
Abstract
Abstract
Purpose:
Various studies have shown the benefit of three-dimensional (3D) systems over two-dimensional (2D) systems in endoscopic surgery. However, few studies have focused on pediatric endosurgery. The purpose of this study was to assess the impact of 2D and 3D environments on the time taken and forceps manipulation by comparing experts and trainees using a laparoscopic hepaticojejunostomy simulator.
Methods:
We have developed a simulator of laparoscopic hepaticojejunostomy for congenital biliary dilatation. Seventeen participants of pediatric surgeons (4 experts and 13 trainees) performed hepaticojejunostomy using our simulator in both 2D and 3D environment. We evaluated the required time, total path length, and average velocities of bilateral forceps in both situations.
Results:
Obtained results show the findings for the required time (seconds; 2D, experts: 810.43 ± 321.64 vs. trainees: 1136.02 ± 409.96, P = .17) (seconds; 3D, experts: 660.21 ± 256.48 vs. trainees: 1017 ± 280.93, P = .039), total path length of right forceps (mm; 2D, experts: 38838.23 ± 30686.63 vs. trainees: 52005.47 ± 31675.02, P = .48)(mm; 3D, experts: 24443.09 ± 12316.32 vs. trainees: 45508.09 ± 26926.27, P = .16), total path length of left forceps (mm; 2D, experts: 131635.54 ± 71669.94 vs. trainees: 245242.48 ± 130940.25, P = .48)(mm; 3D, experts: 88520.42 ± 56766.63 vs. trainees: 230789.75 ± 107315.85, P = .024), average velocities of right forceps (mm/second; 2D, experts: 44.80 ± 21.85 vs. trainees: 44.37 ± 18.92, P = .97) (mm/second; 3D, experts: 37.28 ± 16.49 vs. trainees: 42.58 ± 14.40, P = .54), average velocities of left forceps (mm/second; 2D, experts: 156.65 ± 38.69 vs. trainees: 202.58 ± 63.80, P = .20) (mm/second; 3D, experts: 125.64 ± 44.30 vs. trainees: 219.42 ± 43.82, P < .01).
Conclusion:
The experts performed more effectively when using the 3D system. Using 3D, the total path length of the left forceps of expert pediatric surgeons was significantly shorter than trainee pediatric surgeons, and the average velocities of the left forceps tip of expert pediatric surgeons was significantly slower than trainee pediatric surgeons. These results suggest that training of assisting hand is necessary for advanced pediatric endosurgery to avoid organ injury.
Introduction
Several studies have described the benefits of three-dimensional (3D) systems over two-dimensional (2D) ones in endoscopic surgery.1,2 Poudel et al. 2 reported that the 3D environment helped shorten the training time of laparoscopic skills. In pediatric surgery, sometimes it becomes a problem, as technical improvement of endosurgery for pediatric surgeons is difficult because there are few cases. We therefore believe that 3D environments have the potential to be very useful for pediatric surgeons. However, few studies have focused on the utility of 3D systems in the field of pediatric endosurgery.
Recently, in the field of pediatric surgery, laparoscopic surgery for congenital biliary dilatation (CBD) has become popular. However, except for some Asian countries, the number of cases performed per institution is less at present because it is a rare disease, hence making it difficult to standardize and improve the technique through the accumulation of cases. Therefore, the development of a simulator capable of reproducing a disease-specific surgical procedure and a training regimen using that system have attracted attention. 3 We have developed a simulator of laparoscopic hepaticojejunostomy for CBD.
The purpose of this study was to assess the impact of 2D and 3D environments on the time required and forceps manipulation ability through a comparison between experts and trainees using a laparoscopic hepaticojejunostomy simulator.
