
Abstract
Every field of surgery has seen an explosion of new technologies aimed at improving surgical technique and reducing complications. The use of near-infrared (NIR) fluorescence to assess perfusion has been described in several surgical disciplines. NIR provides the surgeon with real-time perfusion assessment of a target organ or anastomosis and can be invaluable in aiding decision-making during the index operation. In the following article we discuss the use of fluorescence-guided perfusion assessment during colonic interposition for esophageal replacement. To our knowledge this is the first description of the use of fluorescence-guided perfusion assessment during colonic interposition.
Introduction
Surgical resection of the esophagus is the cornerstone of a wide range of esophageal pathologies such as end-stage achalasia, esophageal cancer, and corrosive injury to the esophagus. The primary pathology and the extent of resection dictates the need for replacement of the esophagus with an enteric conduit.
The stomach has been the preferred conduit for esophageal replacement given its robust blood supply, the ability to reach the neck and upper chest to perform a tension-free anastomosis, and finally its ability to adapt and take on the role of both reservoir and conduit.
Alternative conduits might be required when the stomach has been injured or absent. Although both the small and large bowels might play a role as conduits for upper alimentary tract continuity, it is widely accepted that the colon is the preferred conduit for use in case the stomach is not feasible for esophageal replacement. 1
Despite significant improvements in surgical technique, perioperative care, and technology, anastomotic leak remains the major cause of increased morbidity and mortality following esophagectomy. Patients undergoing colonic interposition are particularly at risk of this complication with some authors noting a leak rate of up to 30%. Anastomotic leaks can be due to patient-related factors, surgery-related factors, and simply by an increased number of anastomoses. Multiple interventions have been developed over the years to reduce the rate of anastomotic leak following colonic interposition with the common goal being to avoid anastomotic ischemia and conduit necrosis.2–4
The increased use of near-infrared (NIR) fluorescence imaging in surgery in the last decade infiltrated into multiple surgical subspecialties. While NIR was used mainly for plastic surgery early on, it has seen a rapid adoption in colorectal anastomotic assessment and more recently for the assessment of gastric conduit in foregut surgery. Other utilization such as sentinel lymph node mapping and intraoperative solid and metastatic tumor identification are being investigated.5,6 In addition to anastomotic perfusion issues, colonic interposition carries an added layer of complexity to the perfusion story, besides the necessity to confirm adequate anastomotic perfusion as the surgeon is faced with the need to make a decision regarding which segment of colon is optimal for use.
Our group has been using NIR fluorescence imaging in multiple surgeries for perfusion assessment and solid tumor identification. Utilizing our previous experience, we started looking at leveraging this technology for cases of colonic interposition. While decisions regarding the ideal segment of colon were made either arbitrarily or subjectively in the past, we found that the use of NIR fluorescence imaging provided objective, actionable evidence in real time and helped us in making informed intraoperative decisions. It is also a dynamic technology that can be repeated at each step of the operation for the assessment of a reliable vascular pedicle and for choosing an appropriate conduit before resection. It is also useful in the confirmation of an adequate perfusion before and following the creation of each anastomosis during colonic interposition.
In this article we describe our preferred technique for using intraoperative NIR for anastomotic perfusion assessment and decision-making during colonic interposition.
This method can be applied for other indications where colonic interposition is used for esophageal replacement.
Preoperative and Intraoperative Management
Esophageal surgery is regarded as a highly morbid surgical procedure. Patients are usually sick, malnourished, and have multiple comorbidities. While accidental ingestion of caustic material is more common in children, intentional ingestion as part of a suicide attempt is the leading cause of caustic esophageal injury in adults.
