
Abstract
Background:
Median arcuate ligament (MAL) syndrome is a rare cause of chronic abdominal pain in adults and children. Release of the MAL has traditionally been performed open or laparoscopically. There have not been any published cases to our knowledge of robotic-assisted MAL release in pediatric patients.
Patients and Methods:
Two adolescent patients, aged 12 and 15 years, at our institution underwent robotic-assisted MAL release. The procedure involved dissecting the MAL muscle fibers and overlying scar tissue. Patients stayed inpatient postoperatively overnight and with an average outpatient follow-up of 10 months.
Results:
Both patients had immediate pain relief postoperatively and at 10-month follow-up had no recurrent symptoms. No complications were associated with the procedure.
Conclusion:
The increasing role of robotic surgery as a new surgical technique is gaining momentum for many procedures. This new approach for MAL release in the pediatric population was explored by our institution. It was found to be successful, safe, and reproducible for future patients.
Introduction
Chronic abdominal pain in the pediatric population is common and often associated with psychological diagnosis and sequela. 1 Median arcuate ligament syndrome (MALS) is a known cause of chronic abdominal pain seen in both adults and pediatric populations and is frequently overlooked due to its rarity and overlapping symptoms with many other causes of chronic abdominal pain. 2 MALS, defined as postprandial pain, nausea, emesis, and weight loss, is a clinical entity that involves compression of the celiac artery and celiac nervous plexus by the median arcuate ligament (MAL). Described initially by Harjola in 1963, 3 understanding of the syndrome has improved with many new diagnostic and corrective surgical techniques tested for the past few decades.4–6
The exact pathophysiology of the symptoms caused by MALS is not fully understood. The syndrome has been attributed to celiac artery compression by the MAL, resulting in reduced circulation and ischemic symptoms.4,5 However, compression of the celiac artery may not always be symptomatic and may be a normal anatomic variation. Research has shown that 7%–21% of individuals have compression of the celiac artery with no symptoms.7–9 In addition, studies have also shown that revascularization of the celiac artery is not necessary for symptomatic relief 6 and that residual celiac compression after surgery was not associated with recurrent symptoms. 10 This suggests that the etiology of the syndrome may not be entirely vascular and other factors may be contributing to the pathophysiology of MALS. Chronic compression of the celiac plexus and inflammation of the nerve fibers have been suggested as alternative etiology of MALS. 11
The clinical diagnosis of MALS is usually made after a thorough evaluation for chronic abdominal pain without demonstrable pathology found. MALS is thought to be a cause of chronic functional abdominal pain in the pediatric population and diagnosis is facilitated by imaging. 12 After diagnosis, the mainstay of therapy is MAL release. 13 Although this procedure has been done robotically in the adult population 14 to our knowledge, there are no cases published of robotically assisted MAL release in the pediatric population.
Patients and Methods
Two patients received robotic-assisted MAL release at a stand-alone children's hospital in July and August 2018. Both patients reported symptoms of intractable abdominal pain and had been diagnosed by pediatric gastroenterologists with chronic abdominal pain after completing trials of conservative treatments without resolution of pain.
Both patients received an extensive diagnostic workup, including computed tomography (CT) angiography and dynamic Doppler ultrasound (US) of the abdominal aorta and celiac artery trunk with inspiration and expiration.
The first patient, a 12-year-old male with chronic abdominal pain and unintentional weight loss, received a CT scan and then was finally diagnosed with MALS after a magnetic resonance (MR) angiogram (Fig. 1a, b); diagnosis was confirmed with Doppler US with inspiratory and expiratory phase US (Fig. 1c–f).