Materials and Methods
The simulator of laparoscopic hepaticojejunostomy for CBD with a surgical skill validation system
We developed this evaluation model in collaboration with Kyoto Kagaku Co., Ltd. We developed and reported a 1-year-old infant body model (body weight 10 kg) based on computed tomography data and reproduced a pneumoperitoneum body model based on the clinical situation, as shown (Fig. 1a). 4
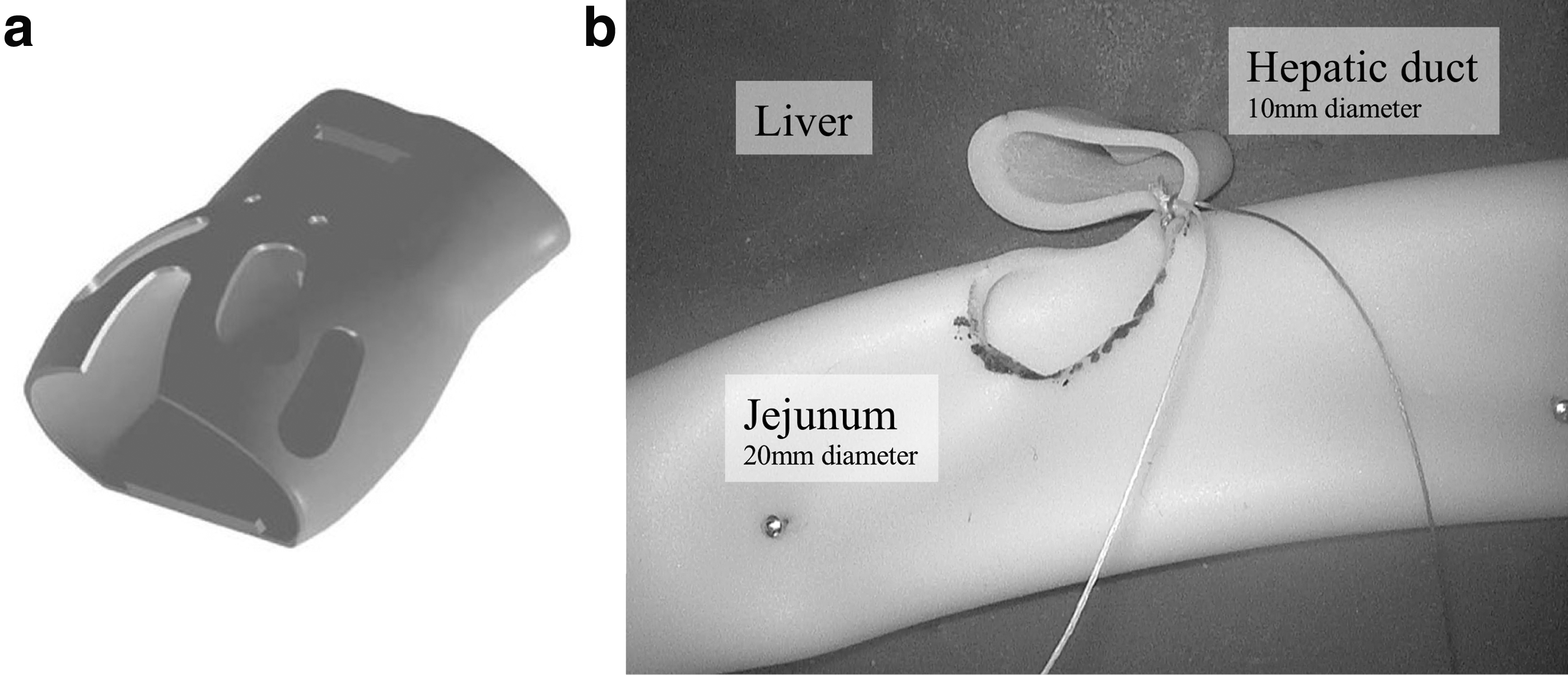
A hepatic duct (10 mm diameter), jejunum (20 mm diameter with 100 mm diameter defect for anastomosis), and liver were placed in this model (Fig. 1b).
The hepatic duct, jejunum, and liver were made of urethane. The pneumoperitoneum model was covered with synthetic skin.