Lye ingestion promotes extensive inflammation and liquefactive necrosis of the esophagus and stomach. This allows the caustic agent to penetrate the esophageal wall more deeply, thereby escalating the severity of the injury. The exposure causes injuries ranging in severity from first-, second-, and third-degree burn to full-thickness necrosis and frank perforation. 7
Following an acute ingestion, patients are either observed or undergo a salvage procedure based on the extent of the injury and clinical picture. Esophageal strictures are the most common sequela of second- to third-degree esophageal burn. Most of these strictures frequently start to develop 3–4 weeks following ingestion, and peak after 2 months. Many strictures will respond to serial dilatation. Refractive caustic strictures require elective esophagectomy with reconstruction. 8
Before surgery, it is advisable to assess the patient's physiologic reserve. Cardiopulmonary assessment should be done to identify patients with limited cardiac output that might affect circulation and might cause limited vascular end-organ perfusion, thereby increasing the risk for anastomotic complications. Colonoscopy and intravenous contrast enhanced computed tomography should be performed preoperatively on all patients to assess the colon for pathology and delineate the vascular supply, respectively. Right colic, left colic, and marginal arteries should be assessed. A marginal artery may be absent or inadequate in 5% of the patients. Special attention should be paid to the status of the inferior mesenteric artery especially in older patients with atherosclerosis. Patients should be placed on liquid diet and given a mechanical bowel preparation 24–48 hours before the operation. Broad-spectrum antibiotics and subcutaneous heparin are given before the procedure.
During surgery, blood volume should be maintained meticulously by both the surgical team and by anesthesia. Bear in mind that 75% of peripheral resistance that modulates peripheral blood pressure occurs in the splanchnic vascular bed. Considerable splanchnic vasoconstriction can occur as a result of changes in blood volume, and this might be reflected by monitored parameters. Splanchnic vasoconstriction can reduce colonic graft perfusion that might result in ischemia and/or reperfusion injury.
In the following section, we describe in details our method for perfusion assessment, which may be readily applied during colonic interposition.
Perfusion Assessment for Appropriate Colonic Conduit
The importance of a reliable blood supply to the conduit cannot be overemphasized.
Both our and others' experience indicates that the preferable graft is the left colon based on the ascending branch of the left colic artery as a vascular pedicle with ligation of the middle colic pedicle proximally to allow enough length and to maintain patency between the right and left branches, which ensures blood flow to the proximal aspect of the graft. This has been shown to decrease the rate of graft ischemia.9–12
If preoperative CT angiography revealed significant arteriosclerotic changes involving the origin and initial portion of the inferior mesenteric artery, or if the patient underwent previous colectomy or has significant diverticular disease as demonstrated in the preoperative colonoscopy, the left-sided colonic graft should not be used, and the right colon can be used, provided it is of adequate length. Oftentimes, the right colon cannot reach to the neck and a high intrathoracic anastomosis is required.13–15
Surgical Technique
Stages
Colon preparation and resection Esophagocolonic anastomoses Cologastric or colojejunal anastomosis Colocolonic anastomosis
The colon is usually prepared through a midline laparotomy. A complete colonic mobilization starts with dissection of the omentum off the transverse colon followed by mobilization of the ascending and descending colon as well as both hepatic and splenic flexures. The whole colon is mobilized to the midline, making sure the mesentery is free of tension (Fig. 1). Stretching out the colon with its mesentery cephalad allows transmesenteric illumination, which helps in the visualization of the vascular supply of the colon. The ascending branch of the left colic artery can be easily identified as it forms a natural pedicle ascending in the direction of the splenic flexure and joining, in a majority of cases, the marginal artery of Drummond. The middle colic arcade with its right and left branches should be identified as well.
