
Abstract
Background:
Posterior sagittal anorectoplasty (PSARP) has been the standard for management of children with high anorectal malformations (ARMs). Recently, there has been an increase in the use of laparoscopy in its management. We analyzed the outcomes of laparoscopically assisted anorectal pull-through (LAARP) compared to PSARP using a large inpatient database.
Methods:
Kids' Inpatient Database was analyzed for ARM (ICD-9-CM 751.2) between 1997 and 2012. Perineal fistulas and low/intermediate ARM were excluded. Propensity score (PS)-matched analyses were performed using 37 variables. Cases were weighted to provide national estimates.
Results:
Of the overall 29,106 cases, 7428 patients <2 years underwent surgical repair. LAARP was performed in 178 patients. Eighty-eight percent were male. Most were of Caucasian (n = 71; 45%), followed by Hispanic (n = 41; 26%) descent. Most were performed in 2009 and 2012 (n = 149; 83%). Most were covered by Medicaid (88; 49%), followed by private insurance (80; 45%). Median length of stay (LOS) was 4 (interquartile range = 3) days. The majority were performed in a children's hospital (n = 90; 88%). On PS-matched analysis, LAARP had shorter median LOS (4 [3]) compared to PSARP (6 [15]) days, P = .003. Rates of reoperation, wound infection, wound dehiscence, and mortality were unchanged between approaches. Cost was lower for LAARP (47,969 [49,450]) versus PSARP (56,110 [160,314]) U.S. dollar , P = .002, whereas total charges did not differ significantly.
Conclusions:
A minimal access approach to a complex procedure requires significant time and resources to be adopted as standard. PSARP is an important example, as increased availability of laparoscopy, and therefore, access to the procedure for patients will greatly affect resource utilization and recovery for the patient. As demonstrated, the LOS and cost is significantly lower for the LAARP procedure in comparison to the traditional approach. Future research will clarify boundaries to introducing the laparoscopic approach as a potential standard technique in the next decade.
Introduction
Anorectal malformations (ARM
Surgical repair of high ARM involves dissection and mobilization of the distal rectum, ligation of the fistula, and accurate placement within the sphincter mechanism.4,5 In 1982, deVries and Pena developed the posterior sagittal anorectoplasty (PSARP), which is an open procedure that achieves these goals. 6 As minimal access surgery became more prevalent for a variety of indications in pediatric surgery, the laparoscopically assisted anorectal pull-through (LAARP) was developed by Georgeson et al. 7 LAARP has increased in popularity over the near-two decade experience, and several analyses have attempted to compare outcomes against the traditional PSARP procedure.1,2,5,8–12 Overall, no one approach has been demonstrated to be superior in the current literature with regard to outcomes, in part, due to the lack of standardized analyses with sufficient subjects in either treatment group.1,2
In this large, population-based analysis, we aimed to compare the outcomes of LAARP and PSARP, particularly as it pertains to resource utilization. This analysis represents the largest comparison of outcomes between LAARP and PSARP, particularly with regard to resource utilization. We believe that this information will be useful especially as LAARP becomes a more commonly performed procedure.
Materials and Methods
The Kids' Inpatient Database (KID) is a population-based sample of pediatric inpatient discharges within the United States. The dataset is managed by the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality. Each of the triennial releases, available between 1997 and 2012, contains ∼7 million weighted cases. Diagnosis and procedure codes are designated according to the International Classification of Diseases, ninth revision, Clinical Modification (ICD-9-CM).
For this analysis, we identified cases of ARM with ICD-9-CM diagnosis code 751.2. We limited the analyses to cases of children younger than 2 years of age, as this analysis sought to perform a comparison between the open and laparoscopic approach in the initial surgical procedure for imperforate anus. As low or intermediate imperforate anus may be repaired via a perineal approach, we isolated cases of high imperforate anus—those necessitating an abdominal approach for surgical repair—by using associated diagnosis and procedure codes. Codes indicating the presence or creation of colostomy and fistulas to the bladder or urinary tract were used in favor of high imperforate anus (including 596.1, 619.1), while others, such as perineal fistula repair (71.72), were used to exclude cases likely to have had low imperforate anus. After an initial screening process based on diagnosis and procedure codes, we performed a manual review to exclude cases with a low likelihood of high imperforate anus. Open and laparoscopic approaches were classified according to procedure codes, including 48.43 and 48.40 compared to 48.42, respectively.
