
Abstract
Abstract
Introduction:
Cryoanalgesia has been applied to minimally invasive repair of pectus excavatum (MIRPE). After implementation of cryoanalgesia at our institution, we had several cases of delayed postoperative pneumothorax. The purpose of this study was to critically evaluate the complications and efficacy of cryoanalgesia in MIRPE.
Materials and Methods:
We performed a single institution retrospective review of pediatric patients undergoing MIRPE from June 2017 to July 2018. Multimodal (MM) analgesia was used in all patients. In addition, most patients received either cryoanalgesia or elastomeric pain pumps (EPPs) as adjuncts to postoperative analgesia. Primary outcome was clinically significant late pneumothorax. Secondary outcomes included length of stay, pain scores, opiate use, and bar displacement requiring reoperation.
Results:
A total of 101 patients undergoing MIRPE were included: 45 had cryoanalgesia + MM, 45 EPP + MM, and 11 MM alone. Postoperative tube thoracostomy was placed in 5 patients with cryoanalgesia (4 pneumothorax; 1 effusion), 1 patient with EPP (1 pneumothorax), and none in MM alone (P = .25). Pain scores at discharge were similar in all groups. Cryoanalgesia patients received less overall inpatient opioids than other groups (P < .05). No patient required reoperation for bar displacement.
Conclusion:
Cryoanalgesia is an effective therapy for pain control in MIRPE. Because thermal injury can occur on the lung and chest wall with cryoanalgesia, we implemented techniques to limit and prevent this injury. Cryoanalgesia offers a safe alternative for postoperative analgesia with significant reduction in inpatient opioid requirement. Larger prospective studies are required to assess the long-term impact and complications of cryoanalgesia.
Introduction
Pectus excavatum is one of the most common chest wall deformities in children with an estimated occurrence of 1 in 400 to 1 in 1000 live births. 1 Historically, surgery to correct this chest wall deformity carried great morbidity. However, since its introduction in 1998, the minimally invasive repair of pectus excavatum (MIRPE), also called the Nuss procedure, has become the most common technique for the correction of pectus excavatum. This procedure offers a less invasive approach with smaller incisions, no cartilage resections or osteotomies, and a reduced operative time and hospital length of stay (LOS). 2
Despite the less invasive approach, some patients have reported significant postoperative pain resulting from the MIRPE, and the challenges of controlling this pain have been the primary determining factor affecting prolonged hospitalization.3,4 There is no universally accepted or standard protocol for pain management and many strategies have been applied. Pain intervention therapies have included thoracic epidural analgesia, patient-controlled intravenous (IV) analgesia, ultrasound-guided rib blocks, elastomeric pain pumps (EPPs), and multimodal (MM) pain management.3–7 The most recent major pain therapy applied to the MIRPE is cryoanalgesia. Based on the potential benefit of prolonged pain relief, cryoanalgesia has been adopted as an adjuvant pain therapy in minimally invasive pectus surgery.8–13
At our institution, we began using cryoablation in some of our pectus surgery patients in late 2017, and our initial adoption was complicated by several cases of significant pneumothorax that resulted in the placement of chest tubes during the postoperative hospital course. There have been no reports of cryoanalgesia related pneumothorax in pectus surgery. The purpose of this study was to describe our experience introducing cryoanalgesia to MIRPE, to compare postoperative complication rates, and to compare the efficacy of cryoanalgesia compared to our conventional pain management cohorts before the adoption of cryoanalgesia.
Materials and Methods
Patients and data collection
After approval from the Phoenix Children Hospital's Institutional Review Board (IRB-18-131), we conducted a retrospective review of all patients who underwent MIRPE at our institution between June 1, 2017 and July 30, 2018. Eight different pediatric surgeons performed these procedures. We excluded all the patients with a previous repair. Cryoanalgesia was adopted at our institution in December 2017. Demographic, operative, hospital, and outpatient data were recorded. Primary outcome was the presence of clinically significant late postoperative pneumothorax, which we defined as any symptomatic pneumothorax with tension physiology or a pneumothorax with complete or severe lung collapse and subsequently requiring intervention. Secondary outcomes included hospital LOS, inpatient IV and oral (PO) opioid use, and subjective patient analgesia as measured by visual analogue pain scores during the hospital stay.