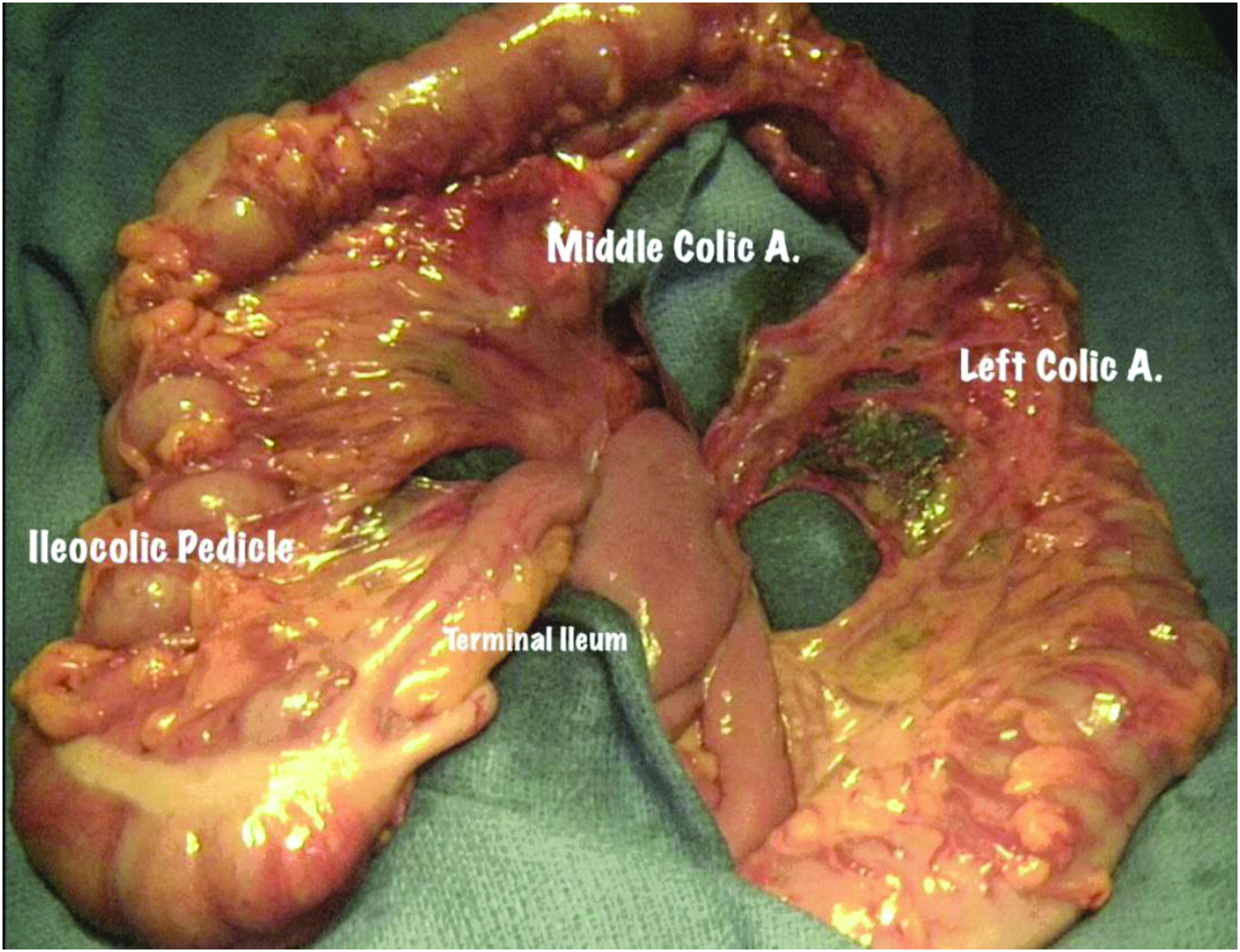
Dissected colon demonstrating the ileocolic, middle colic, and left colic vascular pedicles.
Next, the length of the colon graft should be assessed by pulling the left colon as much as possible in a cephalad direction on the natural pedicle of the left colic artery. This point is usually at the level of the xiphoid and is marking the distal anastomotic site (marked with a stitch). The distance between the xyphoid and the angle of left jaw is measured liberally with an umbilical tape. The same distance is measured from the previously marked distal point using the umbilical tape and should be marked with a second marking stitch. This corresponds to the future esophageal anastomotic site and is usually to the right of the right branch of the middle colic artery. 9
Before ligation and division of any vessel, attention is turned to perfusion assessment. We recommend occluding each of the vessels slated for transection with a small non-crushing bulldog clamp and checking the adequacy of blood flow to the proximal end of the graft. This is most readily accomplished with an NIR perfusion assessment.
