
Abstract
Introduction:
One-stage anorectoplasty provides maximum potential for “normal” defecation reflexes right at birth and avoids complications and problems of colostomy. One-stage laparoscopic anorectoplasty (OSLARP) for rectourinary fistula (RUF) is restricted by distended bowel obscuring the working space for laparoscopy. This study describes transperineal intracath meconiolysis and evacuation (TIME) technique for OSLARP in the treatment of RUF in neonates.
Materials and Technique:
High male anorectal malformation (ARM) admitted from January 2016 to March 2019 were included in the study. Diagnosis of level of ARM was made on the basis of invertogram. Patient presenting with lethal comorbidities were excluded who underwent colostomy. The technique involved placement of a 16G intracath in the perineum through the site of future neo-anus, which was identified using muscle stimulator. Meconiolysis and evacuation was done using warm saline and 2% N-acetyl. The creation of enough abdominal space was achieved after evacuation and two working instruments were placed in paraumbilical positions. The laparoscopic dissection and division of fistula was done as followed in standard laparoscopic anorectoplasty.
Results:
Seventeen patients were selected for TIME technique but on laparoscopy 2 patients had severe necrotizing enterocolitis hence they underwent laparoscopy-assisted high sigmoid colostomy. Fifteen patients underwent OSLARP successfully. Mean weight was 2.5 ± 0.4 kg, mean gestational age was 36 ± 5 weeks, and mean age of presentation was 3.5 ± 1 days after birth. The TIME technique was successful decompressing bowel in all the patients. Out of 15 patients of OSLARP, 14 had rectoprostatic urethral fistula and 1 had rectovesical fistula. Mean total operative duration of OSLARP was 46 ± 15 minutes. Patients who could be followed for 3 years had good results in terms of continence and bowel movements.
Discussion:
TIME technique is a very simple and effective way to overcome the problem of associated colonic distention in neonatal one-stage laparoscopic anoplasty.
Introduction
Rectourinary fistula (RUF) is the commonest type of anorectal malformations (ARMs) found in boys. 1 The RUF is classified into rectovesical fistula, rectourethral prostatic fistula, and rectourethral bulbar fistula. 2 A conventional laparoscopic anorectoplasty is becoming popular for the treatment of RUF due to its advantages and is done as a staged procedure after a neonatal colostomy. 3 The problems of repeated anesthesia, surgeries, need of colostomy, and its associated problems are major drawbacks of staged procedure. One-stage posterior sagittal anorectoplasty (PSARP) provides restoration of anorectal continuity and maximum potential for “normal” defecation reflexes right at birth. 4 However, one-stage laparoscopic anorectoplasty (OSLARP) for RUF is limited by distended bowel filled with meconium and air obscuring the working space for laparoscopy and, therefore, it has not become as popular as its open counterpart. 5 This study describes transperineal intracath meconiolysis and evacuation (TIME) technique for OSLARP in the treatment of RUF in neonates.
Materials and Methods
It is a prospective study, including high male ARM admitted from January 2016 to March 2019. Diagnosis of level of ARM was made on the basis of invertogram. The chest X-ray, spine X-ray, abdominal ultrasonography, voiding cystourethrography, and echocardiography were used to assess the patients' preoperatively. Low malformation (treated with cutback anoplasty), intermediate malformation with rectobulbar fistula (managed with one-stage limited PSARP) and congenital pouch colon (managed with pouch excision and stoma) were excluded from the study. Patient presenting with septicemia, disseminated intravascular coagulopathy, cyanotic heart disease, perforation and associated tracheoesophageal fistula were excluded from the study, all of which underwent colostomy. The finding of necrotizing enterocolitis on laparoscopy was considered as exclusion for OSLARP and laparoscopy-assisted high-sigmoid colostomy was performed. Confirmation of level of fistula was done on the basis of laparoscopy findings in the patients undergoing OSLARP. Ethics committee approval from the institute and written informed consents were obtained before the surgery. All patients were operated at one center by the same pediatric surgeon having experience of >15 years. Complications were assessed in terms of anal surgical site infection, port site infection, anal stenosis, mucosal prolapse, and residual diverticulum (which were assessed using 2-monthly ultrasound and a voiding cystourethrography if needed) till 6 months of age. Krickenbeck classification of postoperative results was used to assess functional outcome and patients were followed up for a minimum of 3 years, which is considered as minimum age of verbal assessment according to Krickenbeck classification.
