
Abstract
Abstract
Introduction:
Laparoscopy has been shown to offer a safe alternative to laparotomy in hemodynamically stable pediatric trauma patients. Our purpose was to identify factors predictive of this approach and examine surgical outcomes.
Methods:
This is a retrospective cohort study using the ACS Pediatric Trauma Quality Improvement Program to examine pediatric patients who underwent exploration for blunt or penetrating abdominal trauma in 2014 and 2015. Patients with contraindications to laparoscopy were excluded. Multivariable modeling identified predictors of a laparoscopic approach. Secondary analysis assessed differences in outcomes and resource utilization between laparoscopy and laparotomy groups.
Results:
A total of 160 patients met inclusion criteria. Patients undergoing surgery in the northeastern (odds ratio [OR]: 2.25, 95% confidence interval [CI]: 1.26–4.03, P = .006) and western (OR: 2.03, 95% CI: 1.06–3.88, P = .032) U.S. regions had over two times greater odds of undergoing laparoscopy as those treated in the south. Patients injured by a firearm were significantly less likely to undergo laparoscopy than those suffering blunt injury (OR: 0.27, 95% CI: 0.13–0.55, P < .001). After adjustment, patients explored laparoscopically in comparison with those through laparotomy had decreased average length of stay (LOS) (mean difference [MD]: 2.55 days, 95% CI: 1.19–3.90, P < .001) and number of intensive care unit (ICU) days (MD: 1.13 days, 95% CI: 0.28–1.98, P = .01).
Conclusion:
Trauma laparoscopy may decrease LOS and ICU days in select pediatric patients requiring abdominal exploration; however, laparoscopy is not uniformly practiced in the United States. Targeted education and protocols for initial use of laparoscopy should be incorporated into hospitals treating this group to minimize morbidity and resource utilization.
Introduction
Minimally invasive surgical techniques have been shown to lead to improved outcomes, such as decreased postoperative pain, recovery time, and resource utilization. 1 Recently, laparoscopy has been increasingly used in support of patients with traumatic injuries, and has been shown to be safe and effective for both diagnostic and therapeutic purposes.2,3 Use of these techniques may be particularly important in children as physical examination is notoriously more difficult, and laparotomy carries increased risk of life-long morbidity such as wound complications and adhesive bowel disease. Data regarding outcomes of minimally invasive surgery (MIS) in pediatric trauma are limited, but emerging literature suggests reliable exclusion of injuries in stable patients, and decreased use of unnecessary laparotomy and its associated morbidity.4,5
The extent and predictors of laparoscopy utilization in pediatric patients being treated for traumatic injury are unknown, as are the potential differences in surgical outcomes related to minimally invasive versus open surgery. Our purpose is to examine utilization rates and factors associated with the use of minimally invasive surgery in a national cohort of pediatric trauma patients without contraindication to the use of minimally invase surgery (MIS), as well as evaluate surgical outcomes in this population.
Methods
On May 1, 2017, the study protocol and use of the ACS Pediatric TQIP were reviewed by the University at Buffalo Institutional Review Board and deemed to meet qualifications for exemption status (IRB ID: STUDY00001522).
Study design
A retrospective cohort study was performed using the ACS Pediatric TQIP, 2014 and 2015. The Pediatric TQIP utilizes the infrastructure of the National Trauma Data Bank (NTDB) and was implemented as part of the ACS TQIP with the goal of improving the quality of trauma care by providing a method of tracking patient outcomes and delivering feedback to participating centers. Participation in the program is open to all Level I and Level II ACS-verified or state-designated pediatric trauma centers or adult centers that treat children. Patient-level inclusion criteria are age ≤18 years; a valid trauma ICD-9 code excluding late effects superficial injuries and foreign bodies; mechanism of blunt, penetrating, or nonaccidental trauma; at least one Abbreviated Injury Scale ≥2 in body regions 1–8; emergency department (ED) or hospital disposition known; ED disposition was not to home, transferred, left against medical advice, or other; patient does not have advanced directives precluding life-sustaining interventions; patient does not have vital signs or Glasgow Coma Score (GCS) combination consistent with dead on arrival; and patient does not have severe burns. The Pediatric TQIP Participant Use File (PUF) data sets for 2014–2015 include data from 71 participating facilities and contains patient-, hospital-, and encounter-level variables including demographic information, comorbidities, physiologic data, injury mechanism and severity, diagnosis and procedure codes, as well as outcome data such as complications, length of stay (LOS), discharge disposition, and mortality.
