
Abstract
Abstract
Background:
To overcome the limitations of single-port laparoscopic myomectomy (SP-LM) and robotic single-site myomectomy (RSSM), we designed a new surgical technique, the so-called hybrid RSSM (H-RSSM), by integrating the advantages of both procedures. This study describes the surgical technique of H-RSSM and reports our initial experiences.
Materials and Methods:
Between February 2018 and September 2018, H-RSSM was performed in 25 women with symptomatic fibroids. During the H-RSSM, the enucleation of the fibroid was carried out using single-port laparoscopy and the uterine defect was repaired using robotic single-site surgery. To assess the feasibility and efficacy of H-RSSM, the results of this study were compared with those of our previous study on SP-LM and its modified surgical technique, so-called single-port laparoscopically assisted transumbilical ultraminilaparotomic myomectomy (SPLA-TUM).
Results:
The mean operation time, hemoglobin change, return of bowel activity, and length of hospital stay were 69.4 ± 18.2 minutes, 1.2 ± 0.9 g/dL, 37.1 ± 15.5 hours, and 4.0 ± 0.8 days, respectively. There was no conversion to laparotomy or multiport laparoscopy. There were no surgical or wound complications. Comparing with SP-LM and SPLA-TUM, H-RSSM had significantly shorter operation time and return of bowel activity.
Conclusion:
H-RSSM can reduce operating time and the conversion rate to multiport laparoscopy and can be considered a feasible alternative for selected patients with symptomatic fibroids. However, further studies are needed to clearly demonstrate these benefits.
Introduction
Given its excellent cosmetic outcome and reduced port site morbidity, single-port laparoscopic myomectomy (SP-LM) could be an ideal surgical modality for women with symptomatic fibroids who wish to preserve fertility.1–3 However, SP-LM is inevitably accompanied by technical and ergonomic difficulties, especially in uterine suturing. 2 Therefore, to overcome the challenges of SP-LM, several modified surgical techniques have been developed and reported.4–6
In the past decade, robotic-assisted laparoscopic myomectomy has been accepted as an alternative that can overcome the limitations of laparoscopic myomectomy by providing improved precision and dexterity and a three-dimensional view.7–9 In addition, robotic single-site myomectomy (RSSM) has emerged as a result of the advances of Da Vinci® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA) and its instruments, and studies on this procedure have been reported.10,11 However, RSSM is also thought to have technical problems; unlike SP-LM, these problems are especially evident for fibroid excision due to the limitations of the robotic surgical system and its instruments.
We designed a new surgical technique, the so-called hybrid RSSM (H-RSSM), by integrating the advantages of both conventional SP-LM and RSSM to overcome the limitations of each procedure. This study describes the surgical technique of H-RSSM and reports our initial experiences with the procedure.
Materials and Methods
In this prospective observational study, the subjects were all women scheduled to undergo H-RSSM at our hospital between February 2018 and September 2018.
The exclusion criteria were women who had more than seven fibroids and whose operation time was predicted to be longer than 3 hours if laparoscopic myomectomy was performed. For these women, institutional policy is to perform laparotomic myomectomy. All women who did not meet the exclusion criteria were informed of the advantages, disadvantages, and limitations of H-RSSM versus conventional SP-LM. Each participant selected the surgical procedure she would undergo, and consent was obtained. The choice of surgical modality was not influenced by the patient's history of previous abdominal surgery or body mass index (BMI).
To assess the feasibility and efficacy of H-RSSM, the results of this study were compared with those of our previous study on SP-LM and its modified surgical technique, so-called single-port laparoscopically assisted transumbilical ultraminilaparotomic myomectomy (SPLA-TUM).4,6
The operation time was defined as the interval between skin incision and closure; the return of bowel activity was defined as the period from the end of general anesthesia to the first occurrence of bowel gas passage, and postoperative fever was defined as a body temperature ≥38°C on two consecutive occasions at least 6 hours apart, except during the first 24 hours. This study was approved by our institutional review board.
Operative technique
Under general anesthesia, the patient was placed in a dorsal lithotomy position, and both arms were tucked at the sides. After prepping and draping were performed in the usual manner, a uterine manipulator and Foley catheter were placed. An ∼15-mm vertical skin incision was made through the center of the umbilicus, extending to the intraperitoneal cavity. The GelPoint™ Advanced Access Platform (Applied Medical, Rancho Santa Margarita, CA) was established, and three trocars, a 12-mm sleeve and two 10-mm sleeves, were introduced through the GelSeal™ cap in a triangular configuration (Fig. 1A).