Technique
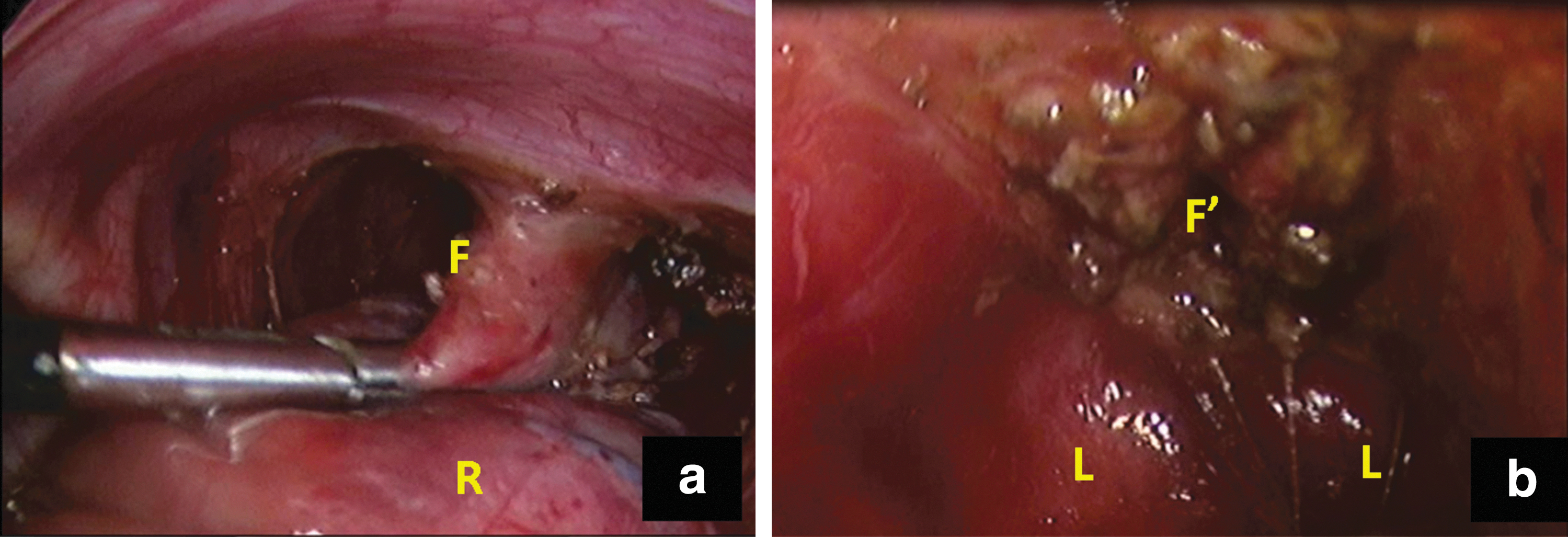
Under general anesthesia and supine-lithotomy position, a 5 mm umbilical optical port was placed by open technique avoiding division of umbilical ligament that are vascular in neonates. The dilated colon and rectum obscured the view universally in all patients, so TIME technique was adopted to decompress the colon before placement of working instruments. The TIME technique involved placement of a 16G intracath in the perineum through the site of future neo-anus, which was identified using percutaneous muscle stimulator (Fig. 1). The needle with the plastic sheath was directed upward along the curve of pelvis and inserted completely. The needle was withdrawn out of canula and free aspiration of air with meconium stain confirmed the placement of canula into the rectum. The decompression of rectum on laparoscopic view confirmed the proper placement of intracath (Fig. 2a, b). Meconiolysis was done using warm saline by repeated instillation and aspiration. Meconium was evacuated with 20 mL syringe to achieve adequate negative pressure to aspirate liquefied but thick meconium. In condition of thick meconium that was not aspirable with saline meconiolysis, the meconiolysis was done using 2% N-acetyl cysteine (Mucomix®; Samarth life sciences) with a holding period of 5 minutes. The creation of enough abdominal space was achieved after evacuation and two working instruments were placed in paraumbilical positions. The use of graspers allowed compression and evacuation of gases toward rectum, which was again aspirated by the TIME technique to achieve maximum working space. Complete laparoscopic examination of colon and ileum was done to rule out necrotizing enterocolitis. The laparoscopic dissection and division of fistula was done as followed in standard laparoscopic anorectoplasty (Fig. 3a, b). After dissection of rectum, the intracath canula was removed and dissection of fistula was completed. To achieve adequate mobilization, division of superior rectal artery was done and marginal arcade was preserved. The level of fistula was confirmed with laparoscopy finding of level of rectal tapering and junction of lower end of rectum. The rectum ending at bladder was labeled as rectovesical fistula and rectum ending at prostatic urethra was labeled as rectoprostatic fistula. The rectum tapering and the fistula opening was divided close to the urethra and transfixed if a wide fistula is found. Incision was given at the site of proposed neo-anus that has been identified by muscle stimulator and anorectoplasty was completed. Port sites were closed.