A 0° 3D and 2D switchable scope 10 mm in diameter (IMAGE1 S™; KARL STORZ SE & Co. KG, Tuttlingen, Germany) was fixed using an arm. TrakSTAR® (Northern Digital, Inc., Ontario, Canada) was used as the 3D position measuring instrument and placed on the thoracic side of the model to trace the tips of the forceps. The right and left forceps had sensors mounted on the tips, and their paths were traced on a computer with an electromagnetic tracking system, as was reported previously. 5
Tasks for participants
The participants had to perform hepaticojejunostomy. The port layout was the right para-axial position. The trocar for the right hand was placed at the right lower lateral abdomen, and that for the left hand was placed at the right upper lateral abdomen. The trocar for the scope was placed at the umbilicus (Fig. 2).
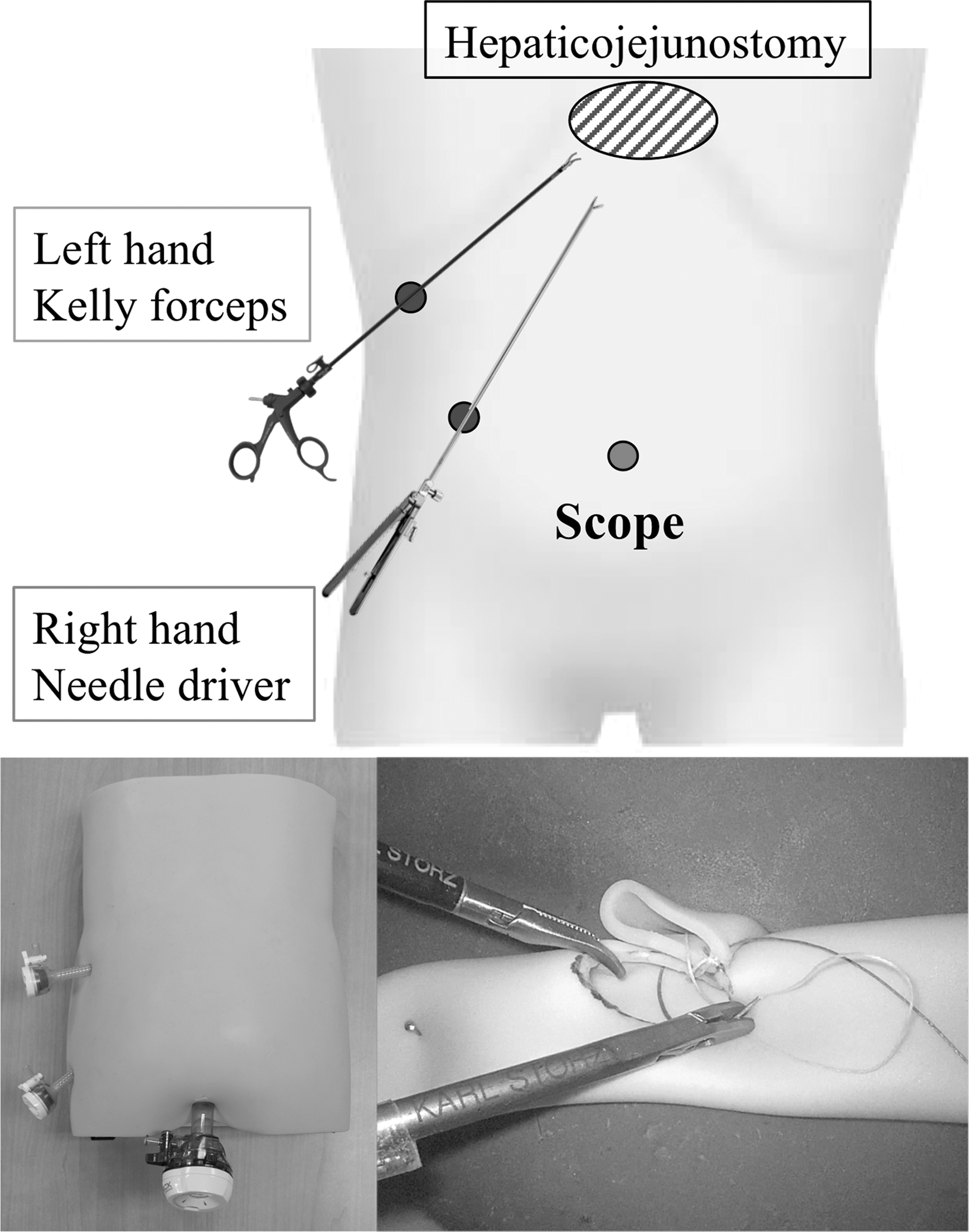
A schematic illustration showing the port layout of the simulator and a laparoscopic view of the simulation of hepaticojejunostomy.
