
Abstract
Abstract
Background:
Every laparoscopic procedure starts with the creation of a pneumoperitoneum. The open trocar introduction and the use of a Veress needle (VN) are the two most frequent techniques used. The aim of this study was to evaluate safety of the techniques used to create pneumoperitoneum in laparoscopic abdominal surgery by Belgian minimally invasive surgeons.
Materials and Methods:
This is a prospective study including all consecutive patients undergoing a laparoscopic surgical procedure for a 2-month period. Primary endpoint was access-related problems during creation of a pneumoperitoneum. Access-related problems were registered using a special smartphone application, facilitating data recording and patient registration.
Results:
Overall, 9 out of 212 invited surgeons (4.2%) actively registered patients during the study period. A total number of 342 patients were included with 6 access-related problems (1.8%) and conversion to open surgery was necessary in 16 patients (4.7%). Most reported access-related problem was failure to establish a pneumoperitoneum secondary to insufflation of the omentum. There were no major access-related complications. There was no conversion in the group of patients who had an access-related problem.
Conclusion:
VN entry to create a pneumoperitoneum is safe. In a short study period, gathering data by surgeons willing to participate in a snapshot study is easy and facilitated by a web-based application.
Introduction
Minimally invasive surgery has become the method of choice for treating most abdominal diseases that require surgery, and laparoscopic surgery is still gaining acceptance in intra-abdominal surgery. Creation of a working space by means of a pneumoperitoneum1,2 is the first and also one of the most critical steps because of the risk of injury to intra-abdominal and/or retroperitoneal structures. Although laparoscopic surgery is common practice nowadays, it is estimated that >50% of all complications are related to the initial trocar insertion.3,4
There are several ways to create pneumoperitoneum and to start a laparoscopic procedure: closed and open techniques. There is, however, no consensus regarding the optimal method of gaining access and to create a pneumoperitoneum. Two most used techniques are open trocar introduction and use of a Veress needle (VN). VN entry involves a spring-loaded needle, which is inserted blindly into the peritoneal cavity, after which the first trocar is also introduced in a blind manner. Moreover, several locations on the abdominal region can be chosen for VN entry and first trocar introduction. Hasson originally described an open entry (OE) technique. It involves cutting the peritoneum, opening the abdominal cavity, and inserting a trocar under direct visualization. 5
Two other methods involve a combination of VN and open introduction, and the use of an optic trocar to introduce the first trocar under guidance of the laparoscope. The aim of this study was to evaluate techniques used to create pneumoperitoneum in laparoscopic abdominal surgery and the safety of the VN entry technique. A Belgian snapshot initiative was started among minimally invasive surgeons to register access-related complications and conversions.
Materials and Methods
All consecutive patients undergoing a laparoscopic procedure were included in this prospective Belgian study over a 2-month period. From October 1 to November 30, 2017, all members of the Belgian Group for Endoscopic Surgery were invited to voluntarily join the study and register all patients undergoing laparoscopic surgery during this period. All adult patients undergoing primary laparoscopic surgery, for any pathology, at a participating hospital during the study period were eligible for inclusion. Patients who had open surgical procedure or nonabdominal surgery were excluded. This study was centrally approved by the medical ethical committee.
The following data were collected.
Identification of the surgeon.
Patient demographics, such as gender, age, and body mass index (BMI), were collected. Surgeons were able to either input exact BMI (kg/m2) or classify patients in a BMI category (<20, 21–25, 26–30, 31–35, 36–40, 41–45, >45 kg/m2).
Indication for surgery and surgical procedure was collected. Pathology of the affected organ was registered, along with type of operation. Only patients with primary surgery were included.
Type of access and insufflation of the abdomen were collected. Modalities of creating a pneumoperitoneum were registered. Surgeons could choose one of the following options: VN closed, VN open, optic trocar, and open introduction. A “closed Veress needle” was defined as creation of a pneumoperitoneum with a VN and introduction of the first trocar without opening the peritoneum in a sharp or blunt manner. An “open Veress needle” was defined as creation of a pneumoperitoneum with a VN and introduction of the first trocar after opening the peritoneum. When the first trocar was placed with the help of a camera, the surgeon could select “optic trocar” as type of access. When the trocar was placed first by an open introduction into the abdomen and insufflation was started afterward, “open introduction” could be selected, which is equivalent to the OE technique.
Location of the VN was determined. Abdominal regions could be selected where the VN was placed.
Location of the first trocar was determined. Five major regions could be selected: left and right subcostal regions, umbilical, midline, and flank.
Access-related problems and conversion were determined. Access-related problems were defined as any problem that occurred during creation of a pneumoperitoneum and insertion of the first trocar. Surgeons could indicate the nature of the problem. Conversion was defined as changing surgical approach from laparoscopy to open surgery.