We queried the 2014 and 2015 PUFs for patients aged 0–18 years suffering blunt or penetrating abdominal trauma who underwent an abdominal procedure. Patients with any absolute or relative contraindication to the use of laparoscopy were excluded. Absolute contraindication was defined as hemodynamic instability: this was determined using systolic blood pressure measurements according to age as recorded in the ED. Relative contraindications were defined as total GCS <14, injury severity score (ISS) ≥16, comorbidity of congestive heart failure, or diagnosis codes for traumatic shock, abdominal compartment syndrome, peritonitis, or abdominal rigidity. 6
Variables of interest
For descriptive bivariate and multivariable analyses, the main outcome variable was use of laparoscopy. We controlled for patient age, gender, race, mechanism of injury, hospital type (pediatric versus adult trauma center), payer status, hospital U.S. region, and hospital academic status. For analysis of surgical outcomes, the dependent variable was procedure type and outcome variables included complications, disposition, LOS, days in the intensive care unit (ICU), and days requiring ventilator support. There were no deaths in either the MIS or open groups. For complications, surgical site infection was defined as any superficial, deep, or organ space infection, and other site infection included urinary tract or catheter-associated blood stream infections. For disposition of transferred to another facility type, facilities included psychiatric hospitals, short-term general hospitals, or other hospital types.
Statistical analysis
Variables were summarized descriptively overall and by relevant demographic variables. Descriptive statistics such as frequencies and relative frequencies were computed for all categorical variables. Numeric variables were summarized using simple descriptive statistics such as the mean and variance. Univariate associations between variables were statistically assessed using standard procedures, including the t-test, the Kruskal–Wallis test, and the procedure of Freeman and Halton, an extension of Fisher's exact test for general contingency tables. 7 To evaluate the multivariate relationship between surgery type and patient, hospital, and encounter demographic factors, logistic regression was utilized based on maximum likelihood estimation of model parameters. Statistical significance of predictors in this case was determined using standard Wald tests. An intent-to-treat paradigm was utilized, categorizing all converted cases as part of the MIS group. All statistical analyses were performed using the R statistical programming language and P values <.05 were considered statistically significant.
Results
A total of 492 patients met inclusion criteria, having undergone an open (n = 332, 67.5%) or laparoscopic (n = 160, 32.5%) abdominal procedure for traumatic injury and were considered to have no contraindication to MIS. There were 45 (28.1%) MIS cases that were converted to open procedures. Details regarding selection of our study population are presented in Figure 1. The overall population was 77% male, 54% white, and 52% adolescent. Ninety-two percent of patients were treated at a pediatric trauma center and 51% were treated in the south. Of all patients, 66% had a blunt injury and nearly 48% had government insurance.
