
Abstract
Abstract
Background:
Increased intra-abdominal pressure resulting from pneumoperitoneum can cause renal physiological changes, such as oliguria and anuria, in mammals. Although videolaparoscopic operations are common, the occurrence of renal lesions due to these procedures has not been precisely documented in the literature. The aim of this study was to evaluate the impact of pneumoperitoneum on renal blood flow using renal scintigraphy in a rabbit model.
Methods:
Six New Zealand male rabbits weighing 3 kg, previously anesthetized, were mechanically ventilated and underwent pneumoperitoneum. Each animal served as its own control and was analyzed in two different moments: [99mTc] diethylenetriaminepentaacetic acid (DTPA) renal blood flow evaluation in baseline conditions (T0) and 30 minutes after installation of 15 mmHg-pneumoperitoneum (T1). The animals were monitored throughout the study by capnography, oximetry, and arterial pressure median, and were euthanized at the end of the experiment.
Results:
The quantitative analysis of the scintigraphic images of renal uptake of the radiopharmaceutical evidence reduced renal arterial blood flow during pneumoperitoneum. Compared with baseline conditions, all animals presented a reduction of renal blood flow varying from 16% to 82%, with mean [±standard deviation] of 53% [±24%].
Conclusions:
Pneumoperitoneum induces a significant reduction of the renal blood flow, as determined in this experimental method in rabbits and dynamic renal scintigraphy with [99mTc] DTPA is an adequate method to investigate this event in the experimental setting.
Introduction
The use of pneumoperitoneum to create a working space inside an anatomical cavity, permitting the introduction of optics and surgical instruments, created a new paradigm in the surgical treatment of several pathological conditions, by yielding better visualization, more precise interventions, and an easier postoperative period1,2 Video-assisted operations have rapidly evolved to become the gold standard worldwide, being performed both in adult and pediatric patients. Despite the advances brought by this method, the insufflation of gas increases intra-abdominal pressure (IAP) and produces significant physiological alterations.3,4
Changes in renal function have been described, leading to oliguria and anuria, especially in children.2,5 Oliguria is frequently observed during pneumoperitoneum, suggesting alterations in the renal physiology of etiology not yet elucidated.6–8
When IAP increases from 0 to 20 mmHg, vascular resistance increases by 555% and glomerular filtration rate decreases by 25%. 9 A prospective study showed decreased urinary output after a short period of pneumoperitoneum in 30 children undergoing laparoscopic operations. 5 The mechanisms by which pneumoperitoneum causes oliguria, although not fully understood, may be related to several factors, such as the reduction of cardiac output and, consequently, renal blood flow, secretion of systemic hormones, increased resistance peripheral vascular, and even renal and/or direct ureteral compression.6,10,11 The IAP levels, the duration of the procedure, the positioning of the patient, and the previous physiological status of the patients appear to be important contributors for the occurrence of these changes.8,12–15
The installation of a pneumoperitoneum acts like a model of ischemia-reperfusion, reducing blood flow during insufflation (ischemia), which is normalized after the abdominal cavity has been deflated (reperfusion), provoking oxidative stress that, in turn, acts at a cellular level, causing tissue damage and potentially organ dysfunction.16–18 In contrast, an experimental study in rats investigating the occurrence of acute renal injury secondary to surgical pneumoperitoneum through the expression of neutrophil gelatinase-associated lipocalin (N-GAL) did not demonstrate this association in animals with normal renal function in preoperative period. 19 In another study of women undergoing videolaparoscopic gynecological procedures, no significant elevations of N-GAL levels were observed, suggesting that oliguria may be transient and not related to early renal damage. 20
Although previous studies have shown reduced renal blood flow and decreased glomerular filtration rate associated with pneumoperitoneum, most of them used highly invasive methodology.8,21 In this study, we investigate the role of technetium 99m-diethylenetriaminepentaacetic acid (Tc 99m-DTPA) renal scan with dynamic images, to study the behavior of renal blood flow during surgical-induced pneumoperitoneum.
