
Abstract
Abstract
Background:
Both medical weight management (MWM) and bariatric surgery are significantly underutilized by patients with severe obesity, particularly males. Less than 30% of participants in MWM programs are male, and only 20% of patients undergoing bariatric surgery are men.
Objectives:
To identify motivations of males who pursue either MWM or bariatric surgery.
Setting:
Interviews with males with severe obesity (body mass index ≥35 kg/m2), who participated in a Veteran Affairs weight loss program in the Midwest.
Materials and Methods:
Participants were asked to describe their experiences with MWM and bariatric surgery. Interviews were audio-recorded, transcribed, and uploaded to NVivo for data management and analysis. Five coders iteratively developed a codebook using inductive content analysis to identify relevant themes. We utilized theme matrices organized by type of motivation and treatment pathway to generate higher-level analysis and generate themes.
Results:
Twenty-five males participated. Participants were 58.7 (standard deviation 8.6) years old on average, and 24% were non-white. Motivations for pursuing MWM or surgery included a desire to improve physical or psychological health and to enhance quality of life. Patients seeking bariatric surgery were motivated by the fear of death and felt that they had exhausted all other weight loss options. MWM patients believed they had more time to pursue other weight loss options.
Conclusion:
The opportunity to improve health, optimize quality of life, and lengthen lifespan motivates males with severe obesity to pursue weight loss treatments. These factors should be considered when providers educate patients about obesity treatment options and outcomes.
Introduction
Severe obesity (body mass index [BMI] of ≥35 kg/m2) is associated with numerous health conditions, including cardiovascular disease and type 2 diabetes. 1 The main treatments for weight loss are medical weight management (MWM), including dietary and physical activity changes with or without weight management medication or bariatric surgery. Both MWM and bariatric surgery are significantly underutilized, particularly by men. One recent systematic review found that only 27% of participants in MWM programs were male. 2 Only 15% of weight management medication users are males. 3 Fewer than 1% of patients who meet BMI criteria for bariatric surgery undergo surgery; only 20% of those patients are male. 4
Literature is lacking regarding the motivations of males with severe obesity, who pursue either MWM or bariatric surgery. Two mixed-gender studies discussed subanalyses of male motivations for MWM such as wanting to improve overall physical health and well-being, as well as the desire to have an ideal body image.5,6 Studies on male motivations for seeking bariatric surgery are limited by low numbers of male patients. Several mixed-gender studies reported subanalyses of male patients' motivations for pursuing bariatric surgery, including medical conditions and health concerns, weight stigma, and reduced work functioning.7–9
In this study, we analyzed 25 semistructured interviews with male Veterans with severe obesity, who participated in a Veteran Affairs (VA) weight loss program. We also identified and described patient motivations for pursuing either MWM or bariatric surgery.
Materials and Methods
Study population
This report is a secondary analysis of patient interviews that were conducted as part of a study investigating barriers and facilitators of severe obesity treatment within the VA. We conducted qualitative interviews with Veterans with severe obesity, who participated in a VA MWM program (MOVE!), which involves individual visits with patients or group classes on nutrition, exercise, and goal-setting.
We identified patients through an administrative data pull of electronic health records. We included Veterans from two VA Medical Centers in the Midwest, who met the following criteria for bariatric surgery: (1) BMI of 35.0–39.9 kg/m2 accompanied by an obesity-related comorbidity (coronary artery disease, dyslipidemia, hypertension, diabetes, gastroesophageal reflux disease, and obstructive sleep apnea and (2) BMI ≥40 kg/m2. We excluded Veterans older than 70. Patients who participated in VA MWM were eligible if they attended at least three MOVE! visits, with the first visit being 6–18 months before the initiation of the study. This allowed us to target patients who participated in the MOVE! program long enough that they could have been evaluated for bariatric surgery. The ICD-9 codes and MOVE! visit criterion are listed in Appendices 1 and 2, respectively.
Patients who pursued bariatric surgery were eligible if they were referred for bariatric surgery and/or underwent bariatric surgery, and attended at least one visit within MOVE! between January 1, 2011, and June 1, 2016 (Appendix 3). Extracting data from this longer time period allowed us to obtain an adequate sample size of patients who underwent bariatric surgery.
Data collection
Veterans were sent recruitment letters asking them to participate in a 60-minute semistructured interview. We obtained verbal consent for phone interviews and written consent for in-person interviews. Participants were asked to describe their experience with weight loss treatment options, their motivations for pursuing bariatric surgery or MWM, and their experience with treatment compared to their goals. Interview guides are shown in Appendix 4.