Categorical variables were compared using chi-square or Fisher exact tests as appropriate. Continuous variables were compared using t or Mann–Whitney U tests as appropriate and are presented as median and interquartile range. Cost values were calculated using cost-to-charge ratio files, which are available for years 2003, 2006, 2009, and 2012 from the HCUP. Analyses involving cost and charges were adjusted to 2012 U.S. dollar values according to rates determined by the U.S. Department of Labor. 13
Propensity score (PS)-matched analyses of LAARP versus PSARP were performed using a 1:1 nearest neighbor matching method. Datasets containing a total of 66 variables were compared using 37 covariates for risk-adjustment. PSs were matched using multivariate logistic regression, on the basis of demographic, socioeconomic, hospital characteristics, and common comorbidities validated as the Elixhauser method. 14 Matched datasets were then pooled for a 1:1 fixed ratio study cohort.
PS value assignment, case sorting, and matching were performed using MatchIt version 2.4-20 (Cambridge, MA), a supplemental module available for R, version 2.14.2 (R foundation for Statistical Computing, Vienna, Austria). 15 All statistical analyses were performed using SPSS Statistics, version 21.0 (IBM; Armonk, NY). The Institutional Review Board at the University of Miami Miller School of Medicine deemed this retrospective study to be exempt from full review.
Results
A total of 29,106 weighted cases were identified during the study period. Approximately 26% of these cases underwent surgical repair, n = 7,428. Among these surgical cases, 178 (2.4%) were performed with a laparoscopic approach, whereas 7250 (97.6%) were performed with an open approach. The total number of cases per year was relatively stable, beginning with 1136 (1997), 1270 (2000), 1305 (2003), 1299 (2006), 1205 (2009), and 1213 cases (2012). During this time, a significant increase in the number of laparoscopic cases was observed (Fig. 1).
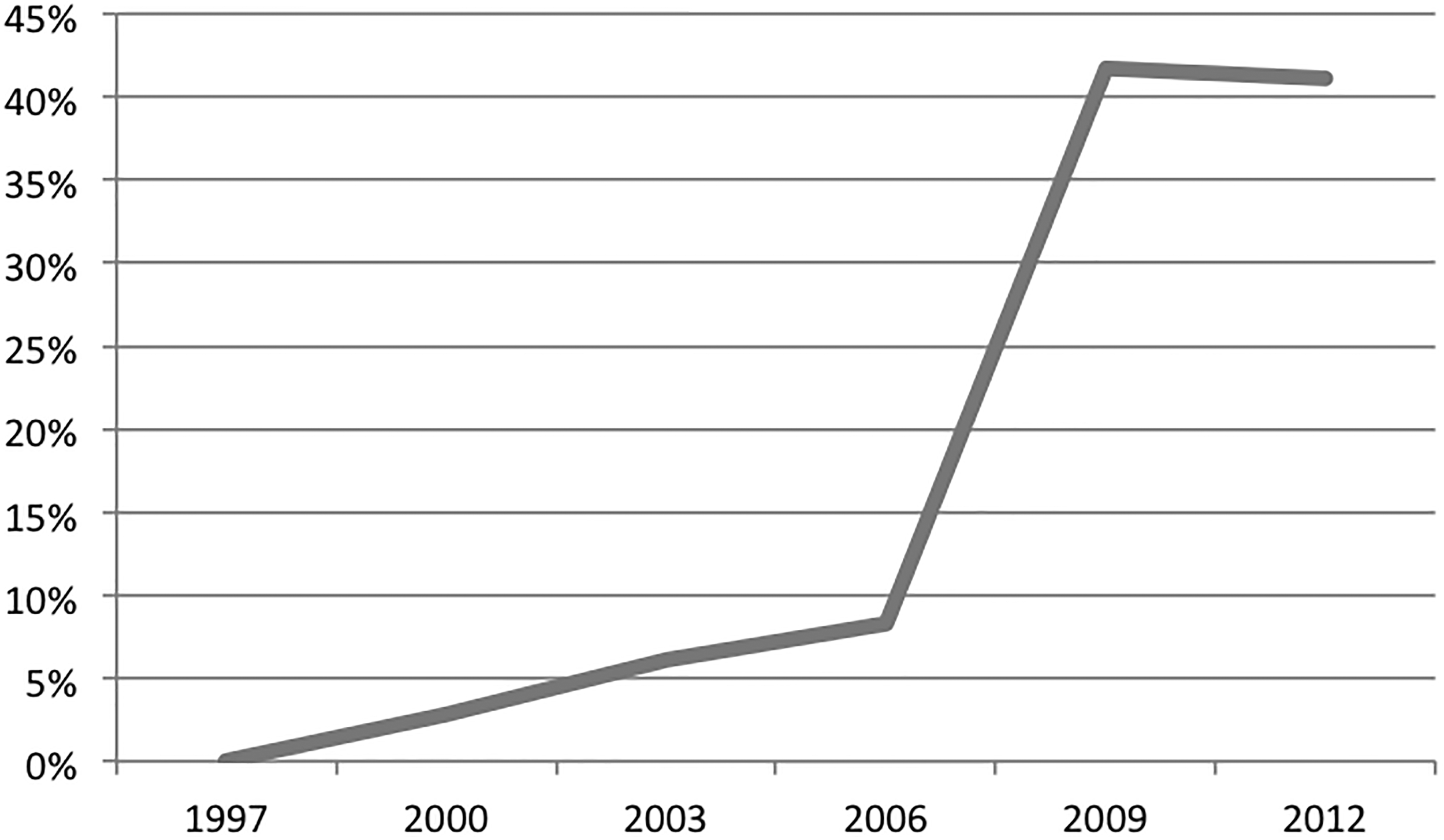
Distribution of laparoscopic pull-through cases for cases of high imperforate anus during study period, 1997–2012. Kids' Inpatient Database. Percentages are displayed to maintain compliance with the Healthcare Cost and Utilization Project Data Use Agreement.