Materials and Methods
Experimental animals
Six male New Zealand rabbits weighing ∼3 kg, healthy and cleared by the veterinarian, were kept under controlled conditions: 20°C–24°C, relative humidity of 50%–60%, light/dark cycles of 12 hours: 8/20 hours, standard diet for rabbits, filtered and chlorinated water.
The animals underwent general anesthesia, with intramuscular ketamine (35 mg/kg) and xylazine (5 mg/kg), repeated throughout the procedure, as needed. Each animal also received a tracheostomy, catheterization of the right internal jugular vein, and an indwelling bladder catheter. An intra-abdominal 6F polyvinyl catheter was placed through a small incision in the upper abdominal midline wall, for pneumoperitoneum installation. Through the internal jugular vein catheter, 0.9% saline was infused at a rate of 0.35 mL/(kg·min).
Every animal was kept on spontaneous ventilation during the initial baseline phase, and switched to assisted-mechanical ventilation during and after pneumoperitoneum using a VLP-4000P mechanical pulmonary ventilator (Vent-Logos).
Experimental protocol and acquisition of images
T0: Immediately after stabilization from anesthetic induction the rabbits received 74 MBq of [99mTc] DTPA, and were evaluated under a Siemens Symbia 2T SPECT/CT scintigraphy equipment, with dynamic acquisitions of flow, capturing 1 image each 2 seconds for 2 minutes.
Installation of pneumoperitoneum: After the initial evaluation of renal blood flow, a 15 mmHg pneumoperitoneum was created and maintained for 30 minutes, by a 1 L/min insufflation of carbon dioxide (CO2) through a SmithNephew® model 15, Dyopneumatic insufflator.
T1: Thirty minutes after the installation of pneumoperitoneum, mathematical removal of the residual [99mTc] DTPA from T0 was performed and administration of 74 MBq of [99mTc] DTPA was repeated. Scintigraphy was performed in the same way as described for T0. The standard processing protocol for [99mTc] DTPA was used.
