosa during laparoscopic hepaticojejunostomy
The closed end of the jejunum is incised with a scalpel (Fig. 1A), and bleeding points are coagulated with bipolar diathermy (Fig. 1B). The mucosa at the incision is everted circumferentially by using 7/0 absorbable sutures (Fig. 1C), which enables the mucosa of the jejunum (Fig. 1D) to be identified readily and allows secure anastomosis to the common hepatic duct by using 5/0 or 6/0 absorbable sutures during lap-HJA (Fig. 2).

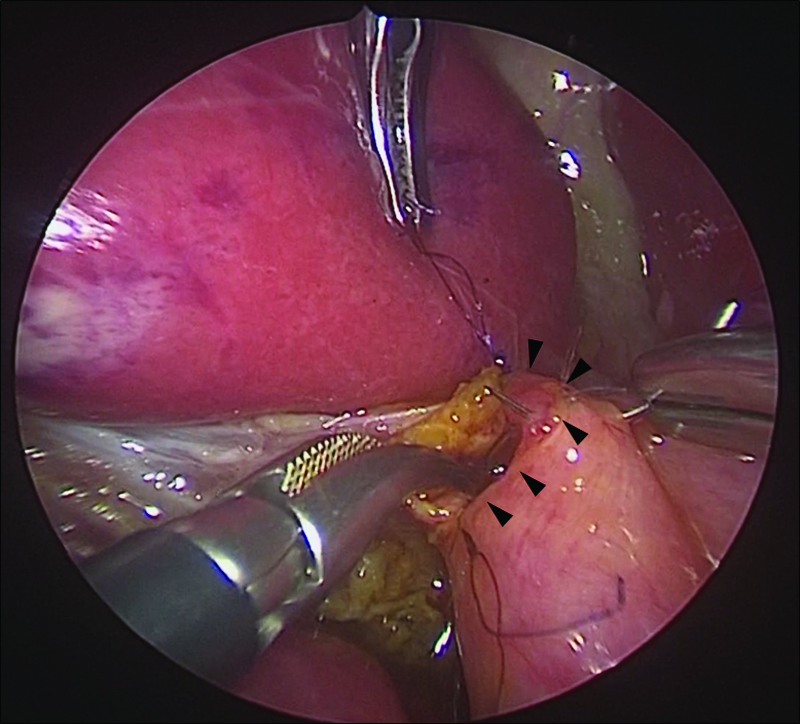
The everted mucosa of the jejunum (arrowheads) is readily identifiable and can be anastomosed securely to the common hepatic duct by using 5/0 or 6/0 absorbable sutures during laparoscopic hepaticojejunostomy anastomosis.
This study was approved by the Juntendo University School of Medicine Institutional Review Board and complies with the Helsinki Declaration of 1975 (revised 1983).
Results
This series comprised 15 girls and 3 boys. CC was fusiform (n = 15) or cystic (n = 3). Mean age and weight at laparoscopic repair for CC were 3.8 years (range 0.3–13.8) and 16.5 kg (range 5.6–59.0), respectively. The diameter of the anastomosis during lap-HJA was less than 5 mm in 4 cases, 5 to 9 mm in 11 cases, and more than 9 mm in 3 cases. Mean duration of surgery was 9.8 hours. Estimated mean intraoperative blood loss was minimal at 1.0 mL/kg. There were no conversions to open surgery and no intraoperative complications. Postoperative recovery was uneventful, and hospital discharge was possible after a mean of 8.5 days. All cases were well after a mean follow-up of 18 months (range 6–36 months). There have been no reports of anastomotic leaks or anastomotic stenoses. Even during lap-HJA when the diameter at the anastomosis was less than 5 mm, the lumen at the incision in the Roux-en-Y loop jejunum was easily visible, the mucosa of the incision in the jejunum was readily identifiable because of EM, and the mucosa could be sutured with less effort than when EM was not used.