Operative technique
The anesthesiologist placed a double-lumen endotracheal tube for each repair to allow for isolated ventilation. There were two main techniques in performing the operation, based on individual surgeon preference. In >90% of the cases, limited bilateral chest incisions were made and extended through the muscular layer with creation of submuscular pockets for the bar placements. Trans-mediastinal dissection was performed under thoracoscopic visualization and most patients received two bars to correct the defect. The pectus bars were secured to the chest wall with permanent braided sutures that were tied circumferentially around the ribs. The other technique utilized a subxiphoid counter-incision to aid in the subcutaneous and trans-mediastinal dissection and placement of the pectus bar, and the bar was stabilized with a lateral bar stabilizer. Thoracoscopy was used in every repair.
Cryoablation was performed under thoracoscopic visualization. Through a small opening in the interspace, the CryoICE Cryoablation Probe (AtriCure, Mason, OH) was introduced into the pleural cavity after the ipsilateral lung was deflated. The intercostal spaces were counted and the cryoablation probe tip was then placed at the inferior margin of the rib of the desired intercostal nerve to be ablated. The site chosen was always lateral to the sympathetic chain, and posterior to the future location of the pericostal fixation sutures (Fig. 1). Care was taken to avoid contact of the probe to the lung or pericardium. Gentle pressure was applied to the desired intercostal nerve and the probe was rapidly cooled to −60°C for 2 minutes. After the 2-minute cycle, the probe went through an active warming phase and the probe was gently taken off the tissue after thawing past 4°C. The probe was always passed through the ipsilateral side. We typically ablated the fourth through seventh intercostal nerves bilaterally. Before re-insufflating each lung, 2 minutes were allowed for thawing. In rare cases, the cardiac displacement on the left side prevented cryoablation of the seventh intercostal nerve.
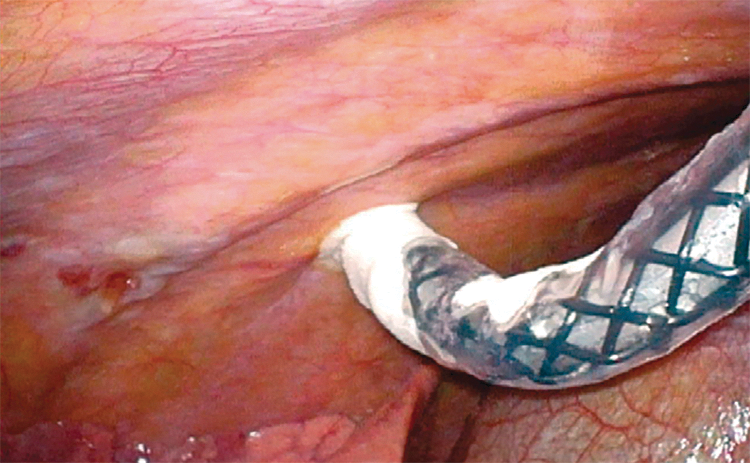
Right intrathoracic view of cryoICE probe placement over the intercostal nerve.
In patients not undergoing cryoanalgesia, the main adjunct pain therapy utilized was the intraoperative placement of elastomeric pump infusion catheters (On-Q Pain Relief System; Avanos, Irvine, CA) for continuous postoperative infusion of local anesthetic to the chest wall. Through small bilateral stab incisions, these catheters were tunneled within the chest wall. The elastomeric pumps were filled with 0.25% bupivacaine that was continuously infused a minimum of 48 hours postoperatively. These catheters were removed before hospital discharge.
Perioperative and postoperative pain control
The pain management strategy for pectus surgery included MM analgesia therapy, as per our published protocol.4,11 All patients received MM analgesia including general anesthesia, ketamine and dexmetomedine infusions, and a single dose of IV methadone. Patient-controlled analgesia (PCA) with either a demand-only or continuous plus demand infusion of hydromorphone (or fentanyl if allergic to hydromorphone) was initiated immediately after surgery. A clonidine patch was placed in the postanesthesia care unit. The PCA continuous infusion was stopped on postoperative day 1 and oxycodone 10–20 mg per day was started based on patient's weight and overall IV opioid use. Postoperatively, ketorolac and diazepam were administered as needed. Patients were then transitioned to ibuprofen, acetaminophen, and oxycodone before discharge. Gabapentin was typically initiated before surgery and continued in the postoperative period.