Analysis of the data was made through quantitative and qualitative analysis of the flow images. Renal arterial blood flow was determined by calculating the ratio of [99mTc] DTPA concentration in the renal areas to the concentration in the aorta on the image generated 2 seconds after the first contrast appearance in the aorta, as expressed in Figure 1 and Table 1.
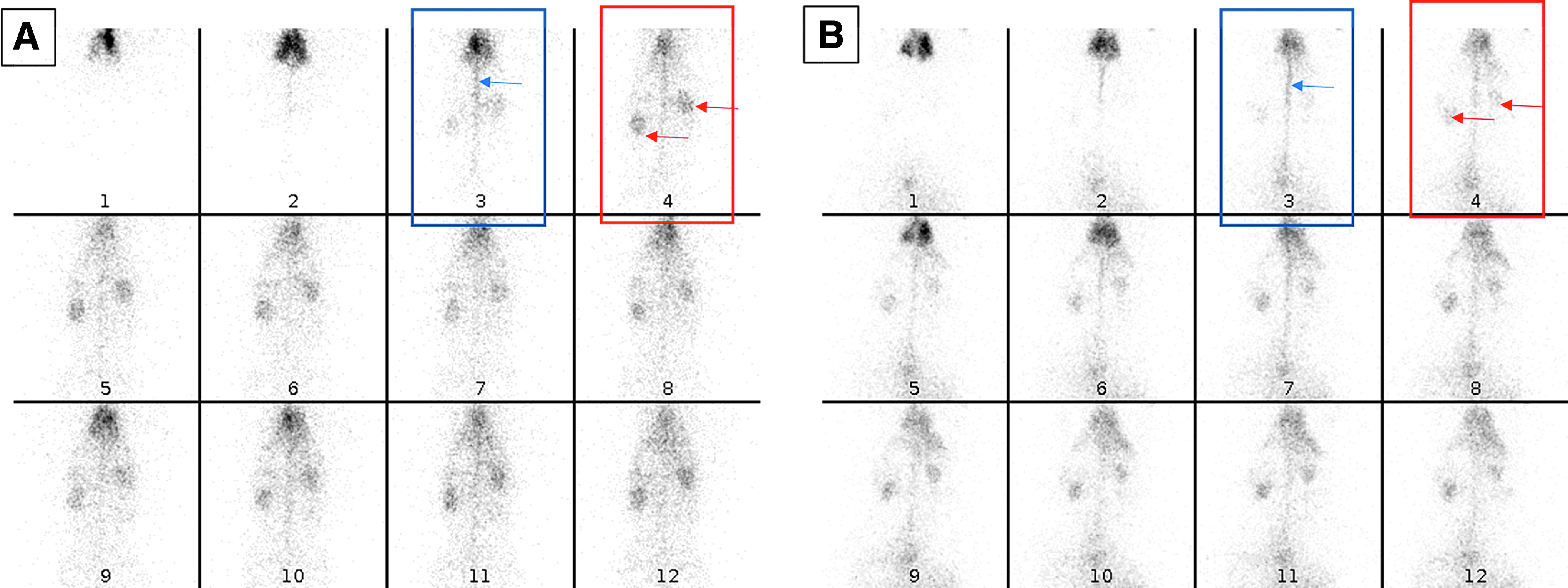
Scintigraphy images each 2 seconds after 74 MBq [99mTc] diethylenetriaminepentaacetic acid intravenous bollus, in baseline conditions
[99mTc] Diethylenetriaminepentaacetic Acid Concentration Ratio Values in the Renal Areas in Relation to the Aorta
PP, pneumoperitoneum; SD, standard deviation.
At the end of the procedure, euthanasia was performed with intravenous sodium thiopental (90 mg/kg) followed by infusion of 19.1% KCl (5 mL) and observation for 20 minutes.
The ethical principles for the use of laboratory animals, elaborated by SBCAL—Brazilian Society of Laboratory Animals—were fully applied during the validity of this protocol; as was the strict compliance with the current national legislation—Law No. 11,794, of October 8, 2008. The project was approved by the Ethics Committee on the Use of Animals of CEUA/UNICAMP on November 4, 2016 (protocol no. 43841).
Statistical analysis was made using the Wilcoxon signed rank test. P values <0.05 were considered statistically significant.
Results
The results obtained through the analysis of scintigraphic images of renal uptake and renal clearance of the radiopharmaceutical at the aforementioned time points are depicted in Table 1 and Figures 1 and 2 and show that, compared with baseline conditions, all animals developed reduction of renal blood flow during pneumoperitoneum, ranging from 16% to 82% with a mean ± standard deviation of 53% ± 24%. Figure 3 presents the results of left, right, and both kidneys, in baseline conditions and during pneumoperitoneum.