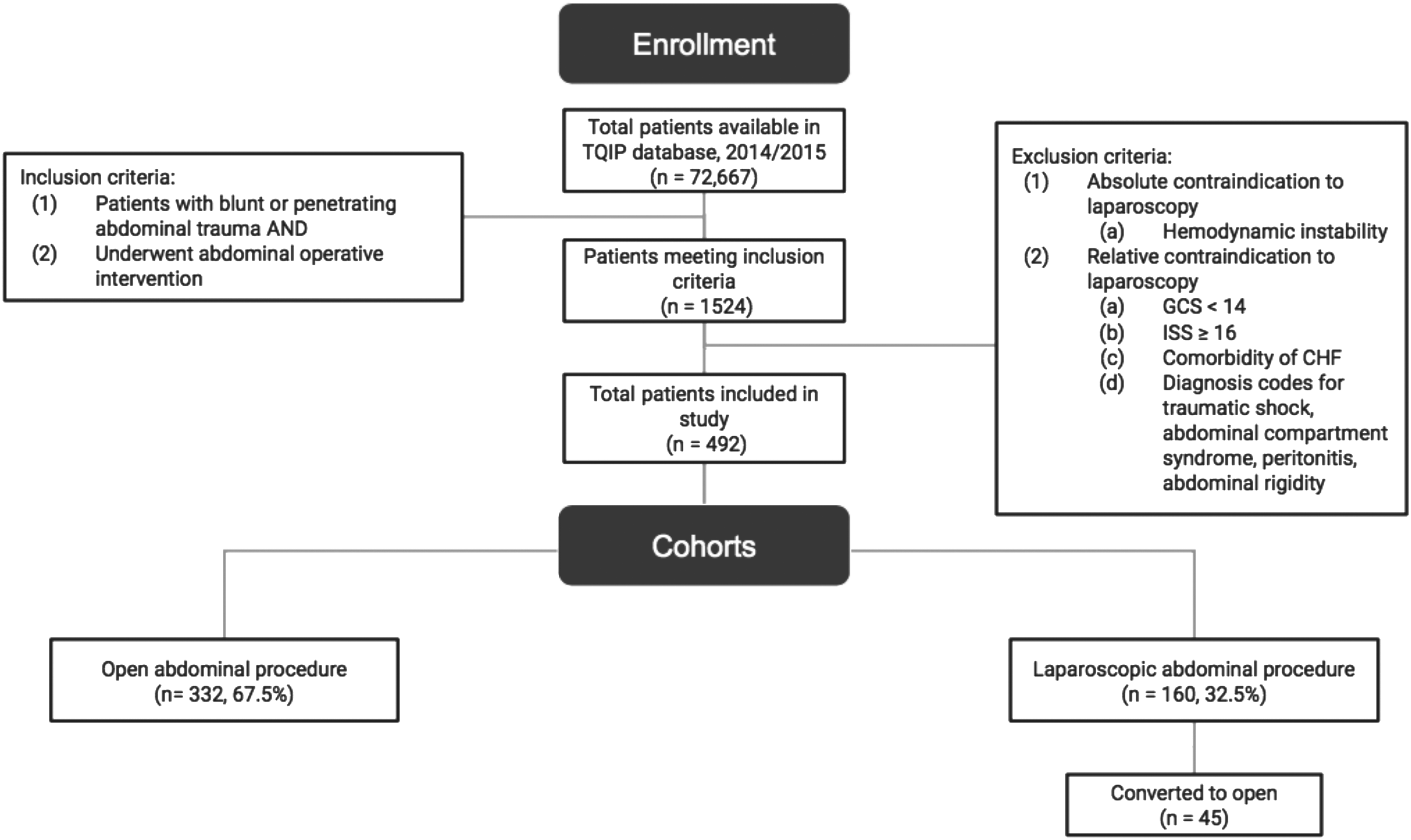
Flow diagram describing phases of patient selection.
Univariate analysis
We examined differences in our variables among our primary categories: those receiving open procedures and those receiving laparoscopic procedures (Table 1). On univariate analysis, there was found to be no statistically significant association between type of procedure performed and age group, gender, race, hospital type, payer, or hospital academic status. There was found to be an association between procedure type and both mechanism of injury and U.S. region. A significantly larger proportion of patients undergoing an MIS procedure had a blunt injury (76.3%, P < .001), and a significantly larger proportion of those injured with firearm underwent an open procedure (24.4%, P < .001); there were also differences in the proportions of patients receiving laparoscopic surgery according to U.S. region, with proportions of MIS versus open highest in the northeast and west and lower in the south (P = .018). The mean ISS was not different between groups.
Patient, Hospital, and Encounter Descriptive Statistics
Calculated using Fisher's exact test or aKruskal–Wallis.
Bold values are statistically significant.
ISS, injury severity score; MIS, minimally invasive surgery.
Multivariable analysis
On multivariable logistic regression, patients injured with a firearm were found to have significantly lower odds of undergoing a minimally invasive procedure (odds ratio [OR]: 0.27, 95% confidence interval [CI]: 0.13–0.55, P < .001) than those with a stab or blunt injury (Table 2). U.S. region was also identified as a significant predictor for undergoing MIS, with patients in the northeast region having the highest odds of undergoing a minimally invasive procedure than all other U.S. regions (OR: 2.25, 95% CI: 1.26–4.03, P = .022).
Odds of Undergoing Minimally Invasive Surgery
No MIS cases were performed in nonteaching hospitals.
Bold values are statistically significant.
CI, confidence interval; ISS, injury severity score; MIS, minimally invasive surgery; N/A, not applicable; OR, odds ratio.
On analysis of surgical outcomes between MIS and open groups (Table 3), the average adjusted LOS was 2.5 days shorter in the MIS group than the open group (mean difference [MD]: 2.55, 95% CI: 1.19–3.90, P < .001). Patients undergoing MIS also spent an average of 1 day less in the ICU (MD: 1.13, 95% CI: 0.28–1.98, P = .009). There was found to be lower odds of having any complication in the MIS group (OR: 0.62, 95% CI: 0.35–1.04, P = .070), although this finding did not reach statistical significance.
Outcomes of Minimally Invasive Surgery
There were 10 total encounters with missing data.
Bold values are statistically significant.
CI, confidence interval; ICU, intensive care unit; LOS, length of stay; MD, mean difference; MIS, minimally invasive surgery; OR, odds ratio; RTI, return to intensive care unit; RTO, return to operating room; VNA, visiting nursing association.