The anesthesiologist injects 5 mL of 2.5 mg/mL indocyanine green (ICG).16,17 We checked perfusion using the PINPOINT© Endoscopic Fluorescence Imaging System (Novadaq) (Supplementary Data). It is imperative to make sure the patient's hemodynamics are optimized and no vasopressors are being used before perfusion assessment. Perfusion is assessed by evaluating the immediate flow and the presence of perfusion (quantified by rapid, slow, or absent perfusion). Demarcation of perfusion should be marked and compared with the previously proximal and distal marking stitches. If needed, injection of ICG can be repeated to assess perfusion again as ICG is well excreted and not reabsorbed (Fig. 2).
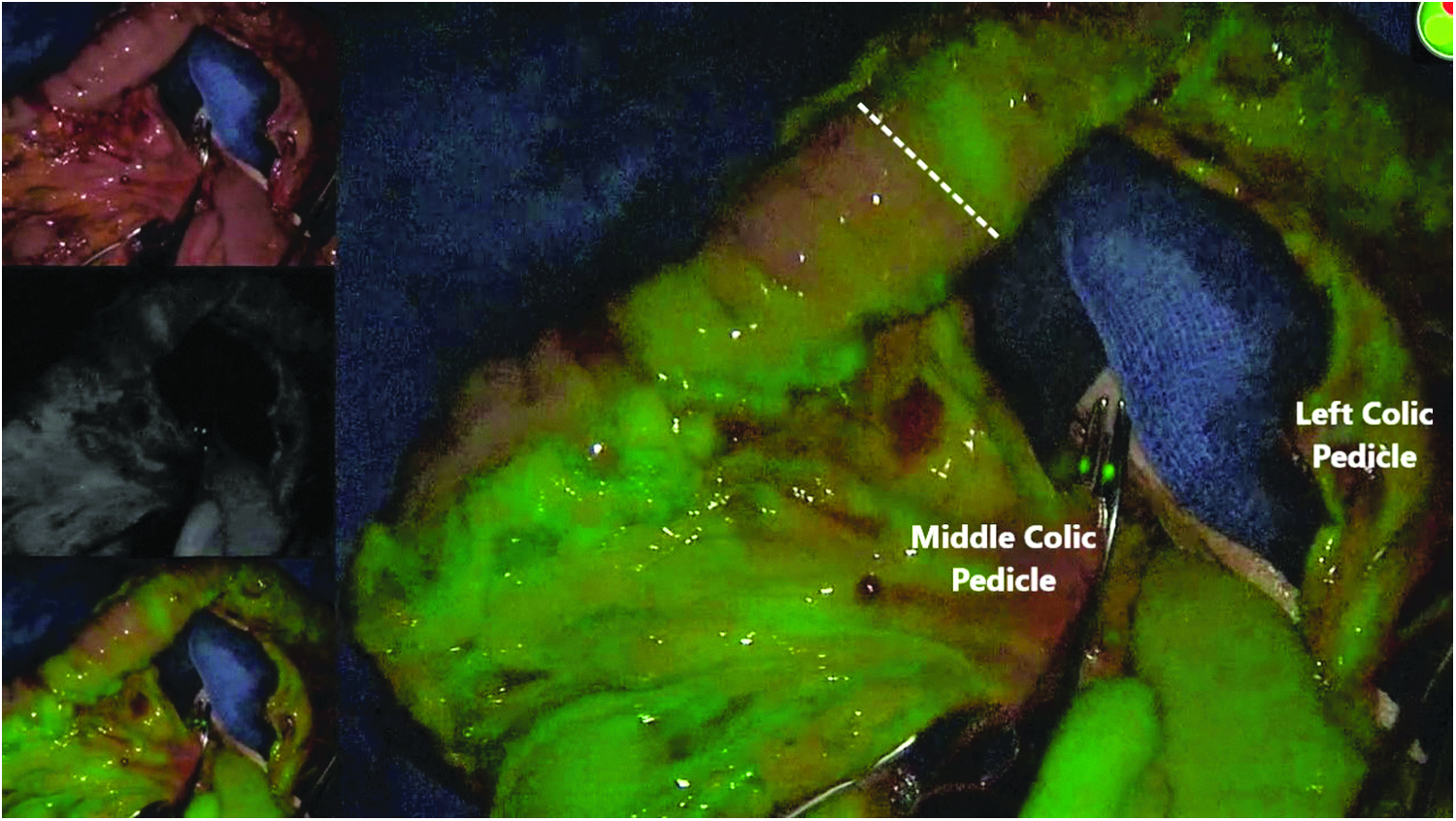
Middle colic pedicle with a bulldog clamp demonstrating the demarcation zone (dashed line) for future resection.