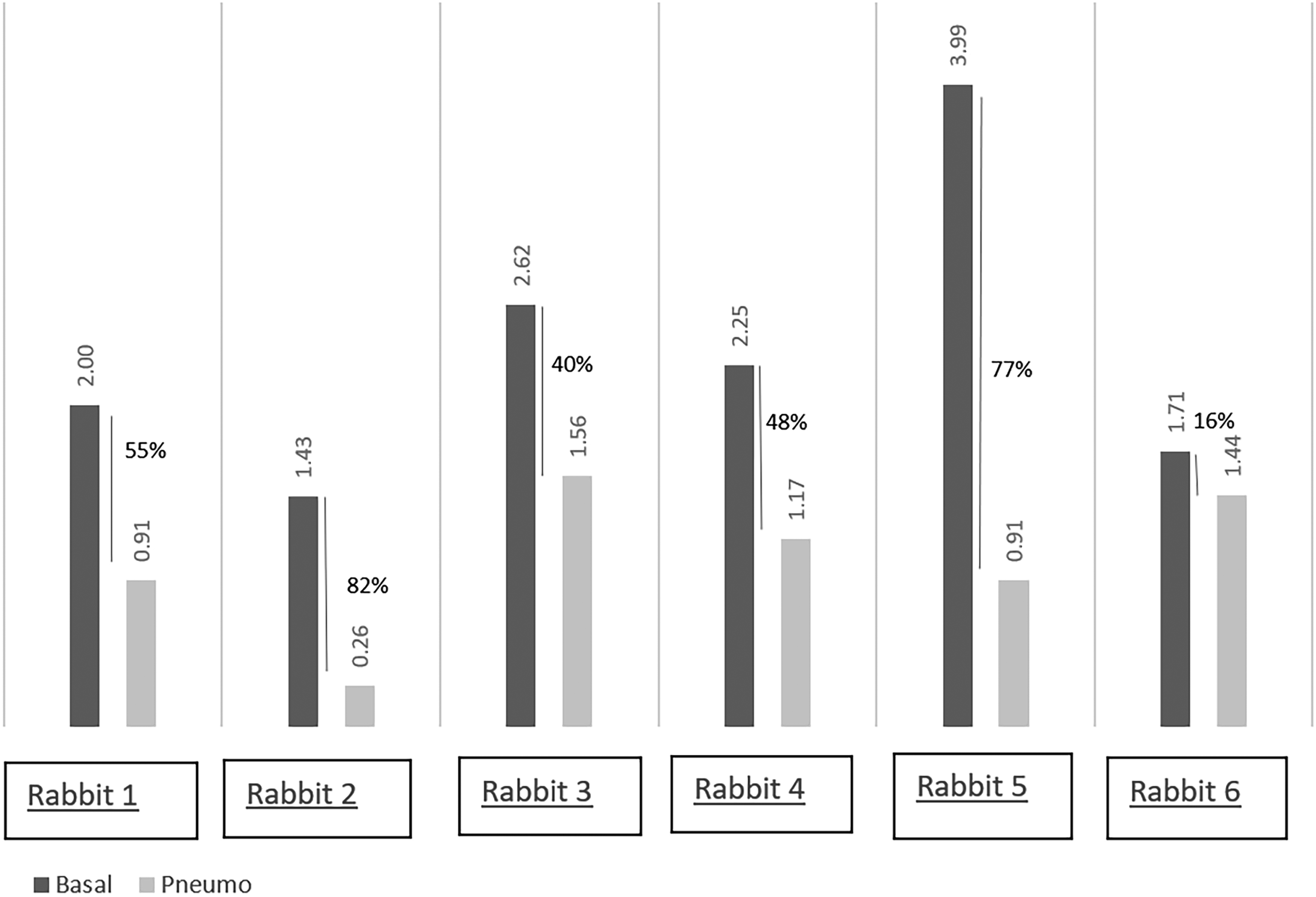
Baseline and post-pneumoperitoneum total (right + left) renal artery blood flow (reduction in %). Percentage of reduction of renal arterial blood flow verified in T1 (after 30 minutes of pneumoperitoneum, with intra-abdominal pressure = 15 mmHg), in relation to T0 (control in the physiological conditions).