The participants used a 3.5 mm needle driver on the right hand and 3.5 mm Kelly-type forceps (KARL STORZ SE & Co. KG) on the left hand. The suture material used was an RB-1 curved needle with white and purple VICRYL® (Ethicon Endosurgery, Cincinnati, OH). Each suture was cut to 8 cm, two sutures were tied together to create a 16 cm double-ended needle (Fig. 3).
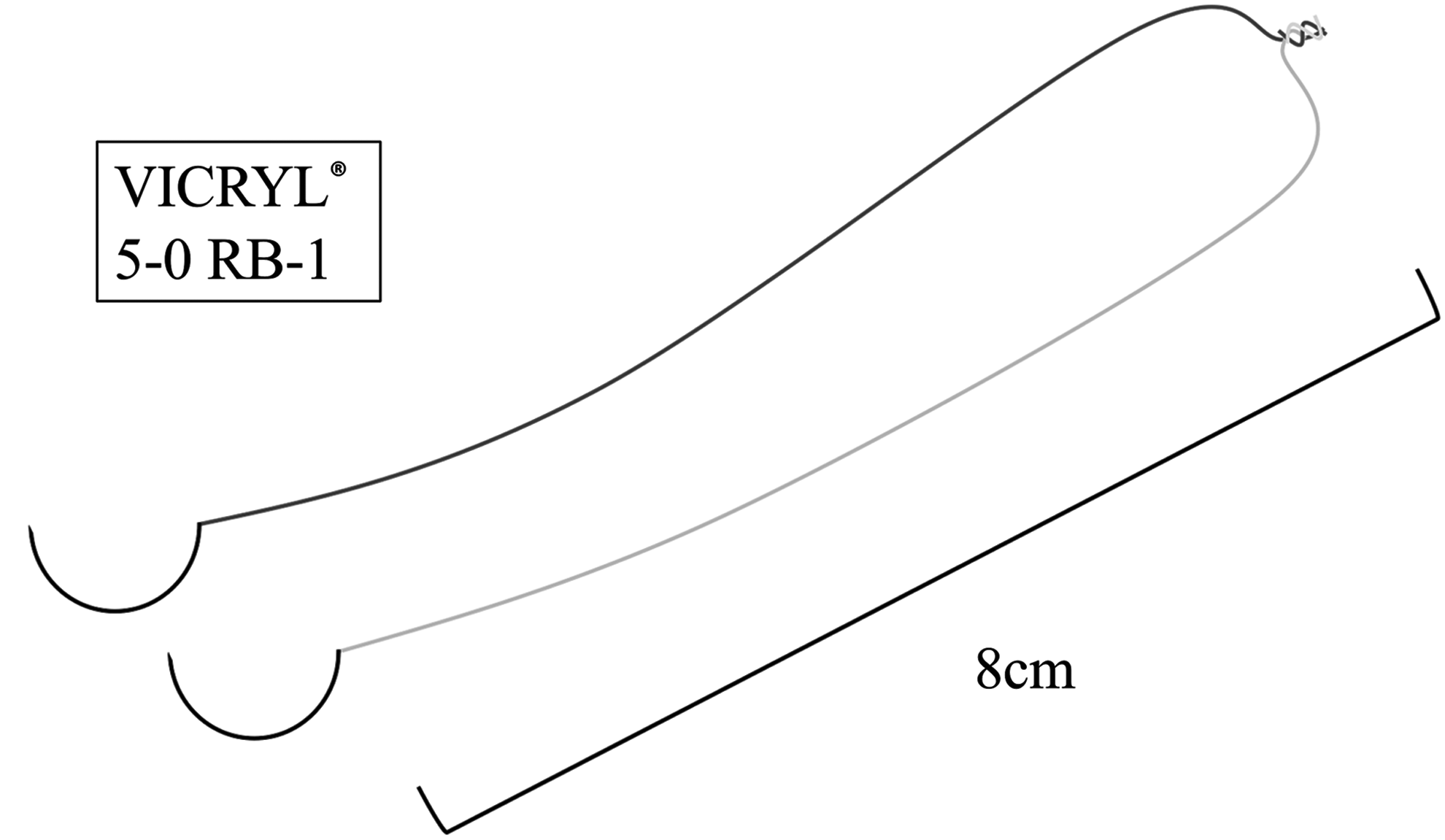
A schematic illustration of 16 cm double-ended needle.