If perfusion appears to be adequate, the vessels may be divided at the stem of the middle colic vessels to allow optimal flow. Colon resection should be postponed until later in the operation for a better demarcation of transection borders (Fig 3).

Old scar at colocutaneous fistula site at the splenic flexure illustrating a lack of adequate perfusion, which prohibits the use of left colon as a conduit.
Simultaneously, we turn to perform cervical dissection and mobilization of the esophagus in preparation for proximal anastomosis. We found that a “two team” approach (one performs laparotomy and colon preparation, while the other exposes and mobilizes the esophagus) significantly decreased operative time.
The left neck approach is preferred. If the substernal route is chosen, the left half of the proximal manubrium together with the medial end of the first rib and the sternal head of the left clavicle are resected to enlarge the thoracic inlet. (Attention should be paid not to injure the left internal mammary artery in case a future free jejunal flap will be needed in case of colonic graft failure.9,15)
Caustic injuries deserve special consideration regarding the proximal and distal extent of injury and resection.
If the cervical esophagus is destroyed, anastomosis can be made to the lateral hypopharynx through an anterior suprahyoid approach. If the scarring extends to the hypopharynx, extensive pharyngoplasty is required, which we usually performed with the help of an otolaryngologist as resection of the hyoid bone as well as the thyroid cartilage is necessary. (Laryngectomy may be needed with the formation of permanent tracheostomy. 