
Abstract
Abstract
Background:
Since introduced in 2010, the transanal minimally invasive surgery (TAMIS) has been gaining popularity worldwide for local excision of benign and early-stage malignant rectal lesions of the proximal and mid-rectum. The aim of this study was to review our experience with the procedure, including mid-term oncological outcomes.
Materials and Methods:
This is a retrospective descriptive study. The data collected include all patients who underwent TAMIS procedure in a single tertiary institute.
Results:
Forty TAMIS procedures were performed on 38 patients, 78% men and 22% women, with a median age of 67 years. The indications were 24 benign lesions, 14 adenocarcinoma, and 1 neuroendocrine tumor. The average lesion size was 43.2 mm and the average distance from the anal verge was 8 cm (range 5–12). We had no intraoperative complications and overall the 30-day morbidity rate was 20%, of which only one was major complication. No perioperative mortality was encountered. After a mean follow-up time of 26 months we had 3 cases of local recurrence (21.4%) of which 2 cases had high-risk features on the primary TAMIS pathology and refused our advice for completion proctectomy. Hence, they were both treated eventually with adjuvant radiotherapy. The distant recurrence rate was 14.2%.
Conclusions:
The TAMIS procedure is an acceptable option for local excision of rectal lesions for carefully selected patients. It has overt benefits of lower morbidity and easier recovery compared with radical surgery. When it is utilized for early-stage rectal cancers, high-risk pathological features should prompt a completion proctectomy.
Introduction
Proctectomy with partial or total mesorectal excision is considered the gold standard procedure for all rectal cancers, allowing complete removal and pathological staging of the tumor and lymph node status,1–4 but it is associated with significant morbidity and mortality and an inevitable negative influence on quality of life.5,6 Hence, there is a continuous drive for an alternative less radical approach, by means of local excision for benign rectal lesions and possibly even for early-stage rectal cancers.7,8
The option for local excision of rectal lesions include either the conventional transanal excision or through transanal endoscopic surgery, where one of two platforms are usually being used; the transanal endoscopic microsurgery (TEM) or the newer transanal minimally invasive surgery (TAMIS). 9
The TAMIS technique, first introduced in 2010, 10 improves the standard transanal excision abilities by using specialized insufflation system with single-site port and laparoscopic optics and instruments, allowing better endoluminal visualization and resection of more proximal rectal lesions. The transanal access in TAMIS, which initially depended on the existing single-port surgery devices, is nowadays facilitated by the GelPOINT Path (Applied Medical, Rancho Santa Margarita, CA) or the single incision laparoscopic surgery (SILS) Port (Covidien, Mansfield, MA).11–13 In controversy to TEM, which requires specialized complex expensive equipment and a steeper learning curve, TAMIS equipment is readily available with easier setup. This makes TAMIS more accessible and approachable to the minimally invasive surgeon as well as more cost-effective.14–17 Similar to TEM, which showed in previous studies better oncological outcomes than the traditional transanal excision, by its higher rate of negative resection margins, lower incidence of lesion fragmentation, and lower overall recurrence rates,18–20 TAMIS has also been proven to be superior over standard transanal procedure for local excision of rectal masses. This is mainly due to TAMIS ability to provide high-quality resections.19,21
Patient selection plays a key role in TAMIS, since patients with benign lesions or histologically favorable, early-stage malignancy (uTis or uT1 uN0 M0 cancer) are considered candidates for the procedure as curative-intent surgery, whereas more advanced lesions still require standard resection. 22 An acceptable exception is patients who are medically unfit for major surgery and can be offered TAMIS procedure for more advanced lesions. For patients with questionable T1 versus T2 lesions with no evidence of nodal metastasis in preoperative evaluation, a TAMIS resection can serve as an “excisional biopsy,” 23 and in case of unfavorable histopathological results, radical surgery should be recommended.
The purpose of this study was to review our own experience with the TAMIS procedure in light of the current literature, with respect to preoperative, operative, and postoperative outcomes. We especially focused on the postoperative surgical outcomes, pathological results, the quality of the specimen resected, and the mid-term oncological outcomes.
Materials and Methods
Subjects
Cohort included all patients who underwent TAMIS procedure in a single tertiary medical center in Israel between July 2011 and November 2017. All procedures were performed electively by 1 of 5 certified colorectal surgeons.