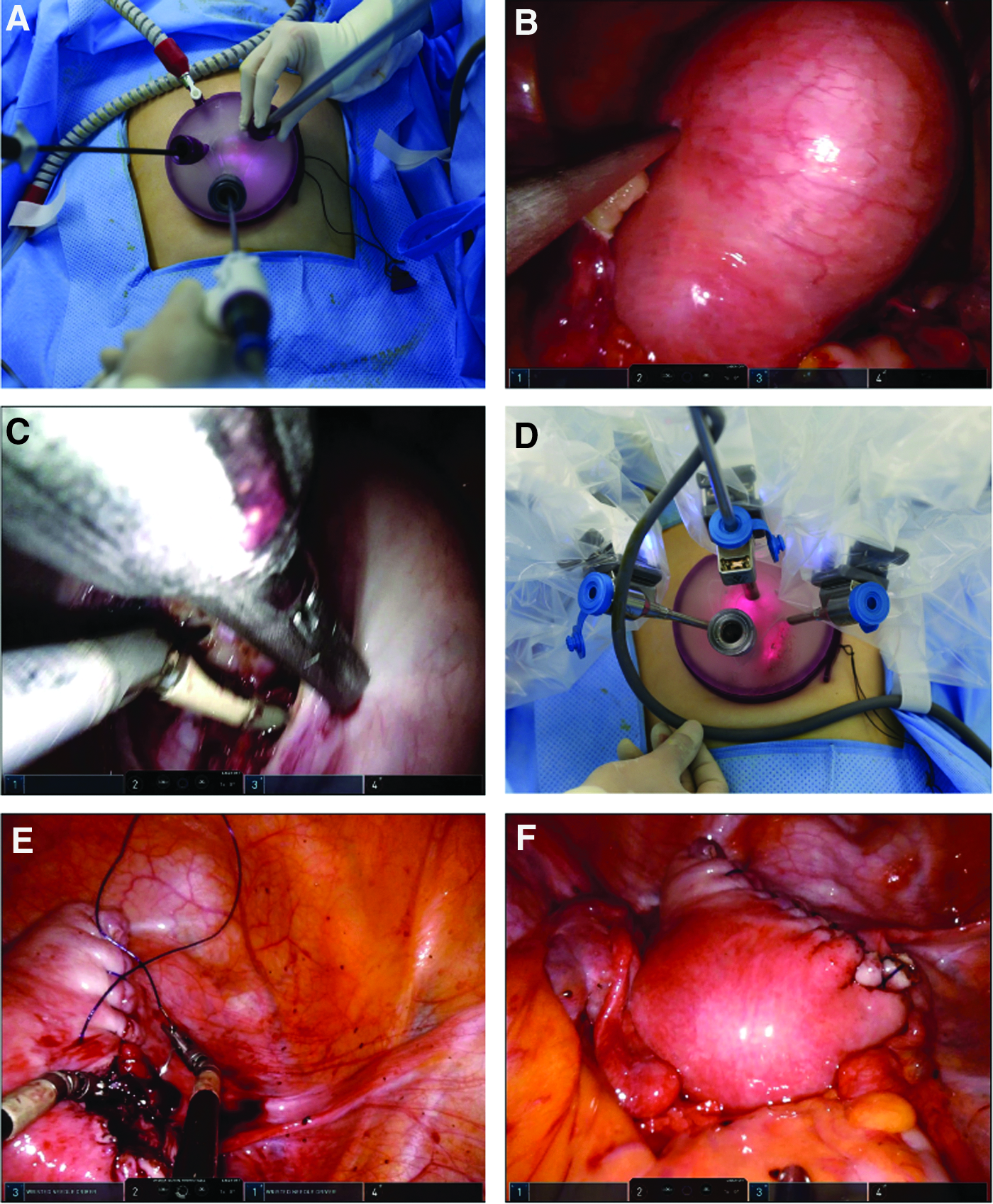
First, in the laparoscopic enucleation of the fibroid phase, a dilute solution of vasopressin (10 IU/100 mL normal saline) was injected into the tissue around the fibroid (Fig. 1B). A vertical or elliptical uterine incision was made over the fibroid using Thunderbeat™ (Olympus Medical Systems Corp., Tokyo, Japan) and was extended to the cleavage plane. The fibroid was grasped with conventional 10-mm laparoscopic claw forceps or conventional 5-mm laparoscopic forceps to provide countertraction and was dissected out of the uterus (Fig. 1C).