Before starting the tasks, the left side of the hepatic duct and left side of the defect hole on the jejunum were tied using sutures (Fig. 4a). The participants had to perform anastomosis with running sutures and finally finished after performing intracorporeal knot tying twice at the right side of the anastomosis (Fig. 4b, c).
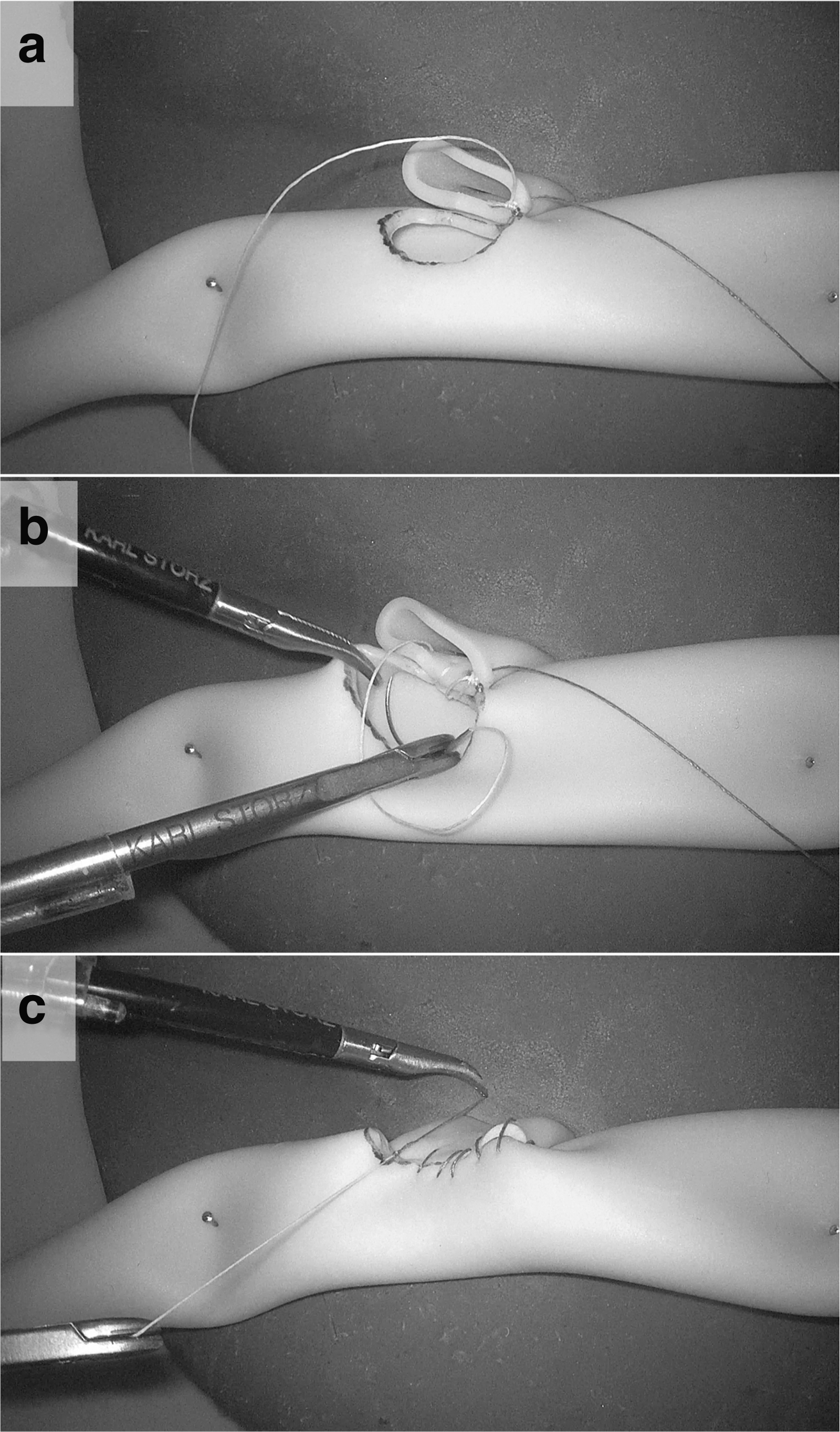
Task process.
Each participant had to perform these tasks twice in total: once in a 2D environment and once in 3D environment. The order of 2D and 3D had been randomized. The randomization used the block randomization method. Each participant could not know which their order was before starting the tasks.
Study participants
Table 1 provides the background of the participants. A total of 17 pediatric surgeons participated in this study. They were participants of the 34th Japanese Society of Pediatric Surgeons Fall Symposium & Pediatric Surgery Joint Meeting 2018. The examinees were divided into two groups, which included pediatric surgery experts and pediatric surgery trainees. The number of their experiences for laparoscopic hepaticojejunostomy was collected from the questionnaire to choose from “0” or “1 to 5” or “over 6,” and those who selected “over 6” were classified as experts. The expert pediatric surgeon group included 4 pediatric endoscopic surgeons and the trainee pediatric surgeon group included 13 pediatric endoscopic surgeons. One expert pediatric surgeon and 1 trainee pediatric surgeon were left-handed, but all other surgeons were right-handed. Three expert pediatric surgeons had endoscopic surgical skill qualification of Japan Society for Endoscopic Surgery, and no trainee pediatric surgeon had that qualification. All participants provided their informed consent.