Upon examining the demographic, socioeconomic, and hospital characteristic distribution at baseline between LAARP and PSARP, we found that boys underwent LAARP at a higher rate than girls, P < .001. LAARP was more frequently performed at children's hospitals compared with nonchildren's hospitals, P = .039. Race and payer status distributions were not significantly different. For a tabular representation, see Table 1. There were no significant differences between LAARP and PSARP with regard to resource utilization measures, including length of stay (LOS), total charges, and cost. For a tabular representation, see Table 2.
Comparison of Demographic, Socioeconomic, and Hospital Characteristics
Baseline comparison of demographic, socioeconomic, and hospital characteristics for laparoscopic and open pull-through procedures for cases of high imperforate anus during study period, 1997–2012. Kids' Inpatient Database. Cases limited to available data. Statistical significance set at alpha = 0.05; significant values are bolded.
Comparison of Resource Utilization Measures
Baseline comparison of resource utilization measures for laparoscopic and open pull-through procedures for cases of high imperforate anus during study period, 1997–2012. Kids' Inpatient Database. Cases limited to available data. Statistical significance set at alpha = 0.05; no significant comparisons were found on this analysis.
IQR, interquartile range; USD, U.S. dollar.
A risk-adjusted comparison of LAARP versus PSARP was performed, accounting for demographic, socioeconomic, and hospital characteristics, as well as comorbid conditions. On this 1:1 matched analysis, we found that LAARP (median: 4, interquartile range = 3) had a significantly lower LOS compared to PSARP (6, 15) days, P = .003. Cost of admission was lower for LAARP (47,969, 49,450) as well when compared to PSARP (56,110, 160,314) U.S. dollars, P = .002. Total charges, however, did not differ significantly. Measures, including rates of reoperation, wound infection, wound dehiscence, and mortality, were unchanged between the two approaches. For a tabular representation, see Table 3.
Risk-Adjusted Comparison of Resource Utilization Measures
Risk-adjusted comparison of resource utilization measures for laparoscopic and open pull-through procedures for cases of high imperforate anus during study period, 1997–2012. Kids' Inpatient Database. Cases limited to available data. Reoperation, wound infection/dehiscence, and mortality rates are censored to maintain compliance with the Healthcare Cost and Utilization Project Data Use Agreement. Statistical significance set at alpha = 0.05; significant values are bolded.
IQR, interquartile range; USD, U.S. dollar.