Second, in the robotic-assisted laparoscopic repair of uterine defect phase, after the three trocars were removed from the GelSeal cap, a cannula for a Da Vinci endoscope, two curved cannulas for 5-mm robotic instruments, and a 12-mm assistant trocar were introduced through the GelSeal cap. The right and left robotic instrument cannulas crossed at the umbilicus level under the cap (Fig. 1D). The Da Vinci Xi® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA) was docked on the right side of the patient. Two wristed needle drivers were inserted into the instrument cannulas. The uterine defect was repaired in multiple layers with a bidirectional barbed suture (Quill™-0 or 2–0; Angiotech Pharmaceuticals, Inc., Vancouver, BC, Canada) (Fig. 1E).
Third, in the fibroid extraction and umbilical closure phase, the robotic instruments and cannulas were removed, and the robot was undocked. Two additional trocars for conventional laparoscopy were introduced through the GelSeal cap. The resected myoma was morcellated and extracted using a scalpel in the retrieval bag. After intraperitoneal irrigation, the uterine incision was covered with an absorbable adhesion barrier (Interceed®; Gynecare, Somerville, NJ). The GelPoint platform was removed, and the incision was closed layer by layer (See Supplementary Video S1).
Statistical analysis
R® version 3.4.2 (The R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses, and P values < .05 were considered statistically significant. Continuous variables are expressed as the mean ± standard deviation, and categorical variables are reported as numbers (percentages). Each variable was confirmed to follow a normal (Gaussian) distribution with the Shapiro–Wilk test. The one-way analysis of variance test or Kruskal–Wallis chi-squared test was used for the statistical analysis of continuous variables. Pearson's chi-squared test or Fisher's exact test was used for the statistical analysis of categorical variables.
Results
During the study period, H-RSSM, SP-LM, and laparotomic myomectomy were performed in 25 women, 14 women, and 1 woman, respectively.
The detailed demographic and clinical characteristics of the resected fibroids in women who underwent H-RSSM are given in Tables 1 and 2. Eleven women had a history of previous abdominal surgery, including appendectomy, laparotomic myomectomy, cesarean deliveries, and robotic single-site cholecystectomy.
Participant Demographics
Using a one-way ANOVA test.
Using Pearson's chi-squared test.
Using the Kruskal–Wallis chi-squared test.
Using Fisher's exact test.
ANOVA, analysis of variance; BMI, body mass index; H-RSSM, hybrid robotic single-site myomectomy; SD, standard deviation; SP-LM, single-port laparoscopic myomectomy; SPLA-TUM, single-port laparoscopically assisted transumbilical ultraminilaparotomic myomectomy.
Clinical Characteristics of the Resected Fibroids
Using the Kruskal–Wallis chi-squared test.
Using Fisher's exact test.
Using Pearson's chi-squared test.
H-RSSM, hybrid robotic single-site myomectomy; SD, standard deviation; SP-LM, single-port laparoscopic myomectomy; SPLA-TUM, single-port laparoscopically assisted transumbilical ultraminilaparotomic myomectomy.
Table 3 gives the operative results. There was no conversion to laparotomy or multiport laparoscopy and no surgical or wound complications in any of the women who underwent H-RSSM. The histopathological findings for all patients were leiomyoma.
Operation Outcomes
Using the Kruskal–Wallis chi-squared test.
Using Fisher's exact test.
H-RSSM, hybrid robotic single-site myomectomy; SD, standard deviation; SP-LM, single-port laparoscopic myomectomy; SPLA-TUM, single-port laparoscopically assisted transumbilical ultraminilaparotomic myomectomy.
A comparison of the H-RSSM, SP-LM, and SPLA-TUM patients showed no significant difference in the clinical characteristics except BMI (Tables 1 and 2). In terms of operative outcomes (Table 3), there was no difference among the surgical groups, but H-RSSM had significantly shorter operation time and return of bowel activity.
