
Abstract
Abstract
Introduction:
The majority of esophageal atresia (EA) patients undergo surgical repair soon after birth. However, factors due to patient characteristics, esophageal length, or surgical complications can limit the ability to obtain esophageal continuity. A number of techniques have been described to treat these patients with “long-gap” EA. Magnets are a nonsurgical alternative for esophageal anastomosis. The purpose of this study was to report long-term outcomes for the use of magnets in EA.
Materials and Methods:
Between July 2001 and December 2017, 13 patients underwent placement of a magnetic catheter-based system under fluoroscopic guidance at six institutions. Daily chest radiographs were obtained until there was union of the magnets. Magnets were then removed and replaced with an oro- or nasogastric tube. Complications and outcomes were recorded. The average length of follow-up was 9.3 years (range 1.42–17.75).
Results:
A total of 85% of the patients had type A, pure EA, and 15% had type C with previous fistula ligation. The average length of time to achieve anastomosis was 6.3 days (range 3–13). No anastomotic leaks occurred, and all of the patients had an expected esophageal stenosis that required dilation given the 10F coupling surface of the magnets (average 9.8, range 3–22). Six patients (46%) had retrievable esophageal stents, and two underwent surgery; yet all maintained their native esophagus without interposition. A total of 92% were on full oral feeds at the time of follow-up.
Conclusion:
The use of magnets for treatment of long-gap EA is safe and feasible and accomplished good long-term outcomes. The main complication was esophageal stricture, although all patients maintained their native esophagus. A prospective observational study is currently enrolling patients to evaluate the safety and benefit of a catheter-based magnetic device for EA.
Introduction
Esophageal atresia (EA), with or without a tracheoesophageal fistula, is the most common congenital anomaly of the esophagus. 1 The majority of patients with EA undergo surgical repair with ligation of the fistula if present and esophageal anastomosis soon after birth. However, factors due to the patient's characteristics, anatomic concerns, or surgical issues can limit the ability to obtain esophageal continuity. 2 These limitations include prematurity, congenital anomalies, a long gap between the ends of the esophagus, failed attempt of primary anastomosis initially, and postoperative complications.
Several techniques have been described to treat these patients with EA not amenable to initial repair consisting of delayed primary anastomosis, 3 extensive mobilization, myotomies, 4 esophageal flaps, and traction of the segments.5,6 The use of thoracoscopy has more recently been utilized by some surgeons to improve visualization and achieve significant mobilization. 7 van der Zee et al. has reported employing thoracoscopic elongation procedures in the neonatal period.8,9 Similarly, Bogusz et al. reported a series with a staged thoracoscopic approach using internal traction. 10 Although esophageal replacement is an option for establishing esophageal continuity in difficult EA cases, conservation of the native esophagus is functionally optimal. 11 However, no definitive consensus for the surgical approach in this technically challenging category of patients exists. 12
The use of magnets is a nonsurgical alternative for esophageal anastomosis. 13 The magnetic force promotes lengthening and approximation of the proximal and distal esophageal ends with compression and ischemia of the interposing tissue. The magnets can be placed primarily or as a second stage after a lengthening procedure. 14 These treatment options have shown promising results.15,16 The purpose of this study was to report the long-term outcomes for the use of magnets in the treatment of long-gap EA.
Materials and Methods
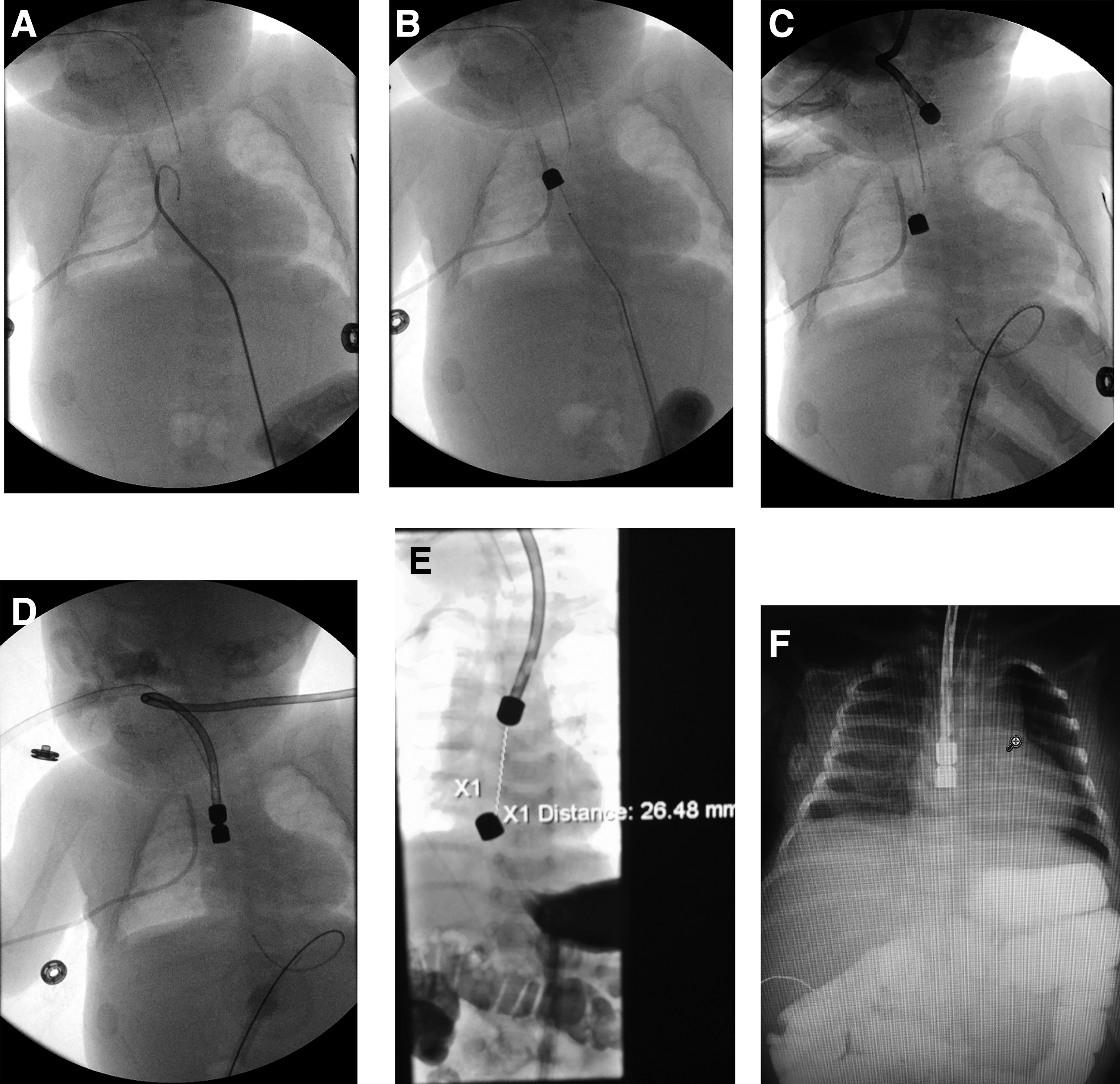
Between June 2001 and December 2017, 13 patients with EA underwent placement of a magnetic anastomosis catheter-based system under fluoroscopic guidance at six institutions. The distances between the esophageal ends were measured before placement with metal probes without exerting pressure on the pouches, and all were <4 cm immediately preceding implementation. All of the patients had a prior gastrostomy, and the lower device was inserted through the mature gastrostomy site. After placement of the device, daily chest radiographs were obtained until union of the magnets occurred. Successful anastomosis was identified by saliva in the gastrostomy catheter or feeds in the esophageal catheter. A few days after confirmation, the magnets were removed and replaced with an oro- or nasogastric tube over a wire. Complications and outcomes were recorded.
The devices used were Food and Drug Administration (FDA)-approved Humanitarian Device Exemption (HDE) with an esophageal catheter and gastric catheter both containing an inner magnet (Cook Medical, Bloomington, IN). The proximal catheter has a suction port to remove saliva and the distal portion has a channel for feeds (Fig. 1A, B). The magnets taper to a 10F coupling surface to allow gradient compression anastomosis. Placement was performed with general anesthesia. The gastrostomy button was removed and dilated to an 18F diameter. A wire was then inserted to the end of the lower esophageal pouch and the gastric catheter placed over the wire. Once in good position, the balloon was inflated. The same procedure was done with the oral catheter through the mouth or nares (Fig. 2).

Results
A total of 85% of the patients had a type A (i.e., isolated EA) and 15% of the patients had a type C EA with previous ligation of the fistula (Table 1). One of the type C patients underwent only fistula ligation initially without esophageal anastomosis due to a cardiac anomaly and poor respiratory status. The other type C patient had initial fistula ligation and repair but had a postoperative stricture that was unable to be dilated and thus magnet compression was used for reanastomosis. The postnatal ages of the patients when the devices were placed averaged 4.5 months (range 2–7.5 months). The average length of time to achieve anastomosis with the magnets was 6.3 days (range 3–13). No anastomotic leaks in any of the patients occurred, and all had an expected stenosis requiring dilation (average number of dilations 9.8, range 3–22). To correct a refractory stricture, 6 patients (46%) had esophageal stents placed, and 2 patients underwent surgery. One patient had a perforation after dilation and thus underwent segmental resection and reanastomosis. The other patient had a recalcitrant stricture requiring resection and reanastomosis. No patient had an intestinal or gastric interposition. A total of 92% of the patients were on full oral feeds at the time of follow-up. One patient could not achieve full oral feeds due to significant life-threatening tracheomalacia requiring tracheostomy. The average length of follow-up was 9.3 years (range 1.42–17.75).
Table of Cases
Discussion
Long-gap EA, defined as cases in which a primary anastomosis of both ends of the esophagus cannot be performed without significant tension, is a technically challenging condition to treat. 12 It is commonly measured during fluoroscopy and there is no standard distance defining it. 17 When early repair is not possible, a variety of techniques have been employed to bridge the gap and establish esophageal continuity. Many of these methods require multiple operations and may expose the patient to repeated anesthetics, prolonged operative time, and physiological stress.
The use of magnets for various types of anastomoses has been described in the literature since the 1970s.18–20 In patients with EA, magnetic anastomosis was first reported in five infants in Argentina. 16 Anastomosis was achieved in all of the patients in an average of 4.8 days. A later series was published describing achievement of primary esophageal anastomosis in an additional four patients with EA using catheter-based bullet-shaped magnet pairs. 15 A recent study described a two-staged approach whereby young infants have an initial esophageal approximation without luminal continuity followed by magnamosis. 14 This study reports long-term outcomes for some of the previously reported patients as well as additional ones at different institutions demonstrating continued patency of anastomosis, esophageal preservation and functional integrity, and further safety and efficacy.
The magnets situated in the proximal and distal esophageal pouches are able to attract one another due to their opposite polarity. Once the magnets have connected, the tissue between them becomes ischemic and sloughs while the outer rim heals establishing the anastomosis. Patients with esophageal gaps of >4 cm are not candidates for placement of a catheter-based magnet device due to the fact that this length surpasses the strength of the magnetic field and will fail to achieve attraction and connection.
Although this method of using the catheter-based magnets had a high rate of stenosis, all of the patients in this series had a successful anastomosis with no leaks or need for interposition grafts. The magnetic coupling surface between the ends of the magnets is only 10F, so a natural waist results after connection. As such, it is anticipated that several dilations may be needed to expand the anastomosis to recreate the diameter of the remaining esophagus. Further improvements of the magnet shape or diameter may be implemented in the future to minimize the risk of stenosis. In addition, being able to control the magnetic strength as the pouches approach one another might allow greater flexibility of the lengthening portion. Finally, early stent placement may be an alternative to prevent a stricture.
The use of magnets in patients with EA may be particularly beneficial for patients with cardiac or other congenital anomalies and those who have undergone previous operations or complications in which reoperative surgery is not optimal. In these select patients, the use of the magnets may avoid operation and potentially an anesthetic as well. Fluoroscopy during the procedure and daily radiographs are utilized to aid with visualization and assessment of the lengthening process. In addition, the magnets may also be used in combination with surgery such as for postoperative esophageal strictures not amenable to dilation 21 or in a staged manner for esophageal gaps >4 cm after initial operative stretching procedures. 22
There are several limitations of the study, including its retrospective nature. There is also the possibility that there were additional adverse events that were not captured. However, this seems unlikely given the fact that all of the patients were followed up frequently initially and then on an approximately annual basis. Finally, there was likely some selection bias in this study given that only certain patients were chosen for the procedure.
Conclusion
The use of magnets for treatment of long-gap EA is safe and feasible and has accomplished good long-term outcomes in this retrospective study. The main complication was an expected esophageal stenosis requiring dilation in all, and if a refractory stricture developed, stent placement in 6 and surgery in 2 of the patients in this cohort. Nevertheless, there were no anastomotic leaks and all patients have their native esophagus without an interposition procedure. A prospective single-arm observational study is currently enrolling patients to evaluate the safety and benefit of the Flourish™ device, (Cook Medical, Winston-Salem, NC) a catheter-based magnetic device used to lengthen the atretic esophageal ends and create an anastomosis for EA patients.
Footnotes
Disclosure Statement
Dr. M. Zaritzky is a medical consultant for Cook Medical, United States, and shares the patent and future royalties of Flourish. No competing financial interests exist for the other coauthors.
Funding Information
No funding was received for this article.