Data analysis
Interviews were audio-recorded, transcribed. and uploaded to NVivo for data management and analysis. 10 We analyzed the data using conventional content analysis, which included both emergent codes and a priori codes based on our research questions. 11 Four members of the research team coded 10% of transcripts independently to develop the initial codebook. We used memos and annotations to facilitate our analysis. After initial coding, the group convened to discuss the codes and determine code definitions. This procedure was repeated for each subsequent transcript, using the technique of constant comparison to finalize our codebook. 12 After finalizing the codebook, 3 coders (S.A.J., E.A., and G.S.) independently coded the remaining transcripts. We extracted the codes “motivations for surgery” and “motivations for weight loss” and utilized theme matrices tabulated by type of motivation and treatment (MWM or bariatric surgery) pathway to conduct higher-level analysis and generate themes. 13
The study was approved by the UW-Madison Institutional Review Board (IRB) and the William S. Middleton VA Research & Development Committee (VA R&D).
Results
As shown in Figures 1 and 2, 743 and 348 Veterans were identified through an administrative data-pull for our MWM or bariatric surgery groups, respectively. Twenty-nine patients participating in MOVE! and 26 patients who were referred for bariatric surgery contacted the study team in response to recruitment letters. Of the 55 interested patients, 25 were scheduled and interviewed. As seen in Table 1, MWM patients were more likely to be black (27% versus 14%), have a graduate degree or higher (36% versus 21%), and have a house income greater than $100,000 (18% versus 8%).
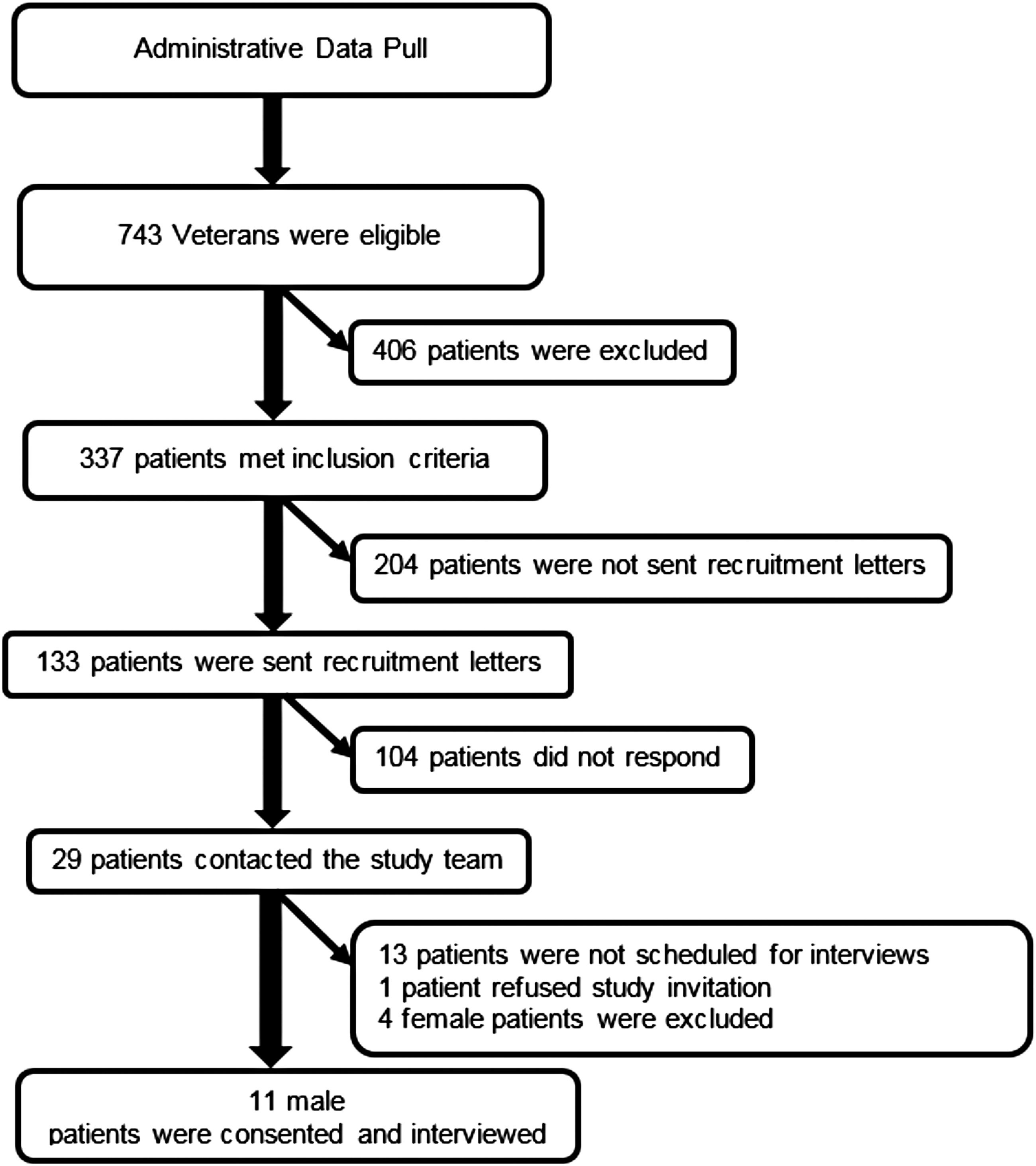
Recruitment of male veterans participating in a medical weight management program.