Data were collected retrospectively from electronic medical records, including preoperative notes and radiological findings, surgical notes, postoperative follow-up notes, pathological reports, and outpatient's clinic charts of the patients. The study was approved by the institutional review board.
The following parameters were reviewed and analyzed: age, gender, American Society of Anesthesiologists (ASA) score, body mass index (BMI), comorbidities and perioperative immunosuppressive, steroid and anticoagulation therapy, lesion size, location and distance of lesion from the anal verge, intraoperative suturing and complication, length of stay, perioperative antibiotic treatment, and postoperative pathology, including resection margins, postoperative complications, readmission, and local and distant recurrence.
Statistics
Data were analyzed using the SPSS® statistical package (IBM, Chicago). All results are indicated by descriptive statistics—frequencies and means with standard deviations or medians, unless otherwise indicated. Data regarding overall survival and disease-free survival were gathered and analyzed as well.
The TAMIS procedure
All procedures were performed under general anesthesia, using either the GelPOINT Path or the SILS Port. Patient positioning in the operating room was dependent on the anatomic location of the tumor. For posterior lesions patients were positioned in high lithotomy, whereas anterior lesions usually required the patient to be positioned in a prone jack-knife position. After the insertion of the transanal port and its fixation above the anorectal ring, pneumorectum was established using CO2 insufflation with air seal insufflation system with pressure set at 15 mmHg. Standard laparoscopic instruments and optics were used for visualization and to perform the excision. The resection was performed using an energy instrument according to surgeon preference; monopolar, bipolar or ultrasonic, and suturing of the resection defect was done by surgeon decision as well.
Results
Cohort and demographics
A total of 40 TAMIS procedures were done during the study period for 38 patients (2 patients had undergone the procedure twice due to recurrence). All patients underwent the procedure at a single institute during the years 2011–2017.
Cohort included 31 male (78%) and 9 female patients (22%). The mean age was 67 years (SD = 8.6, range 50–87). Majority of patients (80%) were ASA score 2 (range 1–4). Mean BMI was 27.6 (SD = 4, range 20.8–38).
Preoperative parameters
During the preoperative work-up 24 patients (60%) were evaluated by transrectal ultrasound (TRUS), 2 patients (5%) by pelvic MRI, 4 patients (10%) had both TRUS and pelvic MRI, and 10 patients (25%) had no preoperative pelvic imaging. Thirty-four of all our patients (85%) had undergone preoperative rigid rectoscopy examination in the outpatient clinic. The indication for surgery according to preoperative biopsy was benign (e.g., adenoma, low-grade dysplasia [LGD], high-grade dysplasia [HGD]) in 24 patients (60%), carcinoma in situ in 4 patients (10%), invasive adenocarcinoma in 10 patients (25%), and neuroendocrine tumor in 1 patient (2.5%). Only 1 patient did not have preoperative biopsy and pathological diagnosis (Table 1).
Surgical Indications
s/p, status post.
Two patients of those diagnosed preoperatively with carcinoma were treated with neoadjuvant chemoradiation. Both had carcinoma with preoperative radiological T3 staging and the TAMIS procedure was done due to patient's preference to avoid major surgery. In the postoperative pathology one had TVA and continued follow-up, whereas the other one had T2 adenocarcinoma, eventually completed low anterior resection (which was complicated with multiorgan failure and death).
None of the patients were under immunosuppressive or steroid therapy during the procedure. One patient had anticoagulant therapy due to paroxysmal atrial fibrillation (PAF) and suffered from postoperative bleeding. The patient's perioperative comorbidities are detailed in Table 2.
Comorbidities and Perioperative Therapy
ASA, American Society of Anesthesiologists.