Showing perineal insertion of 16G intracath for meconiolysis and evacuation of distended bowel.

In the postoperative period, oral feeds were allowed in gradual manner after resumption of bowel movements. Postoperative oral acetaminophen was used thrice a day for analgesia. The wound was taken care by cleaning of fecal matter, local nursing, and local neomycin–bacitracin–polymyxin ointment (Neosporin®; Johnson and Johnson Limited).
Results
Between January 2016 and December 2018, 80 male newborns with ARM were admitted and the distribution of types of ARM and the procedure done for correction is shown in Figure 4. Patients underwent colostomy when they were associated with comorbidities such as septicemia, disseminated intravascular coagulopathy, cyanotic heart disease, perforation, and tracheoesophageal fistula. Seventeen patients were selected for TIME technique but on laparoscopy 2 patients had severe necrotizing enterocolitis hence they underwent laparoscopy-assisted high sigmoid colostomy. Fifteen patients underwent OSLARP successfully. Mean weight was 2.5 ± 0.4 kg, mean gestational age was 36 ± 5 weeks, and mean age of presentation was 3.5 ± 1 days after birth. The TIME technique was successful decompressing bowel in all the patients. Out of 15 patients of OSLARP, 14 had rectoprostatic urethral fistula and 1 had rectovesical fistula. Mean total operative duration of OSLARP was 46 ± 15 minutes, including the time required for evacuation, and mean duration of TIME process was 8 ± 3 minutes. Mean follow-up period was 38 ± 3 months. Intraoperative blood loss was insignificant and none of the patient needed a blood transfusion. There was no injury to vessel, ureter, urethra, or vas deferens in any of the patient. The complications included 2 (13.33%) cases of anal site infection responding to local and oral antibiotics, 1 (6.66%) case of port site infection responding to local and oral antibiotics, 1 (6.66%) anal stenosis responding to dilatation, and 1 (6.66%) case of mucosal prolapse responding to sodium tetradecyl sulfate injection. The results in terms of continence could be evaluated in 5 patients who crossed 3 years age, which was considered as minimum age for verbal assessment of continence and result is shown in Table 1. Most of the patients had good results in terms of continence and bowel movements.