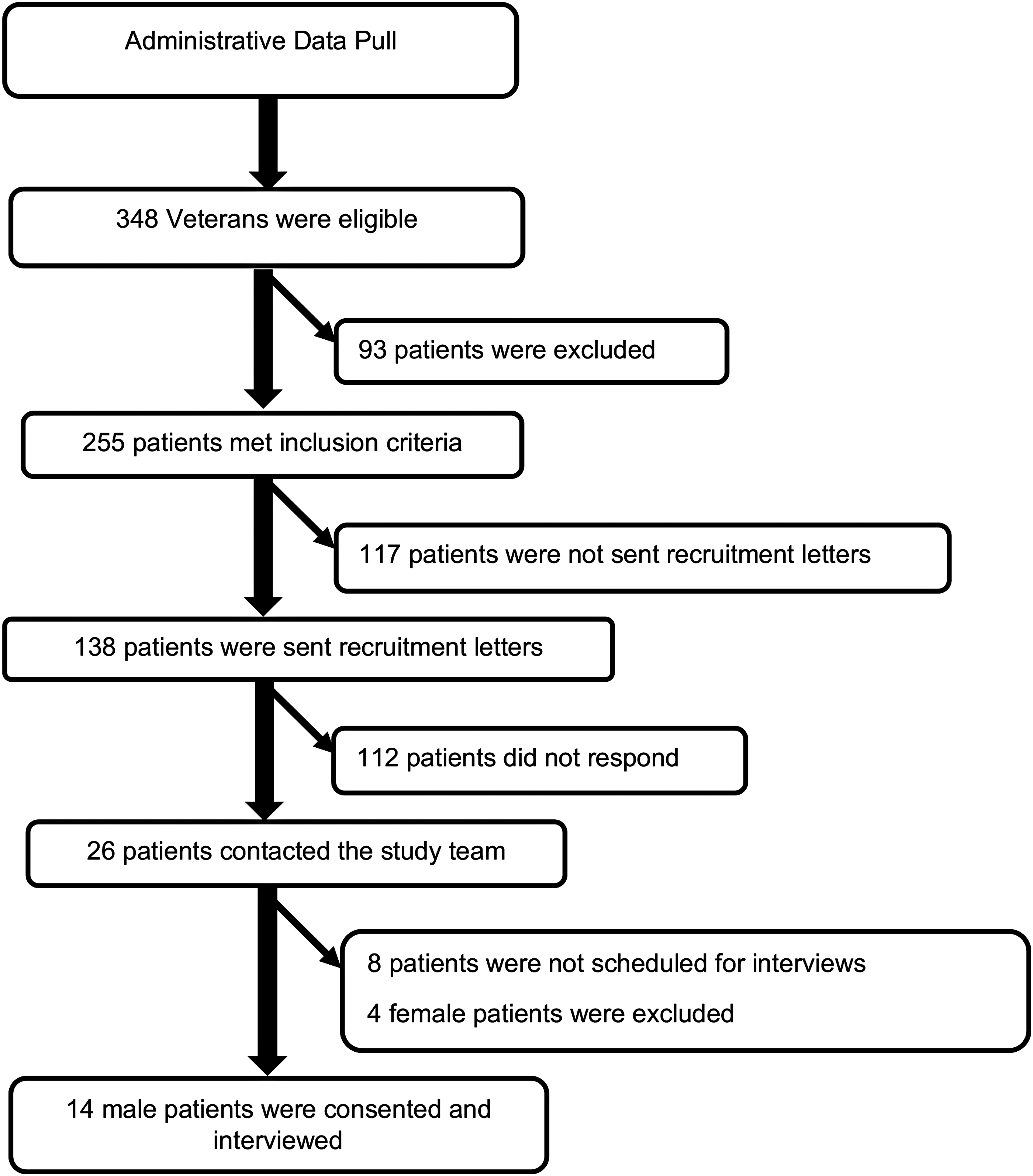
Recruitment of male veterans referred for bariatric surgery.
