
Abstract
Background:
Heller myotomy and laparoscopic fundoplication represents the best treatment option for esophageal achalasia, with effective short- and long-term success. However, treatment options in patients in whom primary surgery failed represent a real challenge. We present the resection of the gastroesophageal junction (GEJ) along with a Roux-en-Y reconstruction as a treatment alternative.
Materials and Methods:
We analyzed the course of 5 patients with achalasia undergoing the resection of the GEJ along with a Roux-en-Y reconstruction for recurrent dysphagia after Heller myotomy and fundoplication, with at least 1 year of follow-up. Symptoms questionnaire and minuted esophagogram before and after treatment were performed in all the patients.
Results:
Five patients underwent resection of the GEJ along with a Roux-en-Y reconstruction. All the patients had dysphagia and 60% had regurgitations. Eighty percent of the patients had more than one previous redo surgery and 100% had had multiple dilations. Preoperative contrast esophagram of 3 patients show Stage II disease (mild and mark dilated esophagus) and 2 patients with Stage III disease (one esophageal curve and severe dilation). Manometry confirmed the diagnosis. At a mean follow-up of 34 months, all the patients reported a marked improvement in dysphagia, with median overall satisfaction rating of 9 (range 7–10), no symptom of gastroesophageal reflux disease (GERD), and good esophageal emptying in the postoperative contrast esophagram.
Conclusions:
The resection of the GEJ and Roux-en-Y reconstruction is an excellent treatment for recurrent dysphagia after Heller myotomy. All the patients reported a marked improvement of their dysphagia. No symptoms of GERD were documented after the surgery. This procedure should be taken into account as an alternative to esophagectomy for recurrent dysphagia.
Introduction
Esophageal achalasia is a rare motility disorder with an incidence of ∼0.5 to 1.6/100,000 inhabitants according to recent reports. It is defined as an esophageal motility disorder characterized by an absence of esophageal peristalsis with impaired (or incomplete) relaxation of the lower esophageal sphincter (LES). 1
The vast majority of cases are of unknown etiology, and different studies have associated them as the underlying cause of an autoimmune, infectious, genetic, neurodegenerative, or hereditary mechanism. The most accepted hypothesis suggests the participation of viral and autoimmune factors that generate an inflammatory cascade and the selective loss or damage of the ganglion cells in the myenteric plexus. 2
The characteristic symptom is dysphagia, which is usually progressive and associated with secondary weight loss. Other symptoms include regurgitation, retrosternal pain associated with swallowing, and respiratory symptoms secondary to aspiration.
Complementary studies should include an upper gastrointestinal series (UGI) that will clarify the esophagogastric anatomy, an upper gastrointestinal endoscopy (UGE) to rule out organic lesion, and an esophageal manometry confirming the esophageal motility disorder diagnosis. 3
Treatment primary objective is directed to improve the symptoms, which is achieved by lowering the functional resistance of the LES and improving esophageal emptying. One must disrupt the muscle fibers of the lower esophagus, the gastroesophageal junction (GEJ), and the first 3 cm of the gastric slope during the surgical procedure called Heller myotomy. This procedure, performed laparoscopically, represents the gold standard for the treatment of esophageal achalasia. The procedure is associated with an antireflux fundoplication to reduce the iatrogenic gastroesophageal reflux created by the myotomy. The overall success rate for the resolution of dysphagia is high (85%–90%).4,5
The small subgroup of patients in whom symptoms of dysphagia recur or persist represent a great therapeutic challenge. In them, the operation is extremely complex. Therefore, treatment options should start with nonoperative approaches, including endoscopic dilations, injection of botulinum toxin, or peroral endoscopic myotomy (POEM).
Given the failure of the endoscopic alternatives, a revisional surgery is advised. Several surgical techniques have been developed for this situation. In our center, we always incline for a laparoscopic redo Heller myotomy. However, in some of these cases, a correct redo Heller myotomy is not technically possible because of the local anatomical situation, fibrosis, or tissue damage in the GEJ.
In these cases, we decided to perform the resection of the GEJ and a Roux-en-Y reconstruction as an alternative to esophagectomy or another type of surgical treatment. This report examines the results of our approach in a short series of patients.