Statistical analysis
Demographic and clinical characteristics within each of the groups were reported as medians and interquartile ranges (IQRs) for continuous covariates and frequencies and percentages for categorical variables. The Kruskal–Wallis test compared the continuous covariates between the three groups, whereas chi-squared or Fisher's exact test compared categorical variables. Multivariable linear regression was used to ascertain estimated differences in morphine equivalence between the analgesia groups using MM analgesia as the reference group. Second, the multivariable linear mixed model calculated differences in pain scores between the analgesia groups over time. Both models were adjusted for age, gender, body mass index (BMI), LOS, correction index, total operating room/surgical time. Further adjustments of baseline pain scores were included in the linear regression model, whereas total morphine equivalence were added to the linear mixed model. Finally, the above described statistical methodology was used once again to compare the elastomeric + MM and cryoanalgesia + MM groups. The regression modeling was now using the elastomeric + MM group as the reference group. All P values were two-sided and P < .05 was considered statistically significant. All data analyses were conducted using STATA version 14 (STATAcorp, College Station, TX).
Results
Minimally invasive pectus repair was performed on 101 patients. We identified three analgesia management subgroups: cryoanalgesia + MM analgesia, elastomeric infusion pump catheters + MM analgesia, and MM analgesia-only therapy. In the study cohort, 45 patients were treated with cryoanalgesia, 45 with EPP, and 11 with MM therapy alone. Demographic data for each group are given in Table 1. There were no significant differences in age, BMI, Haller index, or correction index between groups. Patients presented with respiratory symptoms in almost 90% of all groups.
Demographics
Kruskal–Wallis test to compare continuous variables. Chi-squared/Fisher's exact to compare categorical variables.
BMI, body mass index; IQR, interquartile range; MM, multimodal.
The frequency of pneumothorax and pleural effusion ranged from 60% to 75% with no statistical significance among groups (Table 2). Most pneumothoraces were trivial, measuring <1 cm without clinical significance. During the hospital stay, 5 patients in the cryoanalgesia group (11%) underwent thoracostomy tube placement compared with 1 patient in the EPP group (2.3%). Most of the five cryoanalgesia tube thoracostomies occurred during the first few months of cryoanalgesia experience. Clinically symptomatic pneumothorax was the most common indication for drainage followed by large pneumothorax and symptomatic pleural effusion (Fig. 2). Four of 45 patients (9%) required chest tube thoracostomy for pneumothorax in the cryoanalgesia group. In the elastomeric pump group, thoracostomy was performed for one large pneumothorax. No patient in the MM group underwent a thoracostomy tube placement. Based on patient size and surgeon preference, an 8.5 or 10.2F pigtail thoracostomy drain was used. No needle aspirations or decompressions were attempted. There was no statistical difference for thoracostomy tube insertion between all groups (P = .25). Chest tubes were removed after a median time of 3 days (IQR = 2–3 days). There were no secondary complications after chest tube placement. All patients with evidence of pneumothorax underwent follow-up chest radiograph in clinic after 2 weeks demonstrating complete resolution.
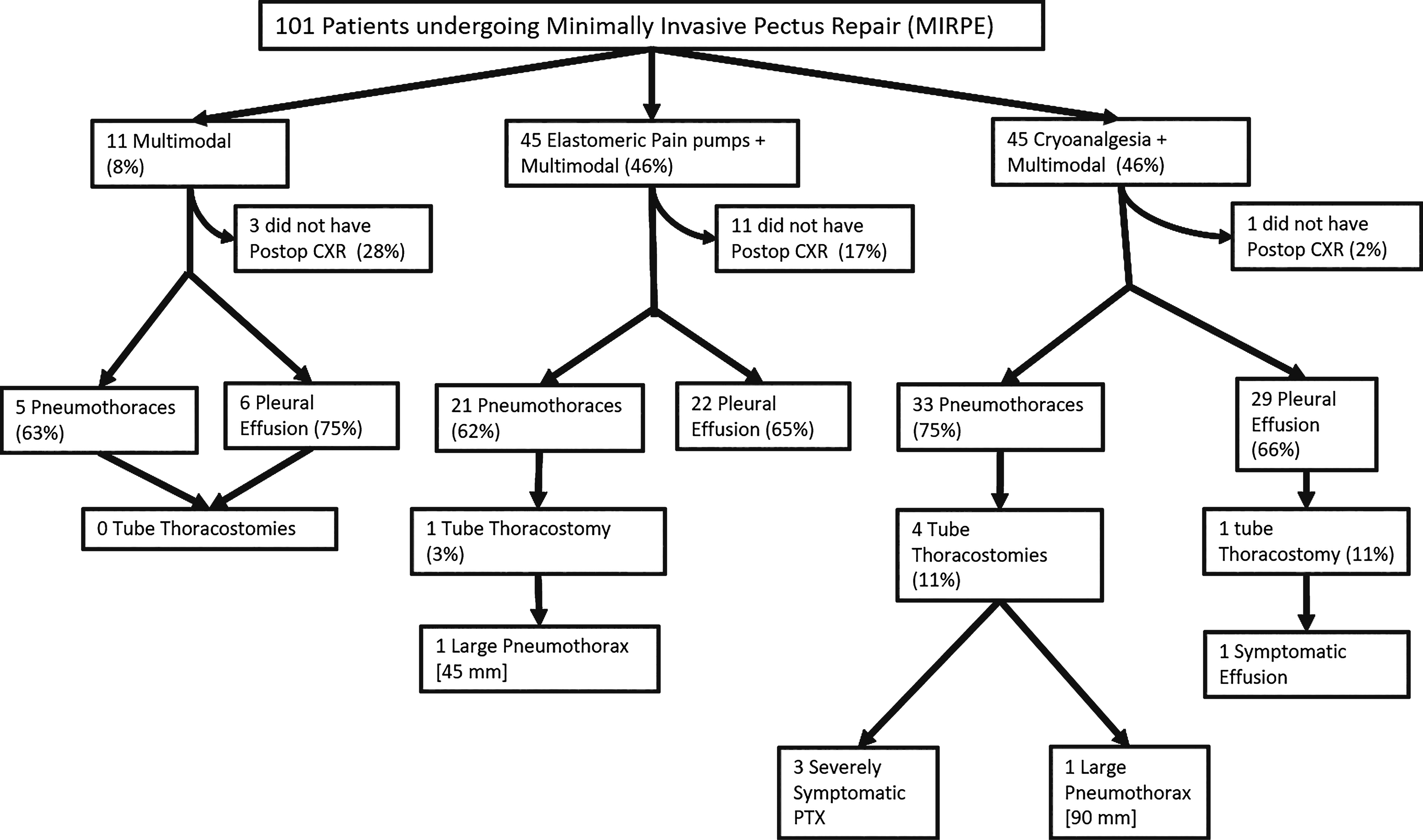
Study population and main outcome. CXR, chest radiograph; PTX pneumothorax.
Clinical Outcomes
Kruskal–Wallis test to compare continuous variables. Chi-squared/Fisher's exact to compare categorical variables.
IQR, interquartile range; LOS, length of stay; MM, multimodal; OR, operating room.
The median LOS for patients receiving cryoanalgesia was 3 (IQR = 3–4) versus 4 days for the EPP group (IQR = 3–4) and 4 days in the MM group (IQR = 3–4). Surgical time was slightly longer but not statistically different in both the cryoanalgesia and the EPP groups compared with MM-only group: 124 minutes (IQR = 107–144) and 118 minutes (IQR = 98–142) versus 108 minutes (IQR = 68–130) (P = .22). Two patients (4%) who received cryoanalgesia developed wound infection and 3 (7%) developed pneumonia. One patient (2%) in the EPP group also developed pneumonia. Median follow-up was 9.4 weeks (IQR = 5.8–13.3) for the cryoanalgesia group, 12.7 weeks (IQR = 9.8–15.3) for the elastomeric pump group, and 13.4 weeks (IQR = 6.9–16.7) for the MM group (Table 2).
Median pain scores throughout the hospital stay were similar between the cryoanalgesia (3.38 [IQR = 1.6–4.7]) and the elastomeric pump groups (3.41 [IQR = 2.1–4.6]), but lower in the cryoanalgesia group compared with MM analgesia-only group (4.5 [IQR = 3.6–5.5]). There was no statistical difference in the median pain scores among all groups (Table 3). Total inpatient opioid use was lower in the cryoanalgesia group (237 mg [IQR = 151–360]) compared with both EPP (357 mg [IQR = 268–471]) and MM-only groups (466 mg [IQR = 355–537]). When comparing cryoanalgesia with solely MM analgesia, there was a statistically significant decrease in total inpatient opioid use (P = .01) that was mostly attributable to IV opioids used (P = .01). When comparing cryoanalgesia with MM analgesia + EPP, there was also a statistically significant decrease in total inpatient opioid use (P = .02), mostly attributable to PO opioids used (P = .002) (Table 4).