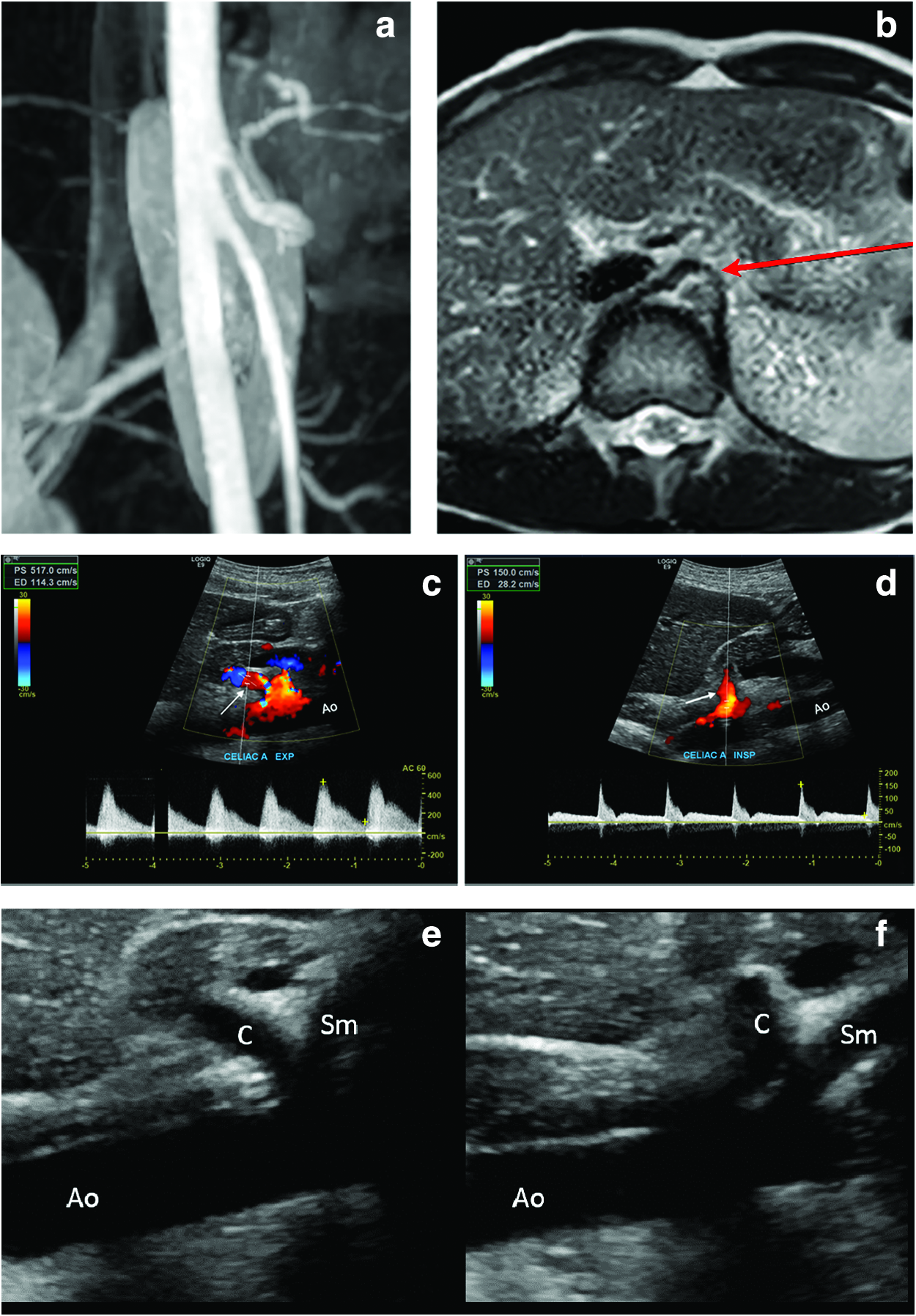
Imaging for diagnostic workup in first patient, a 12-year-old male MR angiogram of the abdominal aorta.
The second patient, a 15-year-old female with chronic abdominal pain and unintentional weight loss, first received a CT angiography of the abdominal aorta (Fig. 2a–c). Diagnosis was confirmed with Doppler US showing peak flow during inspiration and expiration (Fig. 2d, e). The diagnostic criteria for MALS in these patients included a clinical diagnosis of symptoms—abdominal pain, vomiting, weight loss as well as demonstration on Doppler US showing peak flow velocity of the celiac during expiration >200 cm/s, celiac/aorta peak systolic velocity ratio >3, and an angle of deflection of the celiac artery >50%. These diagnostic criteria can be seen in Table 1. Both patients were diagnosed using both clinical and US diagnostic criteria and additionally had other imaging performed for better view of the anatomy before operating.