To collect all data in a minimum amount of time, a special and novel smartphone application was developed. This application could be downloaded on surgeon's smartphone facilitating registration of patient data after each operation. After each laparoscopic procedure, the surgeon could enter patient's data. An online platform Meplis* was used for data registration. Postoperative follow-up data were not required, so all patients should be entered immediately after the operation and data collection should, therefore, be completed by December 1, 2017. No change in normal patient management was required. After closure date of the study, data were downloaded from the platform to an Excel sheet and all analyses were performed using SAS® software, version 9.4 of the SAS System for Windows (Microsoft, Inc.).
Results
Overall, 9 out of 212 invited surgeons (4.2%) actively registered patients during the study period (Fig. 1). A total of 342 patients were included: 170 female patients (49.7%) and 172 male patients (50.3%) with a median age of 55.5 (interquartile range 39–70) years. The majority of patients (38%) had a BMI between 21 and 25 kg/m2 (<20: 5.9%, 26–30: 29.2%, 31–35: 12.6%, 36–40: 7.9%, 41–45: 4.9%, >45: 1.5%). Most patients underwent one surgical procedure, but 12 patients (3.5%) underwent two separate operations with the same approach during the same anesthesia. The majority of patients (25%) had symptomatic gallstone disease and underwent laparoscopic cholecystectomy (Fig. 2). Access to the peritoneal cavity was created by the closed VN method in 281 patients (82.2%). Open trocar insertion was performed in 7.9% of patients, open trocar insertion after insufflation of the abdomen with a VN (Veress-open method) was performed in 2.3% of patients, and in 7.6% of patients an optic trocar was used to create a pneumoperitoneum. If a VN was used, left Palmer's point was the location of choice in 74% of patients, umbilical access in 24% of patients, and right Palmer's point in 2% of patients. First trocars were mostly placed at the umbilicus (64%) or left hypochondrium (18.4%). There was no conversion in the group of patients who had an access-related problem. All access-related problems occurred when VN entry was done at left Palmer's point. The majority of VN insertion problems were failures to establish a pneumoperitoneum with low-flow CO2 insufflation due to insufflation of the omentum (4 out of 6 cases). In 2 cases, the gastric wall was punctured in a nonfull thickness manner, leading to VN replacement. In 1 case pneumo-omentum occurred with minor bleeding (Table 1). There were no major access-related complications.

Flowchart of participating minimally invasive surgeons from the Belgian Group for Endoscopic Surgery.
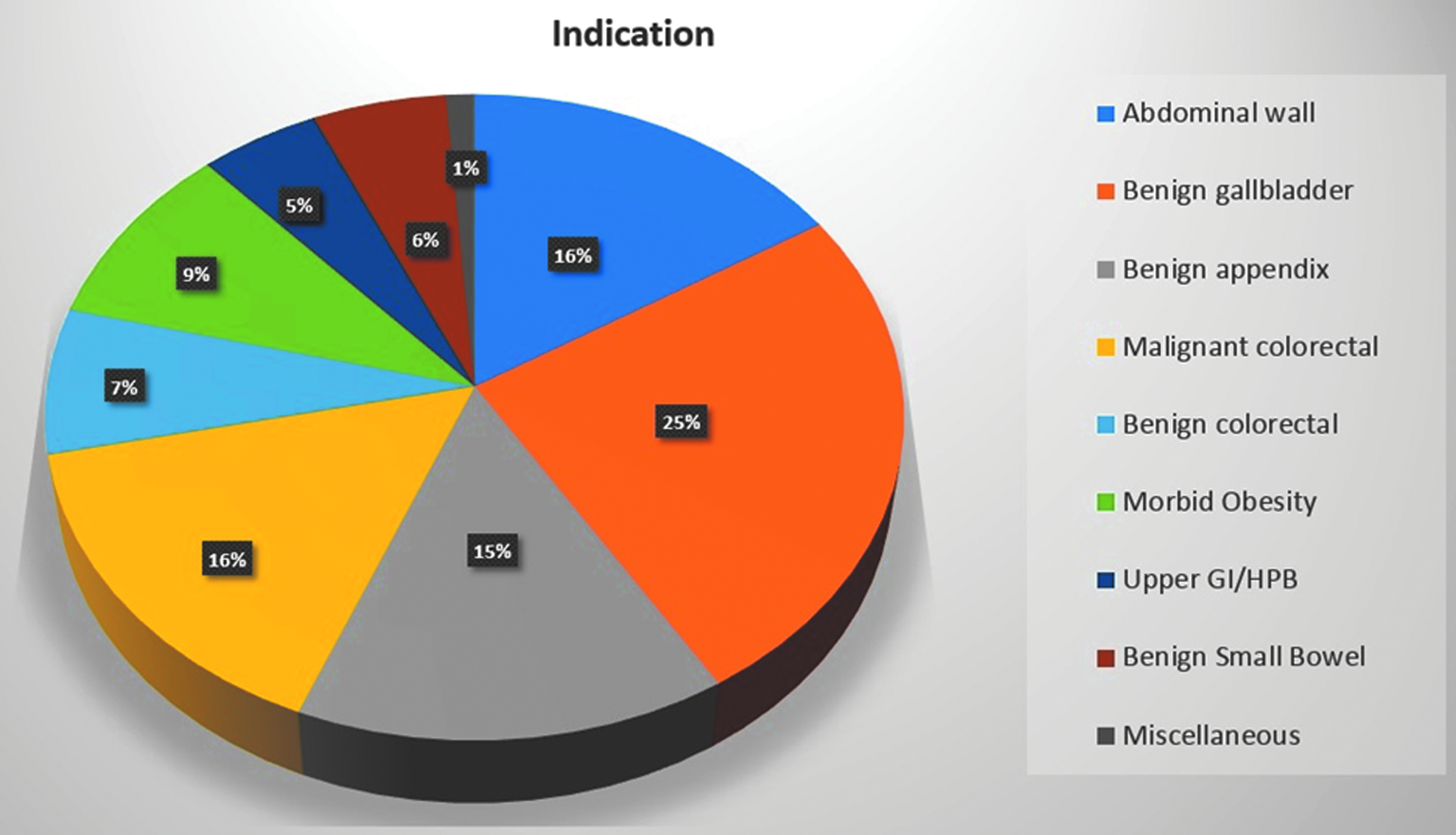
Circular histogram of indication for surgery.