Discussion
In prior literature, LAARP has been demonstrated to have benefits over PSARP. LAARP has lower postoperative complications,1,12 including wound infections and dehiscence,10,12 as well as lower LOS,2,8,12 when compared to PSARP. Due to a more accurate placement of the rectum within the pelvic floor musculature, long-term advantages of LAARP also include more favorable anal manometry findings, 1 such as higher anal canal resting pressure, 8 and lower rates of severe constipation.2,11,12 Other authors found less auspicious conclusions with regard to LAARP, with either higher complication rates 11 or no difference with regard to operative time,2,8 postoperative complications,2,8,9 long-term fecal continence,1,9,10,12 or a Kelly Clinical Score—a comprehensive survey of defecation function.2,8,16 Other analyses remind us, however, that LAARP should not replace PSARP entirely in the setting of intermediate or otherwise complex ARMs. Bischoff et al. described the importance of a combined approach to recto-bladder neck fistulae, which are notoriously difficult to manage with an abdominal approach alone. 5 Our analysis, however, was limited to high ARMs with an abdominal approach, specifically excluding perineal repairs for lower lesions.
Analyses in the current literature are lacking, however, according to recent systematic reviews.1,2,17 On the systematic review of LAARP outcomes compared to PSARP over an 8-year period, Al-Hozaim et al. found that outcomes measured in the current literature are widely variable. A true meta-analysis, while attempted, was precluded due to the lack of uniformity between studies. 1 In its stead, a pooled comparison between the 2 approaches was completed for the study, amounting to a total of 47 patients across 4 studies to develop their conclusions. 1 The authors themselves acknowledged the limitations in achieving truly conclusive results due to the inconsistency of the reported outcome measures. Han et al. performed another systematic review with meta-analyses where possible, where 191 LAARP patients were compared to 169 PSARP patients across 332 articles meeting inclusion criteria. 2 This analysis, however, included both high and intermediate ARMs. Even with such a comprehensive review of the literature, most of the outcome measures were not reported with adequate consistency to be included in a meta-analysis with sufficient statistical power. 2 An additional issue brought forth by Al-Hozaim et al. was the inability to discern whether the comparative studies were truly treating high ARMs, as only 80% of the studies specified accordingly. 1 Overall, the current literature demands that uniform analyses for specific indications be performed to truly compare outcomes between LAARP and PSARP.1,2,4
Our single-study, risk-adjusted comparison of the largest groups of LAARP and PSARP to treat patients with high ARM has found several advantages of the former with regard to resource utilization. Shorter LOS and lower cost were demonstrated after adjusting for confounding variables of demographic, socioeconomic, and hospital characteristics. Overall postoperative complications, as well as specific measures of reoperation, wound infection, wound dehiscence, and mortality, were not changed by the procedure performed. These findings for an advantage in LOS2,8,12 and no difference in postoperative complications2,8,9 are in agreement with multiple prior studies. A benefit with regard to a previously unreported resource utilization measure, cost of hospitalization, is likely associated to the shorter LOS for the minimal access approach. Surprisingly, total charges for the hospitalization were left unchanged. This result may be explained by the variability in the charge calculations for the differing institutions sampled within the KID. In summary, our results support the benefits of LAARP with regard to resource utilization, which maintaining similar results to PSARP with regard to complications following the surgical repair of high ARMs. This strengthens the call for additional resources to be routed toward training surgeons to perform LAARP when possible for this indication.
Our study has several limitations, primarily those that are inherent to the KID. Data within the KID are limited by the predetermined coding scheme, including the ICD-9-CM diagnosis and procedure codes. To purify the dataset, we implemented a series of filtering mechanisms using these codes to identify high ARM accurately and to exclude those with intermediate or low ARMs necessitating a perineal approach. Subsequently, we performed a manual review of the cases within the dataset to ensure data reliability. Another limitation is the sampling error inherent to the data collected by the HCUP. While the KID collects a set of inpatient admissions across the United States, the national estimates provided for analysis rely on the sampling hospitals that are members within the HCUP data system. Finally, our analysis bound by the retrospective nature of the KID, as long-term outcome information, including fecal continence and quality of life, is not available beyond the admission period. Nevertheless, the KID provides significant advantages, specifically for the comparative analysis of resource utilization measures, and has been used as a source for many studies of pediatric surgical outcomes.18–22
Every minimal access alternative to an accepted open procedure takes time to be embraced by the surgical community. As the benefits of a minimal access approach to many surgical indications become apparent, we believe that the repair of ARMs will follow in the same trend. LAARP will likely become the standard of care for high imperforate anus requiring surgical repair, so long as the benefits are objectively demonstrated in the literature. Our large-scale, population-based analysis found that LAARP had the advantages of shorter LOS and lower cost, while other factors were left unchanged. This analysis serves as an initial comparison of outcomes between the minimal access and the traditional approach to a complex surgical problem. As the use of LAARP becomes more widespread, we believe that future studies may be performed to offer additional information on the safety and efficacy of each procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.