Materials and Methods
We performed a retrospective review of prospectively collected data of patients with a diagnosis of achalasia who underwent surgery in our institution. The inclusion criteria were patients who underwent the resection of the GEJ along with a Roux-en-Y reconstruction for recurrent dysphagia after Heller myotomy and fundoplication, with at least 1 year of follow-up. Preoperative workup included recorded history of surgical or endoscopic procedures for the resolution of achalasia symptoms, a comprehensive questionnaire, UGI, manometry, and endoscopic examination.
Each patient received a questionnaire to assess various aspects of their symptoms and were asked to score the frequency from 0 to 4: 0 = never, 1 = once a month, 2 = once a week, 3 = once a day, and 4 = several times a day, and the severity on a 10-point visual analog scale with 1 being “mild” and 10 as “most severe.”
We classified the radiological findings on UGI using the Resano–Malenchini classification 6 :
Stage I: straight esophagus, narrow channel at the GEJ, visible air level in gastric fundus.
Stage II: dilated esophagus, no esophageal curves, and no air level in the gastric fundus.
Stage III: marked dilation of the esophagus with one curve.
Stage IV: more than one curve, sigmoid esophagus.
Patients were followed at least at 2 weeks, 2 and 6 months, and 1 year postoperative. Symptoms comprehensive questionnaire, UGI, and endoscopic examination were performed in all 5 patients. As preoperative, the patients were asked to score the frequency and severity and whether each symptom had improved, worsened, or remained the same as before their procedure. Their perception of the procedure also was scored as to be a success, a partial success, or not a success.
We technically approached these patients with the surgical intention of a redo Heller myotomy. The approach is the same as in any redo, the patient is placed in a low lithotomy position so that the surgeon may stand between the legs while operating. Pneumoperitoneum is established with a Veress needle. The camera port is placed 2 cm to the left of the midline and 10 cm below the costal margin. The upper two ports are used by the surgeon and should form an equilateral triangle with the camera port. The liver retractor and first assistant ports are placed at the level of the camera port in the anterior axillary line.
In this procedures multiple adhesions and anatomy distortions are found because of previous surgeries. So, as in any reoperation, the principle is, first, to dissect the esophagus, the stomach, and the fundoplication free from the crura, the liver, and other adjacent structures. At last, if there is a previous fundoplication, you have to undo the fundoplication completely. The most important issue is to carefully work over the anterior face of the GEJ trying not to open the submucosal/mucosal layers of the previous myotomy. When a correct redo Heller myotomy is not technically possible because of the local anatomical situation, fibrosis, or tissue damage, we perform the resection of the GEJ and a Roux-en-Y reconstruction.