Characteristics of Male Veterans Who Participated in Veteran Affairs Medical Weight Management Program or Who Were Referred for Bariatric Surgery
MWM, medical weight management; SD, standard deviation.
Three themes emerged among both groups: (1) improving physical health, (2) improving psychological health, (3) and enhancing quality of life. Two themes were present among patients seeking bariatric surgery: (1) fear of death (2) and having exhausted all other weight loss options. Patients pursuing MWM expressed a sense of control over their weight and wanted to exhaust other weight loss options before considering bariatric surgery. In contrast, patients pursuing bariatric surgery described their experience as “running out of time” to recover the health that they had lost. Each theme along with representative quotes is characterized in Table 2.
Quote Matrix of Patients Pursuing Medical Weight Management or Bariatric Surgery
MWM, medical weight management; y/o, years old.
Improving physical health
Patients pursuing MWM spoke of “controlling” their weight, diabetes, or getting “a better handle” on their heart disease. MWM patients also described their desire to avoid medications. Motivations of patients pursuing MWM focused more on prevention of future health issues or worsening of current health concerns, while patients pursuing bariatric surgery focused on directly intervening to stop physical health issues. For example, patients pursuing bariatric surgery spoke of “getting rid of” physical health issues such as diabetes or sleep apnea.
Improving psychological health
Both groups discussed their loss of interest in performing daily activities and symptoms of depression as reasons to participate in treatment. Both groups of patients also discussed their desire to improve their body self-image and self-esteem. Patients in the MWM group had difficulty accepting their physical body image as they gained weight. In contrast, patients interested in bariatric surgery described the stigma of obesity. They also described obesity as a barrier to their self-esteem and achieving a normal life.
Enhancing quality of life
Both groups described wanting to be more active. Patients in the MWM group described wanting to return to activities in which they previously participated and to feel more comfortable performing daily activities. Patients referred for bariatric surgery discussed their inability to perform certain daily activities such as walking or playing with their children as motivators to pursue bariatric surgery. Both groups described their fears of being physically limited by their weight. Patients pursuing MWM discussed their fear of losing physical independence. Patients pursuing bariatric surgery described the loss of their physical independence in their daily lives.
Another motivation to improve quality of life was the desire to reduce chronic joint pain and gain mobility. Only the MWM group expressed the desire not to be a physical burden on others as a motivator for weight loss.
Fear of death
Fear of death as a result of obesity-related health issues was a strong motivator for patients in the bariatric surgery group as they shared a conviction that they would die if they did not lose weight. One patient discussed the fear of having an acute health-related issue he could not recover from. Another patient described how difficult his life had become due to chronic respiratory issues, which motivated him to consider surgery, “Nothing could be as worse as I was going through. This is a chance to get some help, let's do it (age 68, surgery).” Fear of death was not a theme that was present among patients participating in MWM.
Having exhausted all other weight loss options
Patients pursuing bariatric surgery described failing multiple weight loss attempts, which included diet, physical activity, and weight loss medications. Bariatric surgery patients had exhausted all other weight loss options and were motivated to try a more permanent weight loss method to recover their health. If they did not pursue surgery and continued down their current path, they feared they would die.
In contrast, when asked if bariatric surgery was a weight loss option they would consider, patients in the MWM group did not feel a sense of urgency and felt they had not yet exhausted all of their weight loss options. Many patients in the MWM group believed that their weight was not high enough to consider surgery. Other patients felt that they could still lose weight on their own with diet and exercise or weight loss medications. One patient commented, “I'd like to try to do this without [surgery]. A pill, I could understand. So, I can go along with that. I like trying it first” (age 60, MWM).
Discussion
We investigated motivations to pursue MWM or bariatric surgery among men with severe obesity. Both groups were motivated by the desire to improve their physical and psychological health and enhance their quality of life. Patients who were referred for bariatric surgery were motivated by the fear of death and by having exhausted all weight loss options. MWM patients wanted to attempt other weight loss options before considering bariatric surgery.