Access-Related Problems and Conversions for Different Approaches
NA, not applicable.
Discussion
Götze designed a needle to create an “automatic” pneumoperitoneum in 1918, 6 but the widely used spring-loaded needle was created by Janos Veress in 1938. 7 Nowadays, creation of a pneumoperitoneum by VN entry is the most commonly used approach,8,9 and it can be placed at practically any site.2,9,10 The present snapshot study showed that access-related problems during general laparoscopic surgery were 1.8%. Considering VN entry only, incidence of access-related problems was 2.1%. Moreover, conversion to open surgery was <5% in this cohort.
Peritoneal entry and initial trocar insertion have been studied in several systematic reviews and meta-analysis.11–13 Safety and feasibility of different options have been shown, but robust conclusions regarding which approach is best could not be drawn. Recent update of a systematic Cochrane review regarding laparoscopic entry techniques concluded that there was insufficient evidence to support the use of one technique over another. Evidence was of low quality, because of small sample sizes and very low event rates. Moreover, there was risk of bias associated with poor reporting of study methods. 11 Several options exist to create a pneumoperitoneum, namely VN entry at the umbilical site and the open Hasson technique.8,11 Alternatively, VN entry can be performed at left Palmer's point, 14 which was also the preferred method in this study. Advantages of this approach are lower risk for major vascular damage and bowel injury, by avoiding the midline and previous scars, feasible blind insertion, and the fact that VN remains in situ when the first trocar is placed allowing optimal constant insufflation. Potential problems are puncture of the stomach wall and left liver lobe and puncture or insufflation of the omentum. In all entry methods, major complications—defined as major vessel injury, gastrointestinal injury, and solid organ injury—were extremely rare. Minor complications, mostly involving trocar site bleeding, were fewer in direct trocar entry, VN entry, and open introduction, respectively. However, it has been shown that omental injury is more frequent in VN entry with incidences reported between 2.9% and 6.4%.13,15 As observed in this study, minor omental injury was the main reason for access-related problems after VN insertion. Overall, injuries caused by VN entry described in the literature are estimated to be as low as 0.23%. 12 Incidence of major injuries is 3.7%, with mainly vascular injuries. This could well be an under-reported number, because many studies included were retrospective in nature, leading to inherent bias. As such, it could be considered a strength of this study, because all patients were included in a prospective way immediately after the operation through a web-based application. Ease and immediate access to the platform contributed to facilitation of patient registration by operating surgeons. Apart from low reported incidences of access-related problems and conversions, this study also shows that surgeons in Belgium are not inclined to participate in a fairly easy study to perform. Response rate was only 4.2%, which is one of the limitations of the study. Another limitation is the lack of clinical follow-up. Moreover, different access groups were too small to compare and to draw meaningful conclusions. In contrast, 9 surgeons registered 342 patients in a timeframe of 2 months, meaning an average of 38 patients per surgeon. If surgeons are willing to be part of a snapshot study, a huge volume of data can be gathered in a limited amount of time, with minimal extra workload for the participating surgeon. It again shows the enormous potential and power of a snapshot study. 16
Footnotes
Acknowledgments
The author wishes to acknowledge the Belgian Group for Endoscopic Surgery-snapshot collaborators: Dr. B. Monami, Dr. K. Demey, Dr. B. Majerus, Dr. V. Drubbel, Dr. M. Vandemoortel, Dr. C. de Gheldere, Dr. B. Smet, and Dr. J. L. Jourdan.
Disclosure Statement
No competing financial interests exist.