Operative parameters
The median lesion distance from the anal verge was 8 cm (range 5–12). 29.4% of lesions were located at the anterior wall, 35.3% posterior, 20.6% on the left, and 14.7% on the right. The average size of lesion was 43.1 mm with median of 40 mm (SD 8.6, range 15–90 mm). In 4 cases (10%) the lesion was excised in piecemeal, whereas the rest (n = 36, 90%) were excised as a whole, and all the surgical specimens were of full thickness with grossly negative resection margins. We had no intraoperative complication. There was only 1 case in which the peritoneal space was entered during the resection and the defect in the rectal wall was sutured with no other implication on the patient operative and postoperative course. Overall suturing of the defect after resection of the lesion was performed in 32 of the cases (80%), using either vicryl suture (n = 11, 34.4%) or vloc suture (n = 21, 65.6%). In 20% of cases no suturing was done. It should be mentioned that the only case in which the lesion (pedunculated polyp) was resected using endoGIA, a recurrence was found 3 months later and the patient had undergone another TAMIS procedure. One patient, who had the TAMIS procedure for benign sessile polyp, had simultaneous right colectomy at the same procedure due to colon carcinoma.
Postoperative outcomes
The median length of stay was 2.6 days (range 1–7). Most of our patients (n = 35, 87.5%) were treated with antibiotic preoperatively (Table 3). In the postoperative 30 days period 8 patients (19.5%) suffered from complications, out of which only 1 was a major complication; 4 had fever treated with antibiotics, 2 postoperative bleedings, of which 1 required hemostatic suture that was done at the clinic, and 1 patient was diagnosed with intraperitoneal perforation on the fifth postoperative day treated with laparoscopic loop sigmoid colostomy for diversion. Only 4 patients (10%) required rehospitalization in the 30 days following surgery; 1 due to fever, 2 had postoperative bleeding, and 1 had suffered from perforation of the rectum. Data are detailed in Table 4.
Perioperative Antibiotic Treatment
Postoperative Data
Pathological outcomes
Twenty-six patients (62%) had benign lesion in the operative pathology (6 adenomas, 8 LGD, 4 HGD, and 8 had granulation tissue), 1 patient had carcinoma in situ, 11 patients (25%) had carcinoma, and 2 patients had neuroendocrine tumors (Table 5). Among those patients who had carcinoma in the pathological result, 8 were T1, 1 was T2, 1 was T3, and another 1 was so fragmented that neither the true depth of invasion nor surgical margins could be assessed. The resection margins were microscopically positive in 4 cases (10%), of which 3 had adenoma in the final pathology and needed no further intervention, and only 1 had carcinoma in the final pathology that required completion anterior resection.
Pathology
Mid-term oncological follow-up
The mean postoperative follow-up time was 26 month during which 7 patients had local recurrence and 2 patients developed distant metastasis. Three patients were lost to follow-up. Among the 7 patients who encountered local recurrence, 4 were benign and only 3 patients had carcinoma. Thus, with regard only to oncological cases, the local recurrence rate was 21.4% and distal recurrence rate was 14.2%. Of those 3 with carcinoma local recurrence; 1 had T1 lesion with relatively close (0.1 cm) but negative resection margins in the operative pathology and stayed in follow-up until the recurrence 9 month later when she underwent completion abdominoperineal resection (APR). The second patient had T1 lesion with perineural invasion and negative margins on the operative pathology and was treated with adjuvant radiotherapy after the TAMIS procedure due to her preference and refusal for the suggested completion surgery. She was lost to follow-up for a couple of years, after which local and distal recurrences were found and were treated with chemotherapy. The third patient had T3 lesion with negative margins on the operative pathology. He also refused completion surgery after the TAMIS procedure and was treated with adjuvant radiotherapy with the recurrence 10 month later when he refused any treatment. It is interesting to mention that one of the patients with the benign lesion recurrence had actually suffered from local recurrence twice; after the first TAMIS with HGD on pathology he had recurrence and undergone another TAMIS procedure with LGD on the pathology. After his second recurrence he was referred to low anterior resection (LAR) and unfortunately died in the postoperative period from cardiac complications. Another patient with benign lesion recurrence had TMAIS procedure twice due to the recurrence. The disease-free survival rate was 85.4%, during a median follow-up of 26 months (Fig. 1).