Discussion
Since Farello et al. first reported laparoscopic-assisted CC dissection and hepaticojejunostomy in 1995, 8 an increasing number of centers have adopted their procedure for the safe, efficacious, and minimally invasive treatment of CC. However, lap-HJA using conventional techniques can be tedious because of poor visualization of the posterior wall, and it is generally considered the most difficult part of laparoscopic treatment of CC. Experience is necessary for confidence, but CC in children is rare; thus, the learning curve for lap-HJA in children is steep. In other words, it is very difficult for pediatric surgeons to gain enough experience to become competent to perform lap-HJA.
Our lap-HJA is performed by using the right upper quadrant port for the needle holder in the right hand, and the 3.9 mm subcostal port as the needle receiver in the left hand. By using extra trocars to prevent the quality of the anastomosis from deteriorating, our lap-HJA is virtually an open repair performed laparoscopically, because we are able to achieve the same angles used for suturing during an open HJA, which contributes to a sense of familiarity that can improve a less experienced surgeon's confidence.
We firmly believe that a precise layer-to-layer anastomosis with interrupted sutures is essential for a secure HJA. Thus, by EM we exploit the theoretical advantage of improving the seal between the approximated and sutured jejunal Roux-en-Y loop and common hepatic duct because everted mucosa is bulkier and has better vascularity than cut edges. Preserving the blood supply of the lumen of an anastomosis is of paramount importance for preventing complications, such as stricture and leakage. Experimental data would also suggest that anastomoses with everted mucosae heal with less fibrosis compared with anastomoses without everted mucosae. 9 EM also decreases the size of the lumen (again, because the mucosa is bulkier) and, in turn, decreases any untoward discrepancy in lumen diameter. In the current series, 4 cases had HJA diameters less than 5 mm, and these cases were also anastomosed smoothly because of EM.
Although we were able to perform our EM safely and successfully in all cases, operative times in our series were considerably longer compared with conventional open surgery. Our procedure took longer because of extra time required for thorough removal of protein plugs in the common channel (if present), and repeated measurement of the length of the distal CC and dissection until the measured length was less than 5 mm. We are particularly meticulous about both these processes because they are essential, but they did contribute to extending operative times. With experience, operative times will, no doubt, improve because there is a learning curve associated with any procedure, but one should not compromise thoroughness and successful outcome, for the sake of time.
Nevertheless, despite reasonable experience of treating CC laparoscopically, we still encounter difficulties during laparoscopic total excision, especially when the HJA diameter is less than 5 mm. Suturing skills are of the utmost importance for successful cure, and a number of different technical modifications to address HJA involving small diameters have been described: biliary ductoplasty with hepaticojejunostomy,10,11 a modified Kasai portoenterostomy procedure, 12 and partial hepatectomy with wide HJ. 13 There are reports describing a longitudinal incision made from the hepatic hilum to where the dilated hepatic ducts are, laparoscopically, to create a very wide anastomosis. Results of hilar ductoplasty with HJ have been reported to be satisfactory after a minimum of 2 years' follow-up, with a reduction in anastomotic strictures observed compared with conventional HJ. 14 However, the extended longitudinal incision along both narrow hepatic ducts that is required is itself technically difficult to perform.
Although we focused on lap-HJA in this series, our maneuver would also be valuable during open HJA as well, because it enhances visualization and gives the operating surgeon an opportunity to improve and secure the anastomosis during HJA by eversion of the jejunal mucosa of the Roux-en-Y loop, or enlarge the anastomotic opening as required to take into account potential contraction due to scarring of the circumferential eversion. However, the number of cases in this series is too small and the follow-up period is too short to make any definitive conclusions about the ultimate effectiveness of our maneuver, but complications caused by anastomotic inflammation and fibrosis would appear to be reduced. To the best of our knowledge, this is the first report about facilitating suturing during HJA by EM to reduce postoperative complications. Being simple and easy to perform are extra advantages.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.