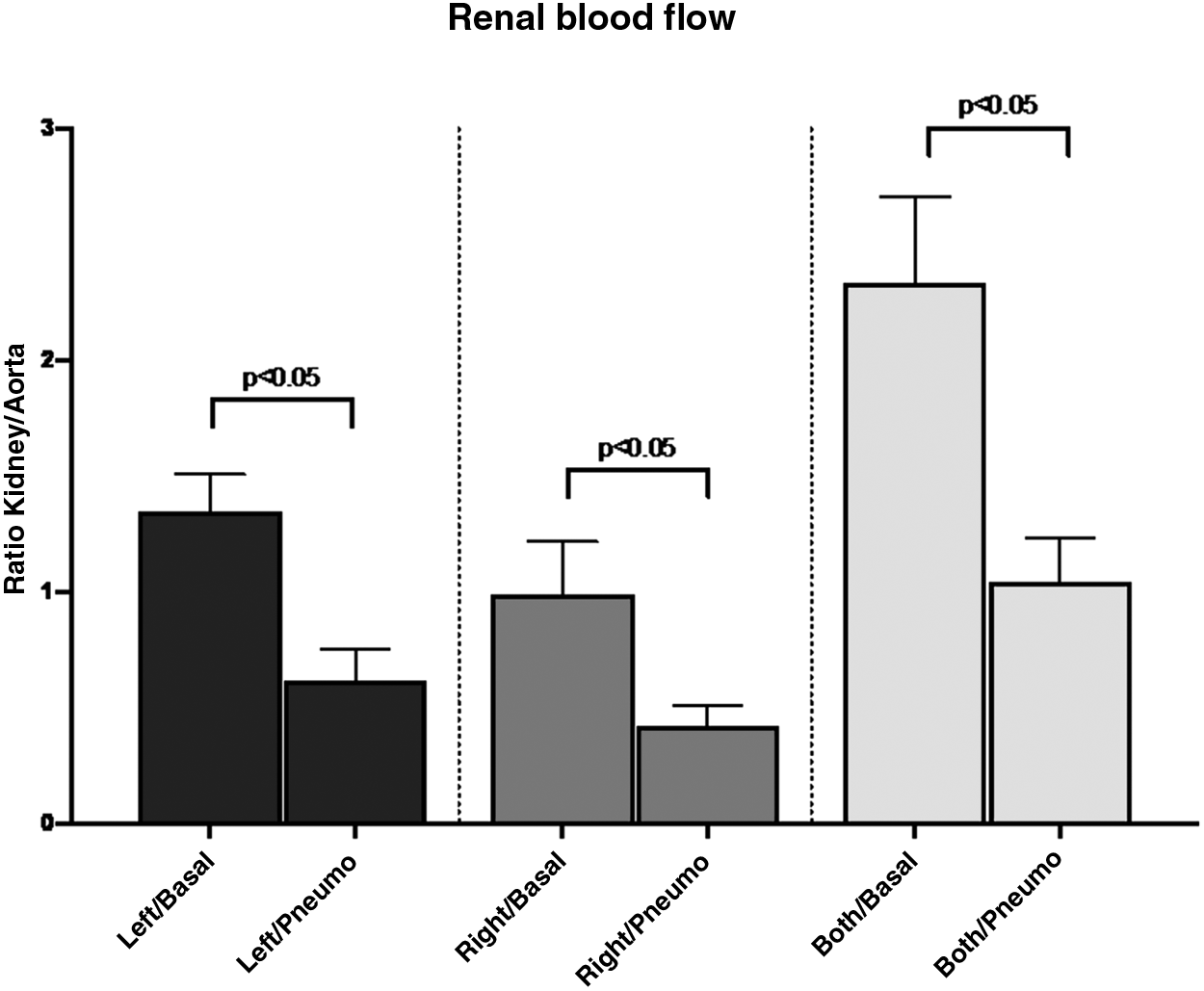
Graphic representation (mean + standard error of the mean) of baseline and pneumoperitoneum blood flow of left kidney, right kidney, and both kidneys.
Discussion
The results of this scintigraphic study, using a dynamic, functional, and less invasive method, indicate reduction of renal blood flow during pneumoperitoneum. The results are in agreement with previous findings by other authors.
Since 1982, there has been an increasing interest in the evaluation of the impact of pneumoperitoneum on renal function. Harman et al. 9 investigated the effects of increased IAP on renal function in dogs by catheterization of both the renal artery and vein and the installation of an inflatable bag inside the peritoneal cavity. Upon reaching a pressure of 20 mmHg, there was a 25% decrease in the glomerular filtration rate. Most studies on the physiological effects of elevation of IAP also use invasive methods and report similar results.8,10,12,22–25 However, none of these studies demonstrate permanent lesions or histological changes.