Pain Scores Over Time
Model 1: Beta (95% CI) calculated using the linear mixed model to ascertain changes in VAS score over time adjusting for time and the patient-level random effect. Model 2: Beta (95% CI) calculated using the linear mixed model to ascertain changes in VAS score over time adjusting for time and the patient-level random effect with further adjustments for age, gender, BMI, LOS, surgical/total OR time, and total amount of morphine equivalents given.
BMI, body mass index; CI, confidence interval; IQR, interquartile range; LOS, length of stay; MM, multimodal; OR, operating room.
Amount of Opiates Needed (In Equivalent Milligrams of Morphine)
Exponentiated Beta (95% CI) calculated using the linear regression to ascertain differences in morphine equivalents adjusting for age, gender, BMI, LOS, correction index, total OR/surgical time, and baseline pain scores.
BMI, body mass index; CI, confidence interval; IQR, interquartile range; IV, intravenous; LOS, length of stay; MM, multimodal; OR, operating room; PO, oral; PRN, as needed.
Discussion
Because MIRPE is associated with significant postoperative pain, multiple modalities of pain control have been developed throughout the years.9,14–21 Cryoanalgesia has been used for a wide array of procedures including sciatica, articular pain, and open thoracotomies. 22 In the thoracotomy realm, the greatest advantage of cryoanalgesia over other methods of pain control is its prolonged period of efficacy, with the effect lasting at least 2–3 months. 23
Cryoanalgesia, also called cryoablation, refers to the localized freezing of peripheral nerves through application of a cryoprobe that achieves freezing temperatures by the Joule–Thomason effect. The freezing of the nerve axon causes axonotmesis, which prevents potentiation of neural impulse, providing analgesia. Wallerian degeneration of axons occurs, and the fibrous neural structure including the perineurium and epineurium remain intact, facilitating axonal regeneration.23–26 Animal studies have shown regeneration of myelin sheath is completed by ∼4–6 weeks.26,27 Concerns with cryoanalgesia include prolonged numbness and neuralgia or allodynia, which may occur during the axonal regeneration phase. There are some reports of relief of hypoesthesia at 6 months but the data remain unclear.26,28
Given the potential benefits of prolonged chest wall anesthesia, cryoanalgesia has been applied to MIRPE.8–10,12,13 In the literature, the technique of cryoprobe placement is varied. Most introduce the probe into the pleural space either from the ipsilateral or contralateral side and freeze the intercostal nerves from within the chest, whereas others advocate a subcutaneous tunneling of the probe into the intercostal space.8–10,12,13 The common ground is to perform the cryoablation under visualization.
At our institution, we faced some challenges upon implementing cryoanalgesia. After having our initial patients with delayed large symptomatic pneumothorax, we suspected that thermal lung injury was the cause. We noted that not only the tip but also the insulated portion might reach freezing temperatures and cause tissue damage to any soft tissue in direct contact with the probe (Fig. 3). We became more vigilant and ensured that the lung would not contact any portion of the insulated probe. In addition, we began to wait an additional 2 minutes after the last intercostal cryoablation before re-inflating the ipsilateral lung to allow the chest wall to thaw before contacting the lung surface. We believe that selective lung ventilation, placing the probe from the ipsilateral side and performing the cryoablation under direct visualization are important techniques in safely performing the procedure.

Left intrathoracic view of cryoICE probe placement on the intercostal nerve during the freezing period.
Pneumothorax is the most common complication of the minimally invasive pectus repair and has been reported to be from 0.3% to 66% depending on the case series.29–32 This wide discrepancy of pneumothorax rates reflects the variability in practice of obtaining chest radiographs after this operation. Most pneumothoraces after thoracoscopic surgery will resolve spontaneously and therefore, some authors advocate not routinely obtaining chest radiographs. A study carried out by Knudsen et al. 33 in 1000 patients concluded that a routine chest radiograph could be safely limited to obtaining one before discharge. The concern of performing a delayed chest radiograph is the development of progressive and tension pneumothorax; however, these occurrences tend to present with symptoms. The reported rate of pneumothorax requiring drainage of the chest cavity ranges from 4.5% to 9% and <4% for symptomatic pleural effusion. 30
In our series, most patients received a chest radiograph at the conclusion of the operation to check bar placement and to assess adequate evacuation of the pneumothorax. Any large residual pneumothorax resulted in additional chest radiographs before discharge. Due to a significant number of patients traveling to our institution from out of state for their repair, our tendency is to be aggressive in assessing resolution or minimal residual pneumothorax before discharge. While flying commercially has been demonstrated safe after thoracic surgery, management of pneumothorax at a distance provides angst for both the patient and surgeon. 34 In our study, the cryoanalgesia group had a postoperative pneumothorax rate requiring drainage of 9% (4 out of 45 patients). This was notable but was not statistically different from the other groups that did not receive cryoablation. Most of these pneumothoraces occurred early in our cryoanalgesia experience. One series looking at cryoanalgesia in the Nuss procedure reported having one hydropneumothorax requiring drainage. 9 However, no series has specifically looked at the complication of pneumothorax associated with the use of cryoanalgesia in pectus surgery.
Although not statistically significant, we had two wound infections in the cryoanalgesia group versus none in the other cohorts. Thermal injury to the skin and chest wall directly in contact with the cryoablation probe may have contributed to these wound infections. Techniques to protect the chest wall by partially covering the cryoprobe with a chest tube has been described and provides additional insulation. 12 We have also used gauze or retractors at the level of the skin during the freezing cycle to prevent any direct contact of the skin to the probe sheath (Fig. 4). Although updated versions of the cryoablation probe may have improved insulation, the surgeon should be conscientious of potential thermal injury of any tissue in contact with the probe.
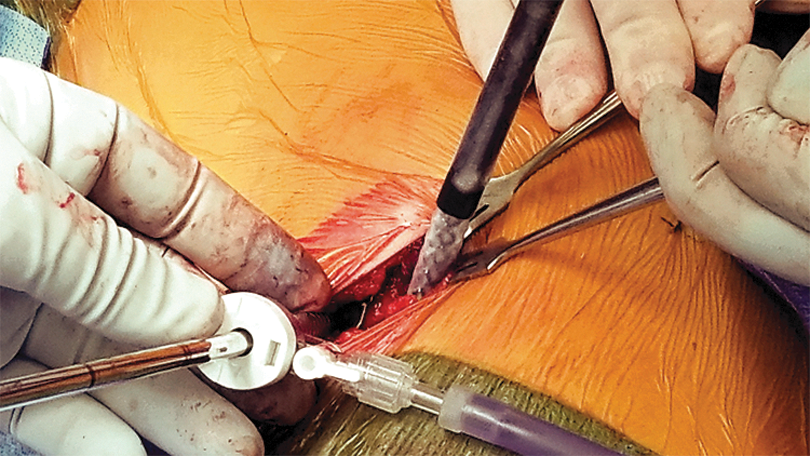
External view of the trocar and cryoICE probe placement with skin protection.
Our study is the largest single-center study of cryoanalgesia versus conventional pain management strategies in MIRPE in the pediatric population. Other studies have compared cryoanalgesia with thoracic epidural analgesia with reported decreased LOS and opiate use.8–10 We have previously demonstrated superior outcomes with MM analgesia and EPP compared with epidural analgesia in pectus surgery. 4 In our experience, the LOS when comparing cryoanalgesia with standard MM therapy was not statistically different. In our MM analgesia pathway, the patient is started on continuous PCA opioid infusion for the first 24 hours that is weaned as soon as possible to demand-only PCA. We have found that with cryoanalgesia, the continuous opiate infusion can be avoided, and the patient can be placed on demand-only PCA without any significant difference in pain scores. Overall, we found a significantly lower inpatient opioid use in the cryoanalgesia group.
Limitations
Our study is a nonrandomized retrospective study with its inherent limitations. Inevitably, there are minor variations in surgical technique among the 8 pectus surgeons. In addition, we found interpatient variability of pain tolerance and self-assessment of the pain score. There were not enough data to assess outpatient opioid consumption. Long-term effects of cryoanalgesia could not be clearly delineated given our median follow-up of 9 weeks.
Conclusions
Cryoanalgesia is an effective therapy for pain control in MIRPE. We experienced a slightly increased rate of pneumothorax when we began using cryoablation, but this increased pneumothorax rate was not statistically significant. Because thermal injury can occur on the lung and chest wall with cryoanalgesia, we implemented techniques to limit and prevent this injury. Cryoanalgesia offers a safe alternative for postoperative analgesia after pectus surgery with significant reduction in inpatient opioid requirement. Ongoing critical evaluation of long-term outcomes of cryoanalgesia is essential for ensuring optimal results in pediatric pectus excavatum patients.
Disclaimer
The views expressed in the submitted article are owned by the authors and are not the official position of an institution or funder.
Footnotes
Disclosure Statement
No conflicts of interest to be declared.