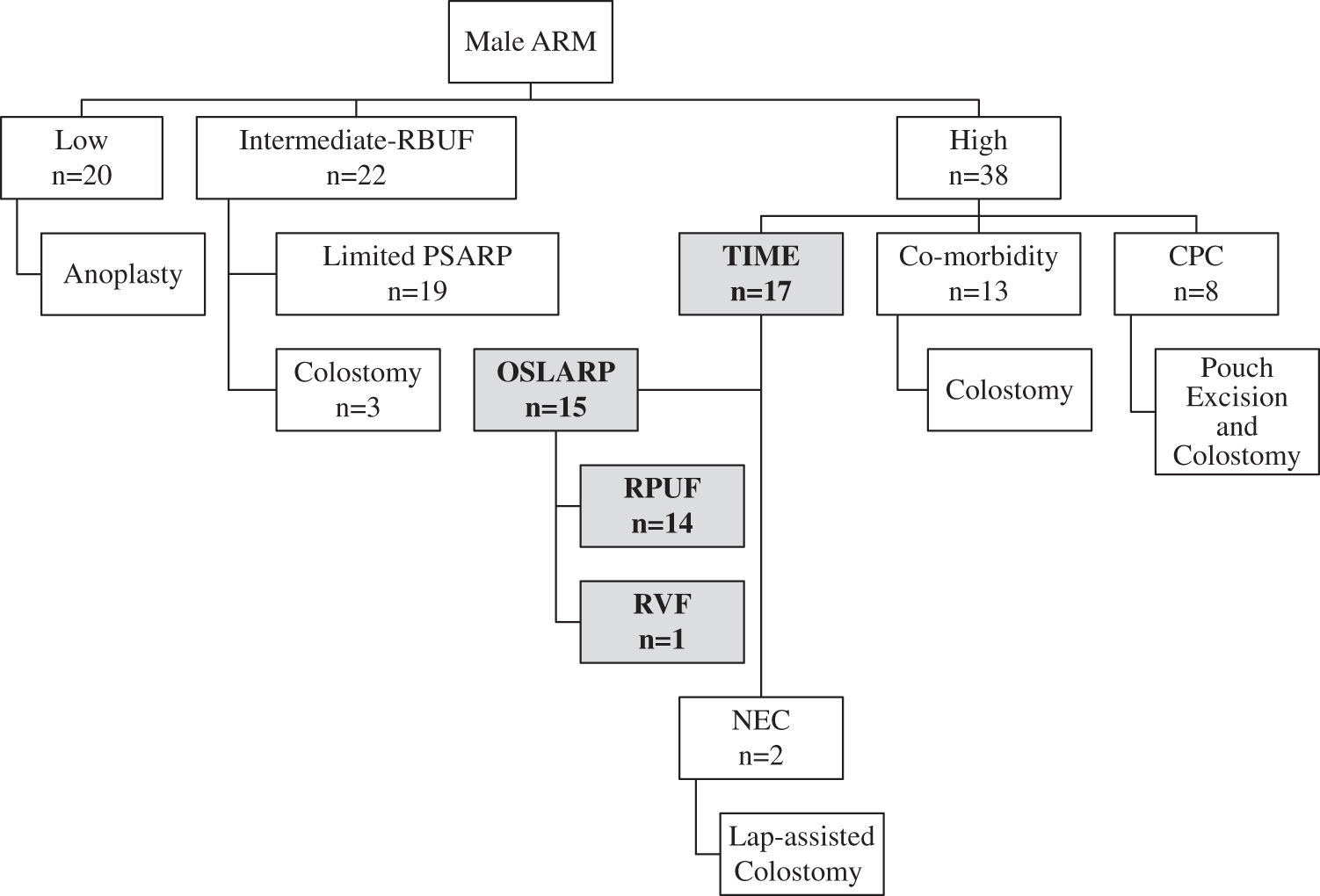
Flow diagram showing distribution of types of anorectal malformations and the correction offered. CPC, congenital pouch colon; NEC, necrotizing enterocolitis; PSARP, posterior sagittal anorectoplasty; RBUF, rectobulbar urethral fistula; RPUF, rectoprostatic urethral fistula; RVF, rectovesical fistula.