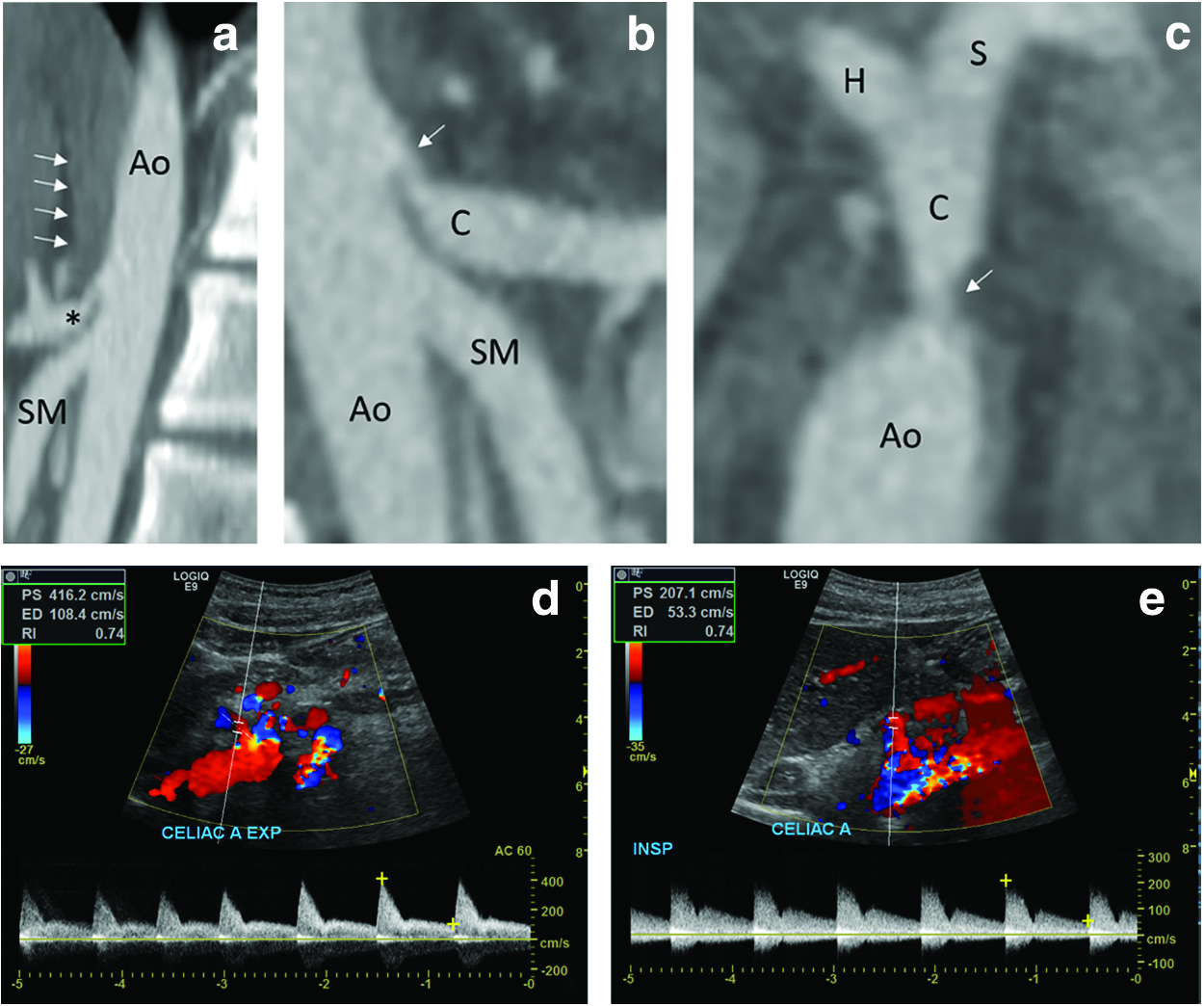
Imaging for diagnostic workup in second patient—15-year-old female patient. CT angiography of the abdominal aorta:
Ultrasound Criteria for Median Arcuate Ligament Syndrome
PSV, peak systolic velocity.
After diagnosis, both patients underwent scheduled robotic MAL release by the same surgeon at our institution. The da Vinci Xi© robotic system was used for the procedure. Clinical follow-up without any imaging after surgery was done to assess reduction in pain and improvement of symptoms. Patients are still being followed.
Description of technique
The patient is placed supine on the operating table. Infraumbilical 8 mm trocar is inserted in the abdomen and the abdomen is insufflated. Once pneumoperitoneum is achieved, the camera is inserted for visualization. A 5 mm incision is made in the subxiphoid area and a liver retractor is placed to retract the liver superiorly. Three more 8 mm robotic ports are placed along the mid abdomen under direct visualization, two to the left of the umbilicus and one to the right of the umbilicus, all parallel to the umbilicus. The patient is placed in a steep Trendelenburg position. Then, the robot is docked to the camera port and the three remaining ports.
Once the robot is docked, the procedure is initiated by opening the pars flaccida with hook cautery to expose and identify the right crus of the diaphragm. Dissection is performed using electrocautery across the retroesophageal window in between the right and left crus, carrying the dissection down to the confluence of the left and right crus to expose the aorta. To perform dissection over chronic scarring of muscular fibers, hook cautery is used. When encountering vessels during dissection, a robotic vessel sealer is used. Once the aorta is exposed, the celiac trunk is identified and noted to be compressed. The dissection was carried out to release the compression and it was completed when the bifurcation of the left gastric and common hepatic arteries was reached. The arteries are examined for damage and the area is examined for hemostasis.
The two leaflets of the crus are loosely approximated. The port sites are removed under direct visualization and the liver retractor is removed. Fascial sutures are places at all the port sites.
Results
Both surgeries had no intraoperative or postoperative complications. Blood loss was estimated as <5 mL in each patient. In both patients, chronic scarring was identified with visualization from the robot and taken down during dissection. The operative time, including docking time, console time, and full operation length of time, is shown in Table 2. Both cases took <3 hours and time to dock the robot was <10 minutes of the total case time. Both patients stayed postoperatively overnight. The first patient required more acetaminophen for postoperative pain and stayed an additional day until postoperative day 3. The second patient was discharged on postoperative day 2. Both patients reported resolution of their symptoms upon discharge. There were no complications postoperatively for either case. