
Abstract
Abstract
Introduction:
Solid pseudopapillary neoplasm (SPN) is the most commonly encountered pancreatic tumor in adolescents. Owing to its malignant potential, the current recommendation for management is complete surgical resection; however, there is no broad consensus on the operation of choice to accomplish this. Herein, we describe three consecutive laparoscopic spleen-preserving distal pancreatectomies for SPN in adolescents.
Materials and Methods:
Our cohort included all patients <18 years of age treated at our institution from 2015 to 2018 who underwent surgical resection of an SPN.
Results:
Three patients (age 13–16) were identified. Two of the patients were male. All patients underwent laparoscopic distal pancreatectomy with preservation of the main splenic artery and vein. No patients suffered from postoperative pancreatic fistula. Median length of stay was 5 days. Final histology revealed SPN in all 3 cases, with tumor size ranging from 2 to 10 cm in greatest dimension. All margins were negative for tumor. All 3 patients have been followed (mean: 6 months) with surveillance ultrasound demonstrating a normal remnant pancreas and normal splenic perfusion.
Conclusions:
Laparoscopic spleen-preserving distal pancreatectomy is a safe and effective treatment for SPNs of the body and tail of the pancreas in adolescents. This approach achieves the margin negative resection that is appropriate for the disease without subjecting children to the risk of postsplenectomy sepsis or the need for antibiotic prophylaxis, and may be associated with a reduction in perioperative morbidity. Therefore, laparoscopic distal pancreatectomy with splenic preservation is our preferred operation in adolescents presenting with SPN.
Introduction
Solid pseudopapillary neoplasm (SPN) is a rare pancreatic tumor with low-grade malignant potential, with just under 2800 cases reported in the combined adult and pediatric literature. 1 However, SPN remains the most common pancreatic tumor in children and adolescents, making up ∼70% of all pediatric pancreatic tumors.2–5 With increased utilization of abdominal imaging and standardization of pathological classifications, reporting of SPN has increased dramatically for the past two decades. 1 For these reasons, management of SPN is a diagnosis of increasing importance for pediatric surgeons.
Upfront surgical resection of SPN is associated with excellent outcomes and remains the standard of care for localized disease.1,6 However, there is no broad consensus on the optimal approach or extent of resection. For tumors in the body and tail of the pancreas, the conventional approach has been open distal pancreatectomy with splenectomy.7,8 More recently, minimally invasive and spleen-preserving operations have been demonstrated as feasible and advantageous for the treatment of pancreatic neoplasms in the adult literature.9–12 Similar reporting in pediatric patients is more limited.
Herein, we present our experience performing three consecutive laparoscopic spleen-preserving distal pancreatectomies for SPN in adolescents. As it applies to our cohort, we consider the feasibility, safety, and suitability of this approach as the operation of choice for SPN in pediatric patients.
Case Reports
Case 1
A 13-year-old boy presented to our pediatric emergency department with 1 day of acute onset left upper quadrant pain, nausea, and vomiting. Initial radiograph showed both gastric and esophageal air fluid levels consistent with a gastric outlet obstruction. A pancreas protocol computed tomography (CT) scan demonstrated a heterogenous mass involving the body and tail of the pancreas measuring 5.5 × 4.7 cm (Fig. 1). The mass had evidence of internal hemorrhage and appeared to be causing the gastric outlet obstruction. Based on the imaging characteristics, it was believed to be an SPN.
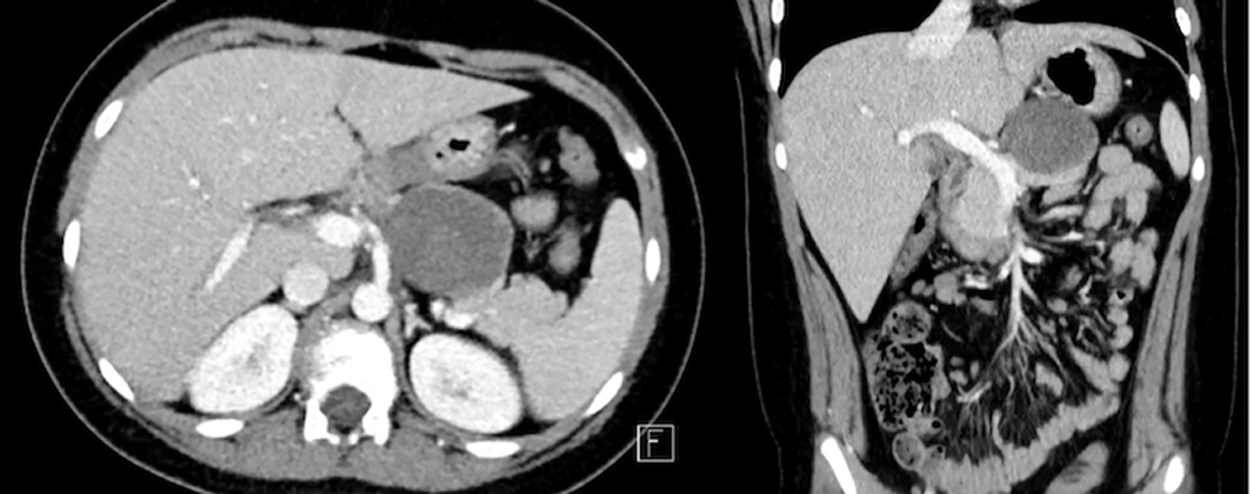
CT of a 5.5 cm solid pseudopapillary neoplasm causing gastric outlet obstruction.
Because of the acute onset of symptoms and gastric outlet obstruction, the decision was made to proceed with upfront operative exploration and resection. Intra-abdominal access was gained through the umbilicus using a Veress needle technique, and a 12 mm port was placed. After diagnostic laparoscopy confirmed the absence of disseminated disease, three additional working ports were placed under direct visualization in the bilateral upper quadrants and the left lower quadrant. Entry to the lesser sac was accomplished through division of the gastrocolic ligament and the short gastric arteries. Elevation of the stomach revealed the tumor arising from the body of the pancreas. The upper and lower edges of the pancreas were dissected free from the surrounding tissue and any sizable vessels feeding the splenic artery or vein were ligated using either clips or a LigaSure™ bipolar sealer/divider device (Valleylab, Boulder, CO). A tunnel between normal pancreas parenchyma and the splenic vessels was made just proximal to the mass, and the pancreas was divided using an endoscopic GIA stapler. Dissection proceeded distally, separating the remaining parenchyma and mass from the main splenic vessels until the specimen was entirely free and mobile. The specimen was placed in an endoscopic retrieval bag and removed through a slightly enlarged umbilical incision. Subsequent inspection confirmed a well-perfused spleen without injury. Cases 2 and 3 were performed in a similar manner, except where indicated (Table 1).
Patient and Operative Characteristics
Laparoscopic spleen-preserving distal pancreatectomy for solid pseudopapillary neoplasm in adolescents.
bx, biopsy; CT, computed tomography; EUS/FNA, endoscopic ultrasound/fine needle aspirate.
Pathology revealed a 4.0 cm well-circumscribed solid and cystic mass consistent with SPN, with 12 lymph nodes negative for tumor, and negative surgical margins. The child suffered from postoperative feeding intolerance, attributed to his degree of acute gastric outlet obstruction. This prolonged the length of stay to 10 days and required a brief period of parenteral nutrition. There was no pancreatic fistula or other perioperative complications. Follow-up after 2 years with duplex ultrasound showed no evidence of disease and a normal spleen.
Case 2
A 16-year-old girl presented to our pediatric emergency department with abdominal pain and was found to have elevated serum amylase and lipase. A CT scan was obtained, which demonstrated a small 1.0 × 0.8 cm focal hypodensity with nodular enhancement in the tail of the pancreas. After resolution of her abdominal pain, an magnetic resonance cholangiopancreatography (MRCP) further characterized the lesion as a likely SPN. However, with the recent episode of pancreatitis and some degree of uncertainty as to whether this was a neoplastic or inflammatory lesion, an endoscopic ultrasound/fine needle aspirate (EUS/FNA) was performed. Immunostaining of neoplastic cells was positive for β-catenin, confirming the diagnosis as SPN.
A laparoscopic spleen-preserving distal pancreatectomy was performed in the manner described earlier, with the addition of a percutaneous Blake drain left in the resection bed. Pathology revealed a 1.5 cm well-circumscribed mass consistent with SPN, with five lymph nodes negative for tumor, and negative surgical margins (Fig. 2).
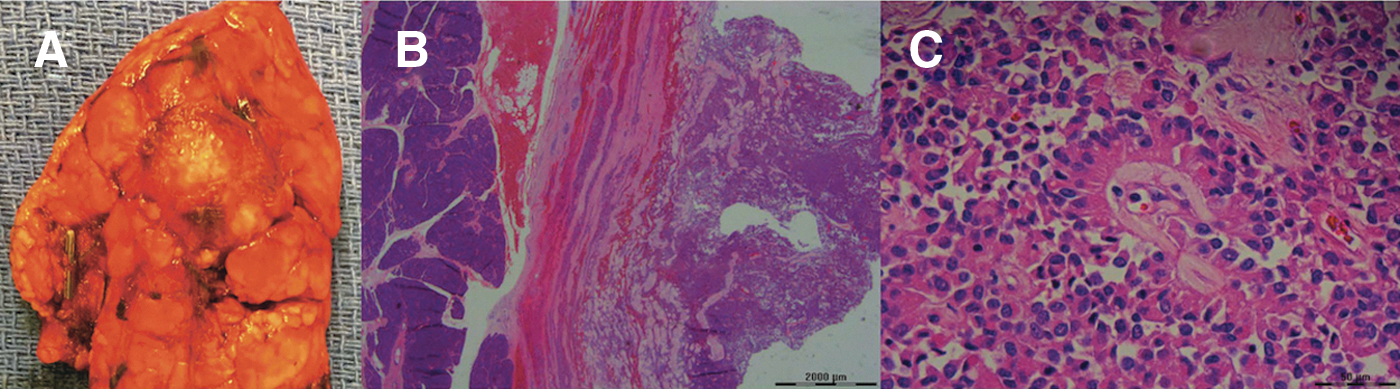
Pathological examination of a solid pseudopapillary neoplasm.
The postoperative course was unremarkable. Drain output was low volume and was removed before discharge on postoperative day 5. Follow-up after 3 months with duplex ultrasound showed a normal pancreas remnant and spleen.
Case 3
A 16-year-old boy was found to have a large pancreatic mass after CT scan was obtained in the workup for 2 days of epigastric pain. The mass measured 7.9 × 10.4 cm, was well circumscribed, and heterogenous (Fig. 3). A multidisciplinary tumor board was convened, and the decision was made to proceed with laparoscopic exploration and core needle biopsy to establish a diagnosis. Pathology of the biopsy specimen confirmed SPN, and the patient underwent elective laparoscopic spleen-preserving distal pancreatectomy.

CT of a 10.4 cm solid pseudopapillary neoplasm involving the splenic hilum. CT, computed tomography.
The operation proceeded as described earlier; however, on exploration the mass was involving the splenic hilum and obscuring visualization of the distal splenic artery and vein. Spleen preservation was accomplished through proximal identification and isolation of the vessels above and behind the body of the pancreas, respectively, and careful medial to lateral dissection. A Jackson–Pratt drain was left in the resection bed.
Pathology was consistent with the biopsy, confirming an SPN measuring 10 cm in greatest dimension. Four lymph nodes and all margins were uninvolved. The postoperative course was unremarkable, and the drain was removed before discharge on postoperative day 5. There is no evidence of disease and no change in the spleen at 6 months follow-up.
Discussion
To our knowledge, this is the first report of three consecutive laparoscopic spleen-preserving distal pancreatectomies for SPN in adolescents. Although rare, SPN remains the most common pancreatic neoplasm in children and adolescents, and reporting of this diagnosis is increasing.1–3 Therefore, determining the optimal operative approach is paramount to pediatric surgeons, and we hope that our experience will increase awareness of the feasibility and benefits of minimally invasive and spleen-preserving surgery for SPN in adolescents.
The first definitive report of SPN is credited to Virginia Kneeland Frantz in her 1959 atlas of pancreatic tumors. 13 Since that time, just >500 pediatric cases have been described.14–16 The diagnosis is usually made in the workup of nonspecific abdominal pain, and there is a strong female predominance. In our series, 1 patient presented with pancreatitis, which is infrequently described. In addition, 2 of the 3 patients presented here are male. Although limited to our single institution series, this suggests that presentation and epidemiology in pediatric patients might be unique. By reporting our series, we hope to increase consideration of SPN as a diagnosis in a wider range of young patients to decrease the high rate at which this tumor is misdiagnosed in children.17,18
As in our series, most SPNs are localized to the pancreas at the time of diagnosis.6,19–22 SPN portends an excellent prognosis, and with complete resection, >95% of patients are disease free with <2% mortality at 5 years. 1 In children, mortality from SPN is exceedingly rare. In two comprehensive long-term follow-up studies after surgically treated SPN, overall survival after median 8.4 and 15-year follow-up was 100%.15,23 When recurrence does occur in children, it is almost exclusively in those diagnosed at <13.5 years of age or those with a positive surgical margin. 23 Our study is limited by short median follow-up of 6 months. However, we expect excellent outcomes for the 3 patients presented here based on their risk factors and negative surgical margins in all cases. Because of the very good prognosis after surgery, upfront resection remains the treatment of choice for SPN.
There remains debate regarding the optimal extent and type of surgical approach for SPN. Just >50% of pediatric SPNs are found in the body and tail of the pancreas, making them amenable to distal pancreatectomy for complete resection.14,16 For body and tail lesions, several approaches have been utilized: traditional open and minimally invasive distal pancreatectomy, with and without splenectomy, and pancreas sparing enucleation.6,21,24–26 Because of its low malignant potential, we believe that SPN in the body and tail of the pancreas is ideally suited for a minimally invasive and spleen-sparing approach.
The laparoscopic approach to distal pancreatectomy has gained increased acceptance in adults and is associated with decreased morbidity. Specifically, when compared with the conventional open operation, laparoscopic distal pancreatectomy is associated with less blood loss, reduced length of hospital stay, decreased risk of postoperative wound infection, and no substantial increase in operative time.9,18 However, the reported experience with minimally invasive pancreatectomy for pediatric tumors is more limited. Only 33 laparoscopic distal pancreatectomies for SPN have been reported in children, and just 57% of those included splenic preservation.3,4,17,22,24,25,27–32 Spleen preservation was achieved in all patients in the present series, despite the presence of large tumors (range 1.5–10 cm) and hilar involvement.
Distal pancreatectomy with splenectomy is appropriate for high-grade malignancies such as adenocarcinoma and some neuroendocrine tumors, where omission of splenectomy might compromise radical oncological resection. In contrast, SPN represents a low-grade malignancy, where margin-negative resection and radical resection seem to have similar oncological outcomes in children.11,15,23 Spleen preservation eliminates the risk of overwhelming postsplenectomy infection and the need for antibiotic prophylaxis. Furthermore, when compared with conventional distal pancreatectomy with splenectomy, splenic preservation is associated with reduced estimated blood loss, decreased length of hospital stay, and decreased incidence of perioperative infectious complications. 11 This is consistent with our series, in which no patients required transfusions, median length of stay was 5 days, and no patients suffered from pancreatic fistula or infectious complications. Guidance for leaving an intraperitoneal drain is unsettled science and is beyond the scope of this study; we selectively utilized a large-bore multiperforated drain in two of our three reported operations. In the absence of a basis in evidence, we can only recommend that in select cases, surgeons may consider leaving a drain in the vicinity of the pancreatic stump to empirically manage any pancreatic fistulae that may arise.
Because splenic preservation compromises the radical resection that would be preferred for a higher-grade neoplasm, there should be a high level of certainty regarding SPN as the diagnosis preoperatively when this approach is planned. In many cases, a high index of suspicion will arise based on imaging characteristics. The tumor is typically well circumscribed and surrounded by a peripherally enhancing pseudocapsule of compressed pancreatic tissue and reactive fibrosis. 33 In some instances there are areas of internal hemorrhage or cystic necrosis, and calcifications are seen in up to one-third of adult tumors, but are rare in pediatric patients.20,33,34 In cases that are decidedly consistent with SPN based on imaging and clinical presentation, upfront resection without a tissue diagnosis is preferred. When the diagnosis is in question, a multidisciplinary review across specialties is valuable, as preresection biopsy could be considered if a spleen-sparing approach is planned. Alternatively, it would be reasonable to proceed with upfront distal pancreatectomy with splenectomy if there is concern for a high-grade malignancy.
In our series, due to preoperative diagnostic uncertainty in 2 cases, tissue was obtained before definitive resection by laparoscopic-assisted core needle biopsy and EUS-FNA, respectively. Laparoscopic biopsy has been used with caution for suspected SPN because of concern that tumor spillage may be responsible for recurrence. One 3-patient series of SPN in children described 100% recurrence of disease in their patients, each of whom underwent preresection laparoscopic biopsy. 35 In that series, 2 patients experienced peritoneal recurrence after a laparoscopic biopsy was performed with grasping forceps, and the third patient had a local recurrence after incomplete resection. In contrast, more recent data suggest that intraoperative tumor spillage, rather than preoperative biopsy, is responsible for SPN recurrence. 15 The risk of recurrence after laparoscopic-assisted core needle biopsy is unknown, and further investigation into the safety of preoperative laparoscopic biopsy for suspected SPN is needed.
Another emerging modality for acquiring a tissue diagnosis is EUS-FNA. Accuracy of EUS-FNA in diagnosing SPN has been assessed in adults, notably correctly identifying SPN in only 60%–70% of cases.1,34 However, complications rate is low at ∼1%. 36 As experience grows and diagnostic accuracy improves, EUS-FNA could provide a safe and relatively noninvasive modality for diagnosing SPN preoperatively. One patient in our study was correctly diagnosed with SPN using EUS-FNA. In our center, the procedure is performed primarily by adult gastroenterologists. This may limit broad application in children but should serve as motivation for increased advanced endoscopic training for pediatric surgeons and gastroenterologists.
The 3 patients in our study have been followed with surveillance ultrasound every 6 months after resection. There is no standardized protocol for postoperative follow-up of pediatric patients with SPN, but the average time to recurrence of this tumor is 4 years.1,17 Therefore, we plan to follow these patients for a minimum of 5 years. CT is another viable modality for surveillance and may be more sensitive in detecting small recurrences or peritoneal implants. However, duplex ultrasonography is radiation sparing and can assess splenic perfusion in our spleen-preserving series. Because recurrence is so rare, further research to determine the optimal postsurgical surveillance for SPN is needed.
In conclusion, SPN is a rare tumor in the pediatric population, but with appropriate management the prognosis is excellent. In our experience and that of the existing literature, laparoscopic spleen-preserving distal pancreatectomy is a safe and effective surgical approach. This approach achieves the margin negative resection that is appropriate for the disease with the additional benefits of minimally invasive surgery and splenic preservation. Therefore, laparoscopic distal pancreatectomy with splenic preservation is our preferred operation in adolescents presenting with SPN and can be performed in most, if not all, cases.
Footnotes
Disclosure Statement
No competing financial interests exist.