18 ) If no proximal scarring or narrowing is found, anastomosis should be done to a well-perfused, viable esophagus. As for the distal extent of injury, if part of the stomach is viable, we prefer to preserve the stomach and perform proximal gastrectomy with cologastric anastomosis to the posterior surface of the stomach. If the stomach is injured from caustic ingestion as well, we proceed with total gastrectomy and perform a Roux-en-Y colojejunostomy. If substernal esophageal bypass is planned, the distal esophagus should be stapled off with closure of the hiatus with sutures to avoid future abdominal viscera herniation. 12
Perfusion Assessment After Creation of Anastomoses
After preparation of the neck (and the substernal space if planning to use this space), we turn our attention to perfusion assessment of all potential anastomotic margins.
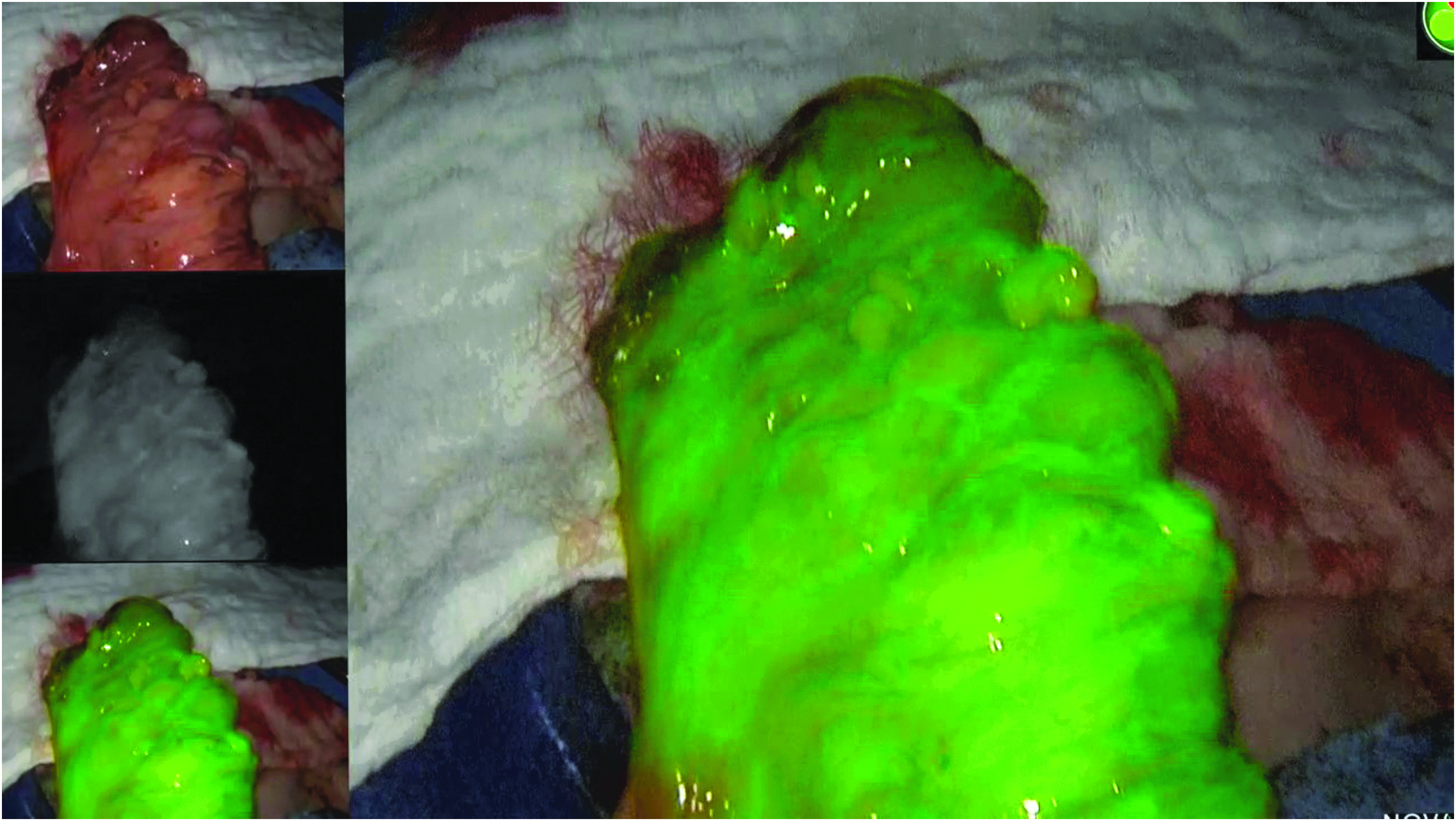
We start by injecting an additional bolus of ICG to make sure there is no change in the perfusion of planned colonic resection sites. We then perform resection of the colon according to the demarcation zones. Following resection, the future conduit is laid on the anterior chest wall to assess that it has an adequate length. Great care must be taken to ensure that the mesentery is not twisted and that the proximal and distal ends are well perfused following an ICG injection (Fig. 4). The colon is brought up to the left neck substernally with the help of a protecting bag, and perfusion is assessed again using an ICG injection before the creation of esophagocolonic anastomosis (Figs. 5, 6).

Left colic pedicle and perfused colon placed on the anterior chest wall showing adequate perfusion before placement at the substernal space.
Robust perfusion of the proximal colon at the level of the left neck before creation of esophagocolonic anastomosis.