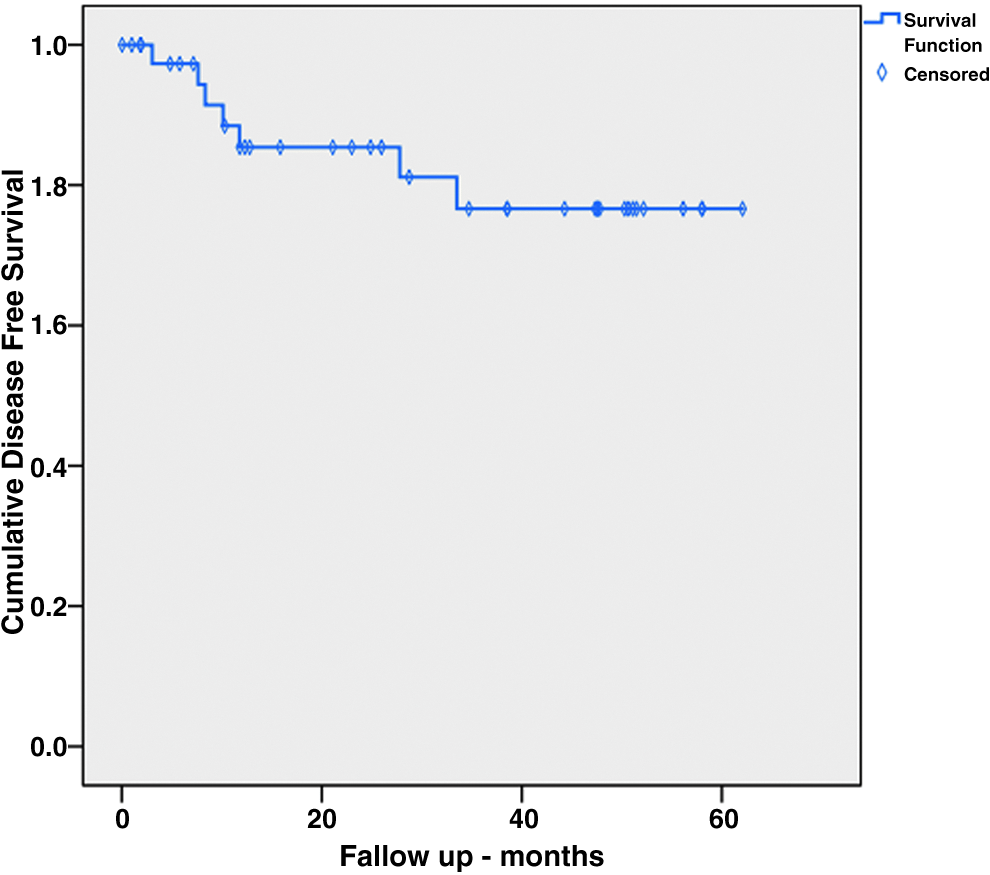
Kaplan–Meier local disease-free survival for patients undergoing curative-intent TAMIS procedure for malignant lesions of the rectum. TAMIS, transanal minimally invasive surgery.
Discussion and Conclusions
The TAMIS is a relatively new advanced videoscopic platform for resection of rectal lesions in the proximal and mid-rectum. As shown in several series, it is a feasible low-cost alternative to TEM.24–28 It can be easily learned by surgeons due to its potential instrumental simplicity and similarity with conventional laparoscopic surgery, making local resection more accessible to allow more patients to benefit from a minimally invasive approach.
The TAMIS procedure is used nowadays for treatment of benign lesion as well as early-stage malignant lesions (uTis or uT1 uN0 M0 cancer) with favorable pathology. Local excision of early-stage rectal cancer is appealing due to lower rates of morbidity and postoperative mortality compared with major rectal resections, although there is always the major concern of leaving metastatic lymph nodes after the procedure, which can lead to recurrent disease. Some studies on locoregional treatment of early rectal cancer have shown satisfactory results with regard to tumor control, supporting the use of TAMIS procedure in those cases.29–31 In contrast, in locally advanced tumors, TAMIS procedure should not be considered as an alternative to standard oncological resection (LAR versus APR), with the exception of morbid patients who are unfit for major surgery or as palliation for metastatic patients. This emphasizes the need for proper patient selection and postoperative surveillance when using the TAMIS platform.