Back Ground of the Participants
Endoscopic surgical skill qualification system from Japan Society for Endoscopic Surgery.
Assessment points
The assessment points were as follows, improving upon the methods previously reported by Uemura, Jimbo, and Ikee.6–8 We did not evaluate the quality of the anastomosis, because we had not established an objective evaluation method.
1. Time required to complete the task
The required time, which was defined as the performance time from the start to completion of the task, was measured in seconds.
2. Total path length of each forceps
The total path length of each forceps was considered to be the total spatial movement measured in the task in millimeters and was determined using the TrakSTAR system.
3. Average velocity of each forceps tip
The average velocity of each tip of the forceps was measured using the TrakSTAR system and defined as the velocity for each 0.05 seconds in the task.
Statistical analyses
All data were expressed as mean ± standard deviation. Two-tailed unpaired Student's t-test and analyses of variance were conducted for comparisons using R version 3.5.2 (R Core Team 2018). All data were defined as being statistically significant at P < .05.
Results
All participants completed the task, and the results of the skill evaluation are described hereunder (Table 2).
Results of the Tasks
Significant difference.
2D, two-dimensional; 3D, three-dimensional.
Time required to complete the task
There were no significant differences in the time required to complete the task using a 2D system between expert and trainee pediatric surgeons (P = .17), but using a 3D system, the time of expert pediatric surgeons was significantly shorter than trainee pediatric surgeons (P = .039).