In a study by Lindström et al., 22 the effects of increased IAP on renal function in rats were also examined by analysis of the renin–angiotensin–aldosterone system, demonstrating a 70% drop in glomerular filtration rate with an IAP of 10 mmHg.
It is uncertain if and when elevation of IAP by pneumoperitoneum during videolaparoscopic surgical procedures may cause permanent renal injury.
A systematic review, including 55 studies on the effect of pneumoperitoneum on renal function, showed high heterogeneity between methodologies and indeterminate risk of bias in most studies. Meta-analysis was able to highlight elevated serum creatinine during pneumoperitoneum, and decreased urine output and renal blood flow, although such reduction was not evident in subgroups with up to 30 minutes of pneumoperitoneum. 21 These results suggest that renal damage is dependent not only on the pneumoperitoneum itself, but also on the preoperative clinical conditions of the patients. Accordingly, in patients with preoperative impaired renal function, these changes may become more evident, since a decrease in diuresis during the pneumoperitoneum is frequently observed. 4
Most of these studies aim to establish the safety levels pneumoperitoneum for laparoscopy, since the use of this access for urological operations pathologies or complex surgeries has become more common, and longer surgical times are often observed.2,26 Knowing the real influences of pneumoperitoneum by CO2, especially its effects on the kidneys, allows the surgeon to minimize the risks and maximize the advantages of this access route, especially in children.
From the methodological point of view, it is recognized that duration and level of IAP during pneumoperitoneum are technical points that may largely influence the degree of renal impairment.
Demyttenaere et al. 8 reviewed 17 animal studies of renal blood flow where different levels of IAP, varying from 4 to 40 mmHg, were used and concluded that 15 mmHg or greater already showed significant reductions in renal blood flow. Wever et al. 21 came to similar conclusions after systematically reviewing an additional 55 animal studies.
As for the duration of the peritoneum, these same authors were able to demonstrate increasing levels of decreased renal flow with times exceeding 30 minutes. Based on these findings we chose to work with an IAP of 15 mmHg and duration of 30 minutes. As shown by Demyttenaere et al., 8 pressures of 15 mmHg have been used systematically to mimic clinical situations and are sufficient to cause significant changes in renal blood flow in many studies. The duration of only 30 minutes was selected given its sensitivity and also to minimize the risk of hemodynamic instability of the animal, when longer durations of pneumoperitoneum were used.
This experimental study utilized a less invasive and original methodology using nuclear medicine with dynamic renal scintigraphy with [99mTc] DTPA for the purpose of studying the effects of pneumoperitoneum on renal blood flow. The scintigraphic images in baseline conditions, under adequate conditions of temperature, pressure, and pulmonary ventilation, demonstrated that renal filtration of the radiopharmaceutical was preserved. After the pneumoperitoneum was created, respecting the same controlled conditions, there was a decrease in the uptake of [99mTc] DTPA, suggesting that the increase of the IAP leads to a reduction of renal arterial blood flow.
Additional studies, measuring glomerular filtration through quantitative analysis of the uptake and clearance of [99mTc] DTPA, are necessary to clarify the effect of IAP on renal physiology. Also, more specific variables should be looked at, to determine which metabolic pathways of the urinary tract may be directly affected.
Under the experimental conditions of this study, it is possible to conclude that pneumoperitoneum induces a significant reduction of the renal blood flow, and that dynamic renal scintigraphy with [99mTc] DTPA is an adequate method to investigate this event in the experimental setting. These results corroborate the findings obtained by other researchers using more invasive methods and authorize the use of this less invasive and sensible method to investigate the pathophysiology of pneumoperitoneum in the experimental settings.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study received partial financial support from the FAEPEX—UNICAMP.