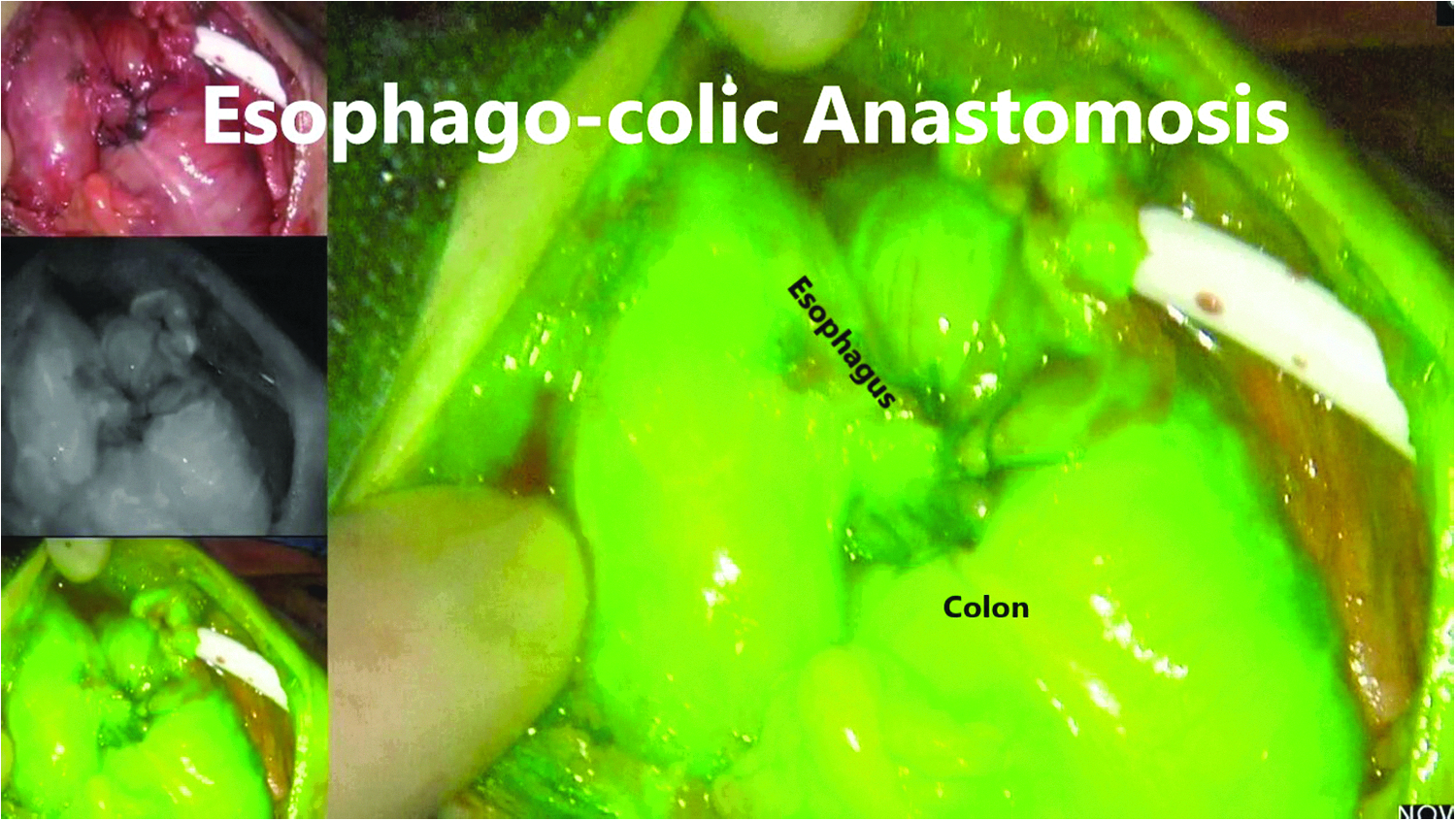
Adequate perfusion following the creation of esophagocolonic anastomosis.
The distal end of the colonic graft is anastomosed either to the stomach (if viable stomach exists) or to the small bowel using a Roux-en-Y configuration. ICG perfusion assessment is again utilized before these anastomoses as well.
Colonic continuity is re-established by bringing the previously mobilized right colon over to the distal end of the divided colon graft (Fig. 7). The right colon mesentery and the descending and sigmoid colon mesentery are not divided to preserve as much arterial perfusion and venous drainage. Additional boluses of ICG injection can confirm adequate perfusion before and subsequent to this final anastomosis.

Adequate perfusion following the creation of colocolonic anastomosis.
Feeding jejunostomy tube is placed at the end of the case.
Decision-Making Based on ICG Perfusion
Anastomotic leak is regarded one of the most devastating complications following colonic interposition. With more than one anastomosis, the risk is increased several folds.
Intraoperative perfusion assessment using ICG can help with decision-making in real time.
Since ICG is retained in the intravascular compartment and is rapidly taken up and excreted by the liver in the bile, multiple repeated injections can be carried out without interference from previous administrations. ICG is also very well tolerated and has a very favorable safety profile. 19
During the resection phase of the operation, repeated ICG injections can help to choose between the right and left colon as an appropriate conduit. Using non-crushing bulldog clamps on the planed transected vessels, ICG perfusion assessment can assist in defining the demarcation zone (Fig. 2). During the reconstruction phase, repeated ICG injections can provide a margin of safety in selecting the optimal site for anastomosis in case there are questionable areas.
If perfusion is insufficient at this stage, the surgeon still maintains the option to convert the anastomosis to a lower site on the conduit. Furthermore, if the conduit is totally inappropriate, the possibility of supercharging the anastomosis can be discussed and still employed.
Following the reconstruction, repeated evaluations of anastomoses may show insufficient perfusion. If patient hemodynamics are optimized (it is highly important to avoid vasopressors at this stage), a redo anastomosis or a supercharged anastomosis can be considered.
Discussion
Although multiple conduit options exist for esophageal replacement, colon interposition is the preferred conduit in cases of an injured stomach.
Given the number of anastomoses and the overall condition of the patient who is being referred to such an extensive surgery, the morbidity and mortality has not changed significantly over the years in spite of improvement in surgical techniques and perioperative care. Several studies have identified the risk factors for anastomotic leakage. 20 These multiple risk factors compromise perfusion of the conduit and thereby promote leak. With this in mind, perfusion assessment of anastomotic margins might be a great resource to assess the conduit's ischemia. Furthermore, NIR provides the surgeon with the ability to assess perfusion intraoperatively and then act on this information, thus allowing the surgeon to choose appropriate sites for anastomosis, the proper conduit, identify demarcation zones before resection, and confirm appropriate perfusion before and following the creation of anastomosis. In case of insufficient perfusion, it may help the surgeon to decide in real time and thus avoid deleterious consequences of one or more anastomotic leaks.
NIR in combination with ICG used in real-time perfusion is a relatively new technique based on the light-emitting properties of ICG at the NIR spectrum. Specialized cameras and imaging sources such as the Firefly system (Intuitive Surgical, Sunnyvale, CA) or Pinpoint imaging system (Novadaq) and others are available in the market for NIR perfusion assessment. 19
Their use has been validated in multiple studies both in colorectal surgery and esophageal surgery.
The PILLAR II (Perfusion Assessment in Laparoscopic Left Anterior Resection) trial, a multicenter, nonrandomized study, reported an anastomotic leak rate of 1.4% in 139 patients, which represents a reduction of eightfold from the historical leak rate of 12% following anterior resection. 17 A systematic review by Degett et al. summarizing 10 nonrandomized trials (n = 916) of immunofluorescence in colorectal surgery supports the early data of PILLAR II. The addition of NIR–ICG gave a pooled incidence of leak of 3.83% (95% CI 2.64%–5.02%) in colorectal resection surgery. 16
Masaki et al. studied 120 patients who underwent esophagectomy with esophagogastric reconstruction. One out of 59 patients had anastomotic leak following perfusion assessment with ICG (1.7%) compared with 9/61 (8.4%) patients who had anastomotic leak where anastomotic perfusion was assessed without the use of NIR–ICG. The authors concluded that using ICG fluorescence imaging to evaluate blood flow in the gastric conduit might decrease the incidence of anastomotic leak following esophagectomy for cancer. 21
Conclusion
Our technique for perfusion assessment using NIR–ICG injection in colonic interposition for esophageal replacement is easy, safe, and effective. It has a short learning curve and can be repeated multiple times during surgery. It can evaluate multiple anastomoses during the surgery in real time and has the potential to improve decision-making during resection and reconstruction with the goal of reducing the rate of anastomotic leak.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.