Discussion
Single-port laparoscopic surgery has been used in almost all fields of gynecology, and many studies on this method have been reported with the development of new instruments and surgical techniques.1,2,4,6 Compared with women who undergo hysterectomy, women who undergo myomectomy are younger and might be more sensitive to postoperative cosmetic outcomes.3,12 In this regard, SP-LM may be the best choice for women with scheduled myomectomy. However, SP-LM is difficult to use in some cases because it is inevitably accompanied by technical difficulties, particularly in suturing and knotting. 6
Because the robotic surgery system provides a three-dimensional view and improves precision, stability, and dexterity, RSSM can offer a new alternative to SP-LM. However, RSSM has not yet been popularized, although some studies on the technique have been published.10,11 The authors believe that this slow uptake of RSSM is due to the following limitations: first, with the exception of wristed needle drivers, the robotic instruments for the Da Vinci single-site platform lack pitch and yaw of the instrument tip. The absence of these functions has led to challenges during fibroid enucleation in particular. 11 Second, robotic instruments for the Da Vinci single-site platform are semirigid, and relatively long metal cannulas (300–250 mm) are used to mechanically support them. Considering the length of the instrument tip and the long metal cannula located below the umbilicus level, the enucleation of large fibroids is difficult in RSSM due to limited workspace. Third, semirigid robotic instruments do not have sufficient mechanical strength for traction and countertraction during the enucleation of myomas. Fourth, the robotic surgical system does not provide haptic feedback or tactile sensation. The absence of tactile sensation is a serious drawback in myomectomy because hidden myomas that were detected in preoperative imaging studies are often encountered during surgery. Although magnetic resonance imaging can provide sufficient information about myomas, the anatomical location of the remaining myomas can be unknown in some cases in which the uterus rotates after a large myoma has been removed. We believe that the aforementioned limitations of RSSM have a greater impact on fibroid enucleation than uterine reconstruction, and we have developed the H-RSSM to overcome these limitations.
As given in Table 3, H-RSSM had a shorter operation time than SP-LM or SPLA-TUM. In general, robotic surgery has been reported to require longer operation time due to the docking time required9,13; however, our result was not consistent with such reports. Although the surgeon's (Dr. J.H.L.) experience of ∼2000 single-port laparoscopies and ∼400 robotic single-site laparoscopies contributed, in part, to the shortening of the operation time, the authors believe that this result was due to the advantages of the H-RSSM, in which fibroid enucleation is performed with laparoscopy and suturing is performed with robotic surgery. In other words, we consider that single-port laparoscopy may be more effective than robotic single-site surgery for fibroid enucleation because the single-port laparoscopy maintains some tactile sensation, provides sufficient mechanical strength for traction or countertraction through the use of conventional laparoscopic instruments, and does not use the long metal cannulas that restrict the operating workspace in robotic systems. However, robotic single-site surgery may be more useful for uterine reconstruction than single-port laparoscopy because robotic single-site surgery provides precise, stable, and dexterous suturing for repairing the uterine defects. In addition, in our previous study on SP-LM and SPLA-TUM, 3 women (3/92, 3.3%) were converted to multiport laparoscopy due to the difficulty of suturing, as given in Table 3. 6 Considering this point, the fact that there was no conversion to laparotomy or multiport laparoscopy in this study seems to support our view.
The authors used the GelPoint platform instead of the Da Vinci single-site silicone port for the H-RSSM because the GelPoint platform has the following theoretical advantages: (1) The distance between the target organ and the cannulas can be easily controlled. This adjustment during operation can be performed by advancing or retracting curved metal cannulas while pushing the clutch button of the robotic arm. Because robotic instruments are semirigid, it is important to adjust this distance between the target organ and the metal cannulas that support robotic instruments to effectively perform suturing. (2) Assistant trocars can be used effectively. The GelSeal cap has enough surface area to be inserted by the trocars and allows the position of the trocar to be changed as needed while maintaining pneumoperitoneum during surgery. (3) Crowding of instruments can be minimized. In the GelPoint platform, the assistant trocar does not penetrate the umbilical incision but is fixed in the GelSeal cap. Therefore, the crowding of instruments at the umbilical level can be minimized, and a 12-mm assistant trocar that permits the passage of a curved needle, gauze, or small specimen can be used relatively easily. (4) A wound retractor can maximally stretch a small umbilical incision in all directions and fix the peritoneum and skin. In addition, this enables the surgeon's finger to touch the uterus through the umbilical incision to find hidden fibroids after decoupling the GelSeal cap from the retractor while the uterus is pushing upward during laparoscopic myomectomy.
Further studies are needed to clearly confirm the advantages, disadvantages, and long-term obstetric outcomes because this study aimed to report on our initial experience with H-RSSM.
In conclusion, H-RSSM is a surgical technique that combines the advantages of laparoscopy and robotic surgery. The technique can reduce operating time and the rate of conversion to laparotomy or multiport laparoscopy, and it can be considered a feasible alternative for selected patients with symptomatic myoma. However, further studies are needed to clearly demonstrate these benefits.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.