Discussion
Major findings and relevance
In this study, we have examined utilization of laparoscopy in pediatric trauma patients using a nationwide database that is representative of the overall pediatric trauma population of the United States. We found that in hemodynamically stable patients without contraindication to MIS, the overall utilization of MIS is <30%. We also found that although the conversion rate was ∼30%, there were no unanticipated returns to the operating room in that group, indicating no missed injuries. On multivariable analysis, U.S. region and mechanism of injury were the only factors found to be significantly associated with the use of MIS. Although the majority of the procedures were performed in the south, this area was the least likely to use MIS techniques. Patients injured with a firearm were also significantly less likely to undergo laparoscopy. Finally, analysis of surgical outcomes revealed that known benefits conferred by the use of laparoscopic surgery to the general population apply to pediatric trauma patients as well; specifically, the group undergoing a minimally invasive procedure experienced decreased average LOS and number of ICU days.
Minimally invasive surgery has been demonstrated to be an appropriate initial intervention for many patients with traumatic injuries. A 2016 systematic review and meta-analysis show that laparoscopy is safe, fast, and sensitive for the evaluation of penetrating abdominal trauma in a stable adult patient. 4 Although there were initial concerns of missed injuries with no increase in therapeutic management if injuries were found, these concerns have decreased in more recent years as laparoscopy has become a staple of surgical technique. 5 More recent studies show ∼100% sensitivity and specificity with very low missed injury rates.4,8–10 Standard examination technique has also been proposed to reduce chances of missed small bowel injury. 11 Studies in the pediatric population have been limited mainly to single or multi-institutional retrospective reviews; however, findings have been similar to those in adults, indicating that use of minimally invasive techniques in stable patients is safe and effective for both diagnostic and therapeutic purposes.3,10–14
Diagnostic and therapeutic laparoscopy have also been found to reduce laparotomy rates by up to 56%–62%.12,13 The primary benefits of laparoscopy over laparotomy include reduction in morbidity associated with negative laparotomy. Laparotomy carries a 20% morbidity risk, up to 5% mortality, and 3% risk of long-term complications. 12 The subxiphoid to pubic ramus incision is associated with greater postoperative pain, risk of infection and hernia, prolonged hospital stay, increased functional recovery time, and poor cosmesis. 14 Our study shows that ∼70% of patients who were potentially appropriate candidates for laparoscopy had an initial open procedure instead. This likely represents a large group of pediatric patients who could potentially have been spared an exploratory laparotomy, as the literature has demonstrated that even when injury severity or surgeon skill level necessitates conversion, the size of the incision may be limited to either trocar extension or minilaparotomy made feasible through initial injury localization and assessment through laparoscopy.15,16
The literature examining predictors of MIS in adult and pediatric patients undergoing elective surgery generally indicates that certain patient-, encounter-, and hospital-level factors do affect the likelihood of utilization of a laparoscopic technique. A study of hospital-level factors affecting the use of laparoscopy for several common surgical procedures in the adult population showed that use of MIS was highly variable according to both hospital factors such as size and location as well as procedure type. 17 Similarly, in children undergoing elective procedures, factors affecting use of MIS have been shown to include certain patient demographic factors such as age and insurance type. 18 In our analysis of this trauma population, the only factors significantly associated with MIS were U.S. region and mechanism of injury, with the likelihood of MIS decreasing for procedures performed in the south and when the mechanism was a firearm. The relative lack of associated factors and overall low utilization seen in our study may indicate that significant differences exist between trauma and elective settings in terms of how the determination of procedure approach is made. These may include the training of trauma surgeons in fellowship programs that do not emphasize minimally invasive techniques, or the fact that patients and their families typically have more choice regarding hospital and surgeon when receiving an elective procedure.