A major risk factor for recurrence of rectal lesions is an R1 resection. 32 One of the advantages of the TAMIS platform is enabling high-quality resection for higher lesions, with lower rate of positive margins and lesion fragmentation rate. In our study the average lesion height was 8 cm from the anal verge, which is comparable with the reported literature. 33 We had only 1 oncological case that had positive margins in the final pathology (2.4%) and a total fragmentation rate of 10%. A systematic review evaluating 390 TAMIS procedures worldwide along 4 years found the rates of positive margins to be 4.36%, tumor fragmentation rate was 4.1%, with an average lesion size of 3.0 cm and the mean distance from the anal verge of 7.6 cm. In that review the overall complications were 7.4%.33,34 In a large series that assessed the perioperative complications and long-term functional outcomes in 75 patients who underwent TAMIS for benign lesions and low-risk cancers, the intraoperative complication rate was 8%, and the postoperative morbidity was 19%. 35 In our study, the 30 days postoperative complication rate was 19.5%, of which only 1 case was considered a major complication. We had no intraoperative complications and only 1 case (2.5%) of penetration into the peritoneal space during the resection, which was resolved without the need of laparotomy or stoma. It should be mentioned that we had a total peritoneal entry incidence of 2 (5%), of which one was diagnosed during the operation and the other one during the postoperative period. The incidence of peritoneal entry has been reported between 0% and 9.7% in the literature31,35,36 with increased incidence noted for proximal, anterior, and near-circumferential lesions.37,38 Of the 2 cases in which we had peritoneal violation, one lesion was located anteriorly at 7 cm height from anal verge and the other one was located on the left posterior wall, but was relatively high at 12 cm from the anal verge.
This low complication rate is one of the advantages TAMIS offers over radical resections for rectal lesions, 39 as does shorter hospitalization length. The average length of stay of our patients was 2.6 days (range 1–7, SD 1.4).
With a median follow-up time of 26 months, the local recurrence rate of our oncological cases was 21.4% (n = 3). Several studies have shown that the postoperative local recurrence rate after local excision for pT1 rectal cancer is in the range of 4%–24%, whereas the local recurrence after radical surgery is in the range of 0%–7%.40,41 It is important to mention that in 2 of our 3 cases with local recurrence, the patients were offered completion surgery after the TAMIS procedure, due to high-risk pathological features, to which they both refused. One could argue that had they been operated as recommended the recurrence might have been prevented.
The TAMIS procedure can be a curative procedure but can also be considered as “excisional biopsy,” especially in oncological cases, allowing definitive T-stage and depending on the operative pathology a decision can be made regarding further intervention needed. This is important to acknowledge especially in light of the fact that preoperative biopsy offers a low accuracy, with a histological discrepancy of up to 20% or even higher. 42
It is accepted that local excision might be offered to patients with high-risk T1 or T2–T3 tumors with poor life expectancy and multiple comorbidities, which are unfit for major surgery, offering a reasonable chance of success. In this group, adjuvant radiotherapy could be an option for selected patients who decline completion surgery or are too frail for radical surgery, but even though radiotherapy appears to have some benefits added to local excision, it is still not as effective as radical surgery. 39
All patients after TAMIS procedure are assigned to close follow-up with frequent endoscopies, which may allow early recognition of recurrences and the opportunity for further intervention as needed. Unfortunately, several studies have shown disappointing results in cases of salvage resection for recurrence after local resection with poor oncological outcomes.43–46 This emphasizes the importance of appropriate patient and tumor selection for TAMIS, and that accurate staging is of paramount importance for decision-making.
It should be mentioned that in only 14 cases of our study the indication for surgery was malignant lesion, making a relatively small sample size for oncological conclusions. In the study we had a relative long follow-up period with an average >2 years (mean 26 months), during which we collected a detailed database with many variables, but since this is a retrospective study we were limited to data available on the medical records. We calculated the survival depending on the last recorded hospital visit (at any department), but as during the follow-up period we had not encountered any disease-related death, we could calculate only the disease-free survival, which was 85.4%. In addition, although all procedures in the study took place in a single medical institute, they were done by 5 different colorectal surgeons.
In conclusion, TAMIS is an acceptable and feasible procedure for carefully selected patient with benign and early-stage malignant lesions of the proximal and mid-rectum who meet the specific criteria. It offers an easier recovery in comparison with radical surgery, with shorter hospitalization, lower complication rate, and significantly better quality of life. When it is utilized for early-stage rectal cancers, high-risk pathological features should prompt a completion proctectomy. It cannot be overemphasized that patient selection is paramount for good oncological results, although further studies with larger patient sample and longer follow-up may be needed for better conclusions regarding oncological results.
Footnotes
Disclosure Statement
No competing financial interests exist.