Assessment of Postoperative Results Based on Krickenbeck Classification (n = 5)
Discussion
Definitive “at birth” one-stage surgical correction of boys with ARM and RUF has the advantage of medical, psychological, social, and economic benefits to the patient. 4 Brain-defecation reflex gets initiated at birth and the existing neuronal network undergoes early development of neurons and their circuits and timely training of pelvic musculature, which collectively improves the results in terms of continence.4,6 Moreover, one-stage anorectoplasty avoids repeated anesthesia, surgeries, and morbidities associated with colostomy. The complication of colostomy includes excoriations, dehydration, prolapse, retraction, and adhesions in 32%–40% patients. 7 The complications of colostomy include obstruction, leak, stricture and incisional hernia in as much as 1.5%–55% patients.8–10 The burden of stoma care, repeated admission for dehydration, and subsequent psychosocial burden to the family should not be underestimated. Repeated surgery and multiple scars also lead to personality disorders. 11 There is lack of high-level evidence that can suggest that neonatal one-stage correction of male ARM is comparable with staged correction. The debate does surround its feasibility, technical nuances, experience, learning curve, complications, and long-term outcome. However, there are many reports on one-stage PSARP to treat the neonates with ARMs and results are comparable with three-stage procedure.12–14 The technique of laparoscopic surgery has the advantages of magnification, minimal surgical trauma, early recovery, precise identification of the anatomical structures, and placement of rectum within the muscle complex. 3 The conventional laparoscopic-assisted anorectoplasty (LAARP) consists of three stages of colostomy, LAARP, and colostomy closure. But, the biggest obstacle to OSLARP is the inability to operate in a restricted working space because of distended bowel in a small pelvic cavity. Therefore, the challenge remains of decompressing the meconium and air from the bowel with avoidance of spillage in to peritoneal cavity. Many pediatric surgeons reported the technique of OSLARP for high imperforate anus.15,16 Vick et al. recommended one-stage laparoscopic anorectoplasty to utilize advantage of early correction of ARM, but recommended surgery within 48 hours and required high operative duration due to distended bowel hindering the space. 15 The tertiary centers often encounter the cases of ARM that are noticed and referred late presenting with severe abdominal distention as found in this study where mean age of presentation was 3.5 ± 1 days and thus colonic distention precludes OSLARP. To overcome colonic distention, Li et al. used enema through a urethral catheter inserted into the distal rectum through the fistula using a cystoscope and decompression by abdominal needle aspiration from the distal rectal pouch under laparoscopic guidance. 16 This is associated with ineffective evacuation, peritoneal spillage due to transabdominal puncturing of rectum and consumption of lot of time. To overcome the maiden problem of distended bowel, Diao et al. used a right semicircular umbilical incision of size 2.5–3 cm to deliver sigmoid colon through the umbilicus and a colotomy to deflate the colon along with multiple needle aspiration of the distended small intestine.5,17 This technique has the disadvantage of unwarranted colotomy, wound contamination, needle injury to small bowel, and risk of leak in postoperative period.
TIME technique allows intraoperative decompression of meconium without a colostomy, prevents pelvic meconium contamination, creates good working space, and provides adequate exposure. As bowel evacuation is near complete, there is early return to bowel function, no postoperative distention, and minimization of infection. The use of N-acetyl-cysteine facilitates meconiolysis in cases where meconium is thick and sticky. 18 The operative duration is reduced remarkably as this is a very handy procedure that took 46 ± 15 minutes in this study; in comparison with 2.5–3.25 hours in study without evacuation. 6 The placement of 16G intracath was unguided in this study but did not require more than one attempt in any of our patients because the rectal pouch is severely dilated in cases presenting late. The cases presenting early without remarkable distention may be handled without evacuation as suggested by Vick et al. and TIME may not be needed. Further research may be done using ultrasound guidance to place the intracath, but ultrasound in neonates with ARM is associated with poor accuracy. 19
Surgical heuristics is in vogue where the observer uses a simple tool to overcome a big problem based on an ordinary observation and introspection. 20 TIME technique is one of the heuristic approaches, which involves tinkering with the procedure to develop a new step to make the procedure feasible and easy.
TIME technique is a very simple, easy, practical, and effective way to overcome the problem of associated colonic distention while performing one-stage laparoscopic anoplasty in male ARM.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information to disclose.