Regional variation in health care utilization such as the observed decreased likelihood for MIS in the southern United States is a complex issue with many underlying drivers. Supply side issues that have been identified in previous studies include varying provider beliefs or attitudes regarding appropriate treatment, individual provider abilities or skill sets, and regional norms.19–22 Alternatively, demand side drivers may include patient preference, health, and socioeconomic status.23,24 Although this type of variation has been researched extensively, there is still a large part of regional variation that is not well understood; regardless of causality, it is known that such variation is a source of inefficiency and higher cost. 25
The observation that patients experiencing injury by firearm are less likely to undergo a minimally invasive approach may be a reflection of traditional teaching emphasizing a more aggressive approach to firearm injuries; however, there is a growing volume of evidence supporting the use of laparoscopy for therapeutic purposes in addition to its well-accepted role in diagnosis. There is clear indication for laparoscopy in the stable patient injured by firearm when fascial penetration is questionable, as studies have demonstrated such benefits as reduced negative laparotomy rate, reduced morbidity, and shortened hospital stay.6,26 As a therapeutic tool, recent studies have found that in stable patients, laparoscopy may be beneficial at least as an adjunct, if not alternative, to laparotomy in patients with stab and gunshot wounds by allowing for exteriorization of bowel through smaller incisions, guided incision placement, or avoidance of laparotomy all together without an increase in missed injuries or high rates of conversion.2,10,27–29
Finally, use of laparoscopy as part of the management of patients with abdominal traumatic injuries has been shown to result in less morbidity as well as decreased resource utilization. A prospective study evaluating the use of diagnostic laparoscopy alone demonstrated that the use of laparoscopy (though all positive laparoscopies were converted to open) resulted in decreased hospital cost and LOS. 30 Zafar et al. utilized the NTDB to evaluate >4700 patients who underwent diagnostic laparoscopy and found decreased LOS compared with a group undergoing open surgery. 31 A retrospective review of stable patients who underwent either laparoscopy or laparotomy for abdominal stab wounds reported shorter hospital stay and operative time in the laparoscopic group. 32 Although some studies may have included a small number of children (the patient cohort in the study by Zafar et al. comprised ∼10% children of ages 0–15 years), our study compares surgical outcomes in a cohort comprised entirely of pediatric patients undergoing either laparoscopic or open surgery for abdominal trauma. Our results demonstrate that outcomes are similar in children as in adults, and those who receive a minimally invasive approach experience shorter LOS and fewer days in the ICU.
Limitations and strengths
In all statistical analyses, including assessment of surgical outcomes, we chose to define a laparoscopic approach on an intent-to-treat basis (we included all conversions to open in the laparoscopic category) to maintain consistency. This approach, however, inevitably leads to differential misclassification bias because patients who underwent an eventual open operation were included in the laparoscopic category for the assessment of surgical outcomes, and this may have resulted in underestimation of the true association between the operative approach and surgical outcome. Although this is a limitation of the study, it also indicates that our results may be viewed conservatively.
Other limitations of this study include those associated with administrative database research, including data entry errors and lack of granular details. For instance, although we observe that ∼30% of minimally invasive procedures were converted to open, details regarding reasons for the conversion such as change in patient hemodynamic status or intraoperative findings are not available to us. There is also oftentimes a delay from the time information is captured to the time it is available in database form for assessment and analysis, and this is the case in our study that utilized data from 2014 and 2015. There is also the potential for in-hospital data and coding bias. The Pediatric TQIP does not provide any information on surgeon experience or training, which may have been of some benefit to the present analysis. Although the Pediatric TQIP is a nationally representative database, participation by individual institutions is voluntary and limited to only ACS or state-designated Level I and Level II trauma centers admitting children, which may compromise the generalizability of study findings. In addition, although our patient cohort comprised entirely of those without contraindication to laparoscopy as defined by deliberately conservative criteria, and further adjustments were made during statistical analysis, we recognize the potential for unobserved bias present in observational studies; therefore, it should be noted that other factors relevant to determining procedural approach may have been present but not captured by the database and could be unaccounted for in our analysis.
As seen by examination of our data, only a very small percentage of pediatric trauma patients undergo immediate operative intervention for traumatic abdominal injuries, making analysis with a database beneficial for several reasons; we are able to not only examine larger number of patients than would be available through institutional data, but we can also limit the study timeframe to include only recent trauma encounters while still maintaining a sufficient number of patients for analysis. Much of the previous literature examining use of minimally invasive techniques in pediatric trauma patients has relied on retrospective institutional records over relatively extended periods of time to increase number of patients, during which time significant advancements in both technology and education have taken place.
Conclusions
Minimally invasive surgical techniques may be underutilized in the pediatric trauma setting, despite demonstrated improvements in patient outcomes and resource consumption. This study determined that in 2014 and 2015, the use of MIS techniques was associated with U.S. region and mechanism of injury, which might indicate cultural or educational differences in the training of trauma surgeons compared with those in other specialties with regard to minimal access surgery. As minimally invasive surgery is quickly becoming the standard approach for many types of procedures, certain advanced techniques should be incorporated into trauma training programs, as well as the creation of future protocols for the management of abdominal injuries in hemodynamically stable pediatric trauma patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.