Total path length of each forceps
There were no significant differences in the total path length of the right forceps between the expert and the trainee pediatric surgeons using a 2D (P = .48) and a 3D (P = .16) system.
There were no significant differences in the total path length of the left forceps using a 2D system between the expert and the trainee pediatric surgeons (P = .48), but using a 3D system, the total path length of left forceps of the expert pediatric surgeons was significantly shorter than the trainee pediatric surgeons (P = .024).
Average velocities of each forceps tip
There were no significant differences in the average velocities of the right forceps tip between the expert and the trainee pediatric surgeons using a 2D (P = .97) and a 3D (P = .54) system.
There were no significant differences in the average velocities of the left forceps tip using a 2D system between the expert and the trainee pediatric surgeons (P = .20), but using a 3D system, the average velocities of the left forceps tip of the expert pediatric surgeons was significantly slower than the trainee pediatric surgeons (P < .01).
Discussion
The purpose of this study was to assess the impact of 2D and 3D environments on the time required and forceps manipulation ability through a comparison between experts and trainees using a laparoscopic hepaticojejunostomy simulator.
We used three assessment points to evaluate the endoscopic surgical skills of the participants, as described in our previous report.4–8
We made several major findings in this study. First, there were no significant differences in the time required to complete the task using a 2D system between the experts and the trainees group, but using a 3D system, the time required to complete the task in the expert pediatric surgeons was significantly shorter than that of trainee pediatric surgeons. Second, in the total path length and the average velocities of the right forceps, there were no significant differences between the expert and the trainee pediatric surgeons using a 2D and a 3D system. However, using a 3D system, the total path length of the left forceps in the expert pediatric surgeons was significantly shorter than that of the trainee pediatric surgeons, and the average velocities of the left forceps tip in the expert pediatric surgeons was significantly slower than that of the trainee pediatric surgeons.
In our study, the time required to complete the task in the expert pediatric surgeons was shorter than the trainee pediatric surgeons using a 3D system.
Harada et al. 9 reported that a 3D system improves efficiency and dexterity with simple tasks. In our study design, the movement of the left hand (supportive use) is simpler than the movement of the right hand (suturing). So, we considered that the impact of a 3D appeared in expert performance, such as the required time and the movement of the left hand.
Ieiri et al. 10 reported that a shorter path length and slow manipulation increased the quality of endoscopic procedures. This report shows that the average velocity of the forceps gets slower and the path length gets shorter as surgeons become more skilled.
In this study design, the right forceps was the needle driver, and the left forceps was a Kelly-type device used to assist the right hand. The results of this study show that it is more difficult to control the movement of assist hand than suturing hand.
The port layout of this task was right para-axial position. So, the participants needed to control their left hand forceps close to the liver. These results suggested that if the movement of supporting forceps was not well controlled, there was a risk of organ injury.
A previous report suggested that pediatric surgeons were able to perform endoscopic procedures with the same quality as general surgeons after short-term training.10–12 In addition, Tomikawa et al. 7 showed the effectiveness of training on both spatial path lengths and average tip speeds in the left hand were particularly significant.
In conclusion, the experts performed more effectively when using the 3D system. The movement of assist hand in the trainee was too fast and too long. Trainee pediatric surgeons should train to be able to move their assist hand more slowly and simply to be an expert pediatric surgeon.
Footnotes
Acknowledgments
We thank MC Medical, Inc. (Tokyo, Japan) and Mr. Aida for renting us the 3D laparoscopic system for the study.
Disclosure Statement
The authors received rental services of the 3D laparoscopic system from MC MEDICAL Inc. All authors have no conflicts of interest or financial ties to disclose.
Funding Information
This study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS: 19K10485, 19K09150, 19K09078, 19K03084, 19K18061, 19K17304, 19K18032, 18K08578, 18K16262 17K10555, 17K11514, 17K10183, 17K11515, 16K10466, 16K10094, 16K10095, 16K10434, 16H07090).