Both MWM and bariatric surgery patients placed importance on physical health and independence. Bariatric surgery patients wanted to gain back the physical independence they had lost, while MWM patients feared losing the physical independence they currently maintained. Hankey's single-gender study of interviews of males with overweight and obesity revealed that improving physical health was a key motivating factor for weight loss. 14 Brink and Ferguson's qualitative interviews with participants with overweight and obesity had similar findings, describing maintaining physical health as an impetus for losing weight. 6 One mixed-gender study by Peacock et al. regarding the experiences of people with severe obesity pursuing bariatric surgery found that quality of life centering on physical health was the most frequently reported motivation for surgery. 15
Both bariatric surgery and MWM study groups placed an importance on improving psychological health. Other studies have found psychological health to be an important motivator. In their mixed-methods study, Munoz et al. found that participants with severe obesity, seeking bariatric surgery, were motivated to improve their body image and self-esteem. 16 Similarly, Wee's secondary analysis of patients with severe obesity found that males pursued bariatric surgery due to experiencing weight stigma. 9 However, no single-gender study of men with severe obesity describes improving psychological health as a motivator for seeking bariatric surgery. Improving body image is less common as a motivator for patients seeking MWM in the literature. Yoong's mixed-gender survey study assessing normal, overweight, and obesity-related patients' motivations for MWM reported that <4% of patients with obesity chose improving appearance as a primary motivator for weight loss. 17 In interviews with people with overweight and obesity, Al-Mohaimeed et al. found that the desire to have an ideal body image was a primary motivator for only 16% of its participants. 5 Only 2 males with obesity mentioned appearance as a motivator for weight loss in Brink and Ferguson's mixed-gender study among 76 men who were seeking to lose weight. 6 Hankey's secondary analysis reported that “improved appearance” was the primary reason for weight loss for men 30–40 years of age, while younger men (18–29 years old) ranked this second. 14
Both MWM and bariatric surgery patients in our study cited quality of life as a driving force for pursuing weight loss. Improving physical health and body image were the two biggest drivers for males with obesity seeking MWM in Al-Mohaimeed's mixed-gender study. 5 Patients described being motivated to seek MWM by improving quality of life, and in particular, by their increasing loss of independence, which supports our study findings. 5 Two mixed-gender studies noted that functionality was a motivator for participants with obesity and severe obesity pursuing bariatric surgery.8,9 In particular, Wee found that males were motivated by poor physical functioning. 9
Our study supports existing mixed-gender literature suggesting that patients were motivated to pursue surgery to prevent death or extend their lifespan. 15 Nevertheless, literature on fear of death as a motivator to pursue surgery is limited and there are no single-gender studies that describe the fear of death among males. Patients pursuing MWM believed that they had not exhausted all other options and wished to lose weight without surgery. This is described by Wharton's mixed-gender survey study, in which patients with severe obesity, who pursued MWM rather than bariatric surgery, were confident of future weight success using a nonsurgical option. 18 No single-gender study discusses exhausting all other weight loss options as a motivation for seeking MWM.
Identifying and understanding the motivations of males pursuing obesity treatment options are critical because these findings can inform providers about what matters to patients who are considering obesity treatment. Patients pursuing bariatric surgery described their experiences with failing physical health and deteriorating quality of life. They also discussed their fear of death. Providers can apply these patient stories to weight loss treatment conversations with patients. Further, a better understanding of patient motivations will allow providers and researchers to develop and test educational interventions designed to improve obesity treatment decision-making. For example, information about how quality of life may improve with bariatric surgery or MWM would be important to include in this type of intervention because patients have indicated that it is important to them.
This study has several limitations. Our population comprised older male Veterans, who are not representative of the typical bariatric surgery patient in the United States. Veterans have more economic hardship, service-connected disabilities, and higher illness burden. 19 In addition, MOVE! is an MWM program that is unique to the VA. While the core goals of promoting behavioral changes coupled with other treatment options likely align with the goals of other MWM programs, there may be programmatic differences that affect the representativeness of our MWM experience.
Our results demonstrate that multiple factors motivate males with severe obesity to pursue weight loss treatments, including improving physical and psychological health and enhancing quality of life. Bariatric surgery patients were also driven by a fear of death and felt they had exhausted all other weight loss options. MWM patients believed they had more time to pursue other treatment options. These factors should be discussed when providers are educating patients about the obesity treatment options and outcomes.
Footnotes
Acknowledgments
Effort on this study and article was made possible by an American College of Surgeons George H.A. Clowes Career Development Award and a VA Career Development Award to Dr. L.M.F. (CDA 015-060). Dr. C.I.V. was supported by a VA Career Scientist Award (RCS 14-443). The views represented in this article represent those of the authors and not those of the VA or the U.S. Government.
Disclosure Statement
No competing financial interests exist.