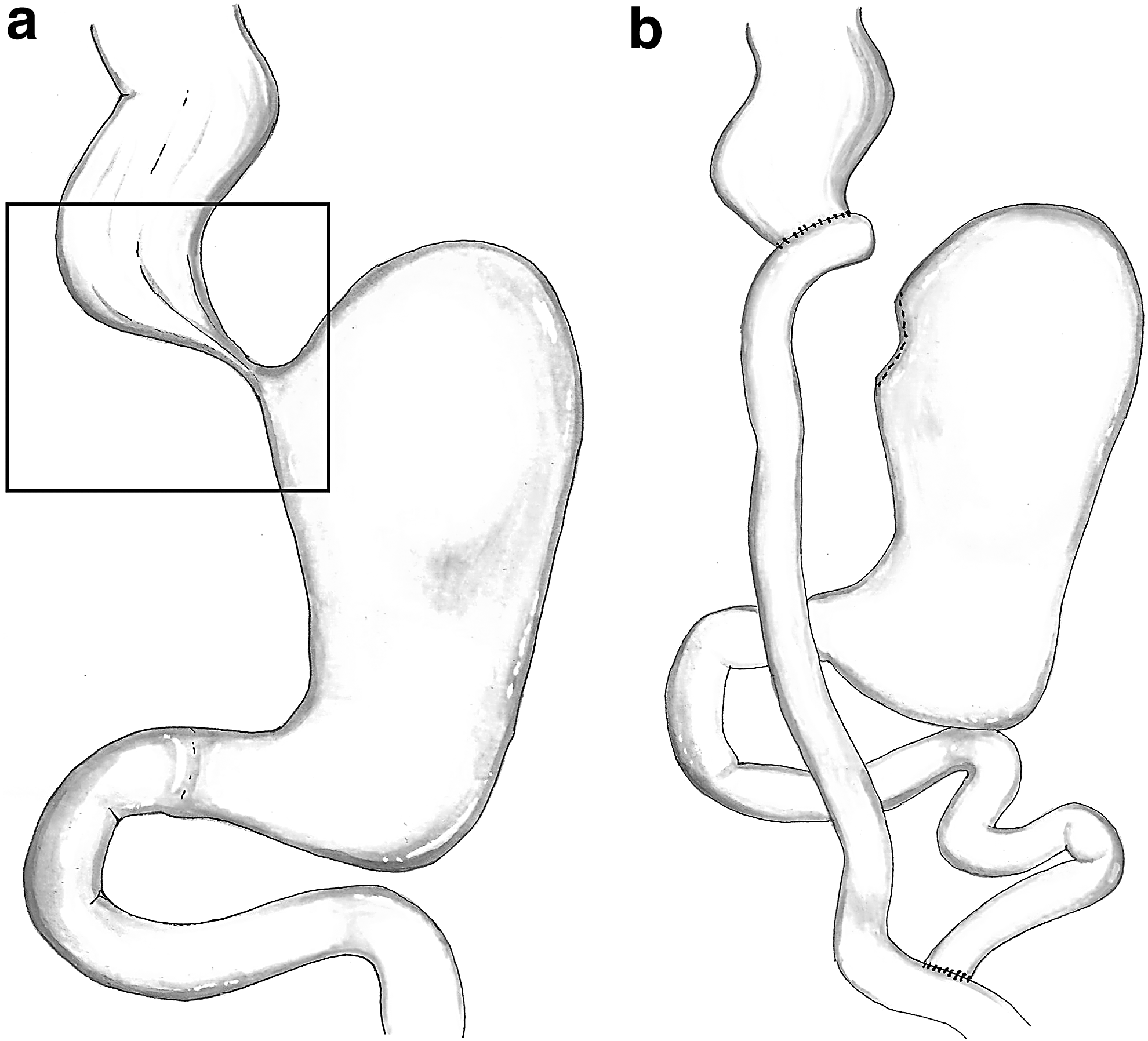
If you decide to continue the approach with either open or laparoscopic, the technique is the same. The inferior mediastinal esophagus dissection is performed as cephalad as possible to achieve the best length for intra-abdominal esophagus. An esophagotomy in the anterior wall of the esophagus is performed cephalad to the superior edge of the previous myotomy, if seen, or to the fibrosis area. The head of the anvil is inserted inside the esophagus. Then, the point of the anvil is extracted through the posterior wall of the esophagus. With a 60 mm length linear stapler, the esophagus is transected immediately cephalad to the esophagotomy. With two or more 60 mm length linear staples, the stomach is transected distally to the inferior edge of the myotomy and at least 4 cm from the GEJ. Generally, the first suture section is across the GEJ, and then the gastric section line is directed vertically toward the angle of His.
Roux-en-Y reconstruction is performed transectioning the jejunum 30–40 cm distal from the Treitz angle (biliopancreatic limb). Then, a 25-mm EEA stapler is introduced through the Roux limb, enabling an intracorporeal end-to-side esophagojejunal anastomosis. Then, 60–70 cm distal from the esophagojejunal anastomosis, a side-to-side entero-entero anastomosis is performed finalizing the Roux-en-Y reconstruction (alimentary limb). The remaining stomach is excluded from the passage of the food and is left intact for eventual future use (e.g., if needed in an esophagectomy) (Fig. 1).
Results
From January 2008 to January 2018, 207 patients with diagnosis of esophageal achalasia underwent surgery in our institution. In 5 patients, we performed the resection of the GEJ along with a Roux-en-Y reconstruction for recurrent dysphagia after Heller myotomy and fundoplication, with at least 1 year of follow-up. All these patients had their initial operation in another institution.
There were 4 women and 1 man, with ages ranging from 22 to 57 years (mean 42 years). All the patients had had an abdominal approach, 4 patients had had two surgical procedures, and all were dilated more than one time (range 2–5 dilations) with poor response. The mean time between the last surgical procedure and the resection of the GEJ and a Roux-en-Y reconstruction was 7.4 years (range 3–13 years) (Table 1). The main symptoms of presentation were dysphagia (100%) and regurgitation (60%). All the patients had UGI, 3 patients presented a Stage II disease, and 2 patients a Stage III disease (Fig. 2). Manometry showed in all patients an absence of esophageal peristalsis with impaired relaxation of the LES.
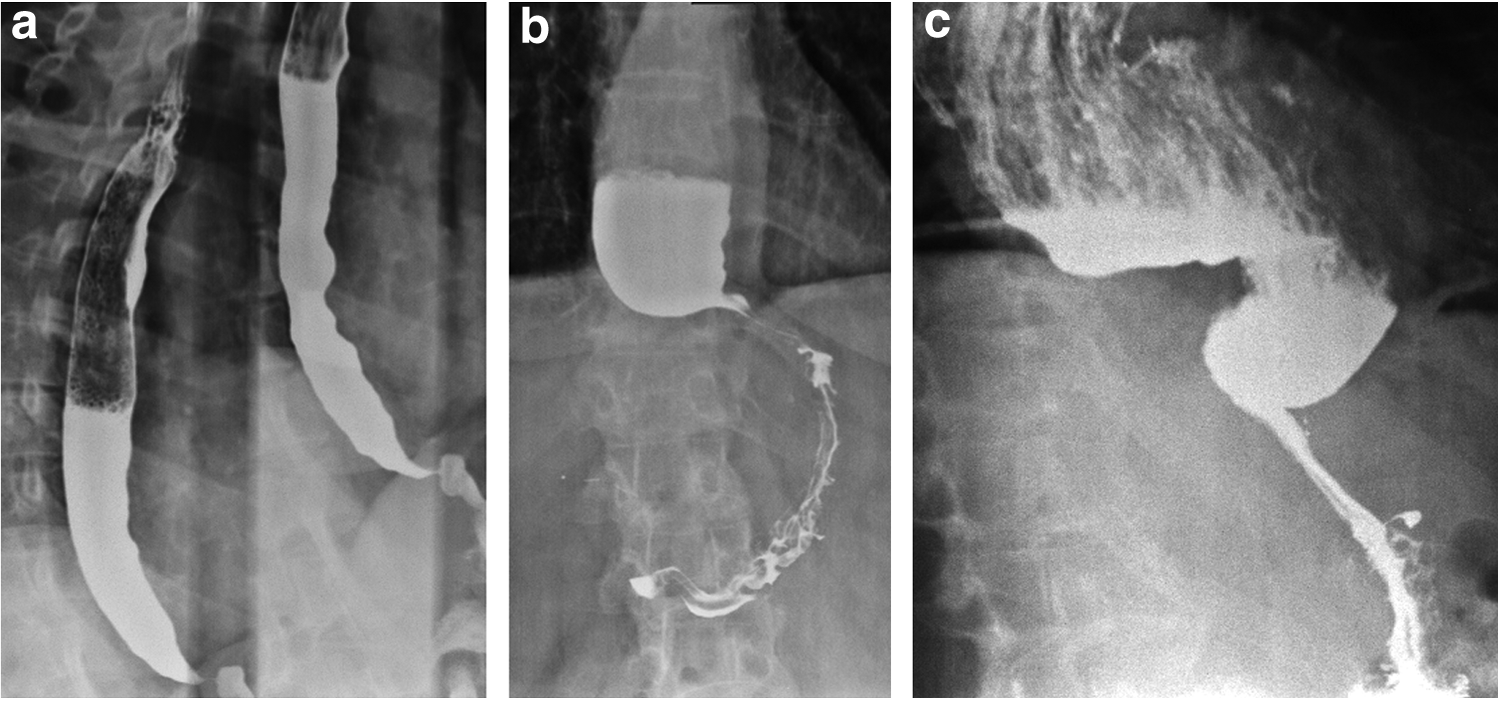
Preoperative contrast esophagram showing
Results
RGEJYR, resection of gastroesophageal junction and Roux-en-Y reconstruction.
In all 5 patients, laparoscopic exploration with the primary intention of a redo Heller myotomy was performed. In 4 cases, we found what we interpreted as a fundoplication and in every case it was taken down. In 3 patients, we can say that an incomplete myotomy was the cause of recurrent dysphagia, and in the other 2 patients, we could not be certain of the cause of recurrent dysphagia. In 3 cases, the fibrosis or scarring and previous adhesions made it impossible to do a correct redo Heller myotomy, and in the other 2 cases, during the release of adhesion and fibrosis, tissue damage in the GEJ happened. The resection of the GEJ and a Roux-en-Y reconstruction was performed in all these patients. The operating time was 164–215 minutes.
Postoperatively, all the patients started liquids through the nasojejunal feeding tube on the first postoperative day. We were very conservative in these patients, and we did an UGI in the 6th postoperative day. Progression to liquid diet is done on the 7th day and to soft diet on the 8th day. In 1 patient, UGI showed a leak from the anastomosis, which was managed conservatively (Clavien II). One patient developed a leak from the esophagojejunal anastomosis in the 4th day and needed a thoracoscopy with a thorough wash and toilette for a pleural abscess and a chest tube was left (Clavien IIIb). The patient went on parenteral nutrition. The leak was hard to resolve. Endoscopic clipping and placement of an Ovesco® device was tried to resolve the leak, but with mild results. Finally, after 2 months, the leak was closed. The patient was discharged on the 65 postoperative day. The median length of stay was 9 days (range 9–65 days).
The mean follow-up was 34 months (range 13–62 months). Questionnaire to assess postoperative dysphagia revealed for frequency with a median of 0 (range 0–2) and for severity with a median of 0 (range 0–4). All the patients reported a marked improvement of their dysphagia. The median overall satisfaction after resection of the GEJ and a Roux-en-Y reconstruction was 9 (range 7–10). Patients were asked for postoperative heartburn, and none of the patients referred to have it (Table 2). UGI revealed a good esophageal emptying through the esophagojejunal anastomosis in all the patients (Fig. 3).

Postoperative contrast esophagram showing good esophageal emptying through the esophagojejunal anastomosis in
Postoperative Symptoms and Overall Satisfaction After RGEJYR
RGEJYR, resection of gastroesophageal junction and Roux-en-Y reconstruction.
Discussion
On general rules, the treatment of achalasia focuses on symptom resolution. In the wide variety of procedures, it seems that in the end they all aim to generate relaxation, weakening, or breakage of the muscular fibers of the LES. The therapeutic options vary with different percentages of success in the medium and long term. Long-term relief of symptoms has made laparoscopic Heller myotomy the procedure of choice.7,8 However, there is a reported rate of ∼10%–15% failure in these procedures.
9
In the literature, inconsistently, some preoperative factors that predict poor outcome after myotomy are considered, such as severe preoperative dysphagia, hypotensive LES, sigmoid esophagus, the use of endoscopic balloon dilations, and botulinum toxin before myotomy.
10
The management of this subgroup of patients is controversial. The most important causes of surgery failure are:
Incomplete myotomy: inadequate section, in length or depth, of muscle fibers. Clinically, in these patients, dysphagia does not improve post-procedure or appears in the early postoperative period. It is always recommended to perform an extended myotomy, meaning technically, a section of the longitudinal and circular esophageal muscle fibers at least 4 cm above the GEJ, and distally at least a 3 cm complete gastric myotomy. Fibrotic scarring of the myotomy: usually, the clinical recurrence appears in the late postoperative period. Cancer: the association between achalasia and esophageal or GEJ cancer is known.
11
Once the failure of the treatment has been detected, the patient should be re-studied with UGI, UGE, and esophageal manometry. In this way, the cause of the dysphagia can be diagnosed and the appropriate treatment implemented. Due to the complexity of these reoperations, the first line of treatment is represented by conservative therapies, in which access to the fibrotic area generated by surgery is avoided.
There are multiple treatment options for the persistence of symptoms. Nonsurgical techniques include injection of botulinum toxin, endoscopic balloon dilation, and POEM. The injection of botulinum toxin is reported to lead to a 71% success rate after the year of application; it is a safe technique, but with limited efficacy in the long term. 12 Endoscopic balloon dilation allows an incomplete myotomy or fibrosis to be easily resolved in most of cases, showing a 75% resolution of symptoms for recurrent dysphagia after Heller myotomy. 4 Unfortunately, it carries the risk of perforation, which is around 5% with each dilation. 13
Finally, the POEM should be highlighted. Onimaru et al. 14 reported the use of POEM in 10 patients with persistent or recurrent dysphagia after Heller myotomy or pneumatic dilation, revealing symptomatic improvement and a lower resting pressure of the LES in a short-term follow-up. We should wait for more studies with longer follow-up to indicate this technique, but it should be taken into account in the near future. The counterpart represented by this procedure is the post-procedure gastroesophageal reflux, which must be opposed to the benefits of an endoscopic approach. Several reports have shown that gastroesophageal reflux reaches 50% or more in the first year of follow-up. 15
The failure of conservative options leads us to think about surgical alternatives. They are multiple and with different results in terms of morbidity and mortality, surgical effects, and success rate. From the strictly technical point of view, it should be emphasized that redo operations of functional esophageal pathology are extremely difficult. Among the different surgical options, the redo Heller myotomy with or without a valvuloplasty is probably the most valued option. Most patients improve substantially with this intervention with a success rate reported in almost 80%. 16 In cases of marked fibrosis, a possible option is to perform the myotomy on the posterior or lateral side of the esophagus and thus avoid an altered area of the previous surgery.
In the absence of satisfactory results, the need to discuss an alternative surgical procedure other than a redo myotomy is generated. The existing options to stand out are:
Cardioplasty with partial gastrectomy and Roux-en-Y reconstruction: Procedure known as the Serra-Doria operation, 17 in which a latero-lateral anastomosis is made between the esophagus and the gastric fundus (Gröndhal type cardioplasty 18 ) plus a partial gastric resection with a Roux-en-Y reconstruction. This procedure presented a low mortality and dysphagia improvement in all patients; however, short-term complications could be perforation or fistula in 10% of the patients and its long-term main complication is gastroesophageal reflux disease (GERD) and esophagitis. 17 Similar results reported by Braghetto et al. presenting an inversed Y cardioplasty plus a truncal vagotomy-antrectomy and a Roux-en-Y gastrojejunostomy. They found improvement of dysphagia in all patients and low morbidity. Gastroesophageal reflux symptoms were present in 25% of the patients without esophagitis. 19
Since these procedures involve a partial gastrectomy, it prevents the use of the stomach as a possible esophageal replacement in a possible future esophagectomy if recurrent symptoms of dysphagia or failure of the procedures occurs.
Esophagectomy: This is considered as the last option in the treatment of achalasia. We know that good results for recurrent dysphagia are achieved after esophagectomy in comparison with the other options, and there is no question that an esophagectomy reliably restores the ability to swallow.20,21 But we also know that esophagectomy is far from being free of complications, including anastomotic leak (10%), laryngeal nerve injury (5%), bleeding (2%), and chylothorax (2%), 22 and the mortality is not insignificant, being reported up to 5.4% in these cases. 23
As we have shown previously, all the procedures we mentioned before have their advantages and disadvantages when approaching a patient with recurrent dysphagia after Heller myotomy and fundoplication. For those cases where a redo Heller myotomy is not technically possible, we present a new procedure.
Our series of 5 patients shows that the patients with achalasia whose laparoscopic Heller myotomy fails and whose dysphagia does not resolve with endoscopic dilation can be treated successfully with the resection of the GEJ and Roux-en-Y reconstruction. Although it was not described previously to treat achalasia, this procedure meets three important findings.
First, it had an excellent effect on symptoms, showing a complete resolution of frequency and severity of dysphagia in almost all 5 patients, and if reported, it was very infrequent and of mild severity. This was reaffirmed by the high overall satisfaction of patients after the procedure. Moreover, the patients did not complain of heartburn, which is another positive key factor of this procedure due to the Roux-en-Y reconstruction, which should avoid the possibility of symptoms of postoperative GERD. This is an advantage compared not only with Heller myotomy with or without fundoplication but also with the previous procedures named.
Second, it allows the organ of natural replacement of the esophagus, the stomach, to be preserved in case an esophagectomy is needed in the future for recurrent dysphagia after the procedure.
Third, it showed an acceptable morbidity and no mortality. Although we had in two cases a confirmed anastomosis leak, only one needed a long workout to get resolved. We assumed that probably this is the most delicate technical issue with this procedure, knowing that this anastomosis is performed over a scarred tissue and altered anatomical situation.
We know that this is a short series of patients, and more patients are needed for conclusive statistical results. However, the excellent symptomatic evolution with this procedure makes us think that this is an effective alternative for the treatment of recurrent dysphagia when a redo Heller myotomy is not technically possible. This should be a previous option or procedure to be taken into account when esophagectomy is considered as the only last option for recurrent dysphagia.
Conclusion
In our short series of patients, the resection of the GEJ and Roux-en-Y reconstruction was an excellent treatment for recurrent dysphagia after Heller myotomy. Patients resolved symptoms of dysphagia and were highly satisfied after the procedure. Patients did not report symptoms of GERD after the procedure. We think this procedure should be taken into account as a better alternative to esophagectomy for patients who have failed Heller myotomy and subsequent dilation and when a correct redo Heller myotomy is not technically possible.
Footnotes
Disclosure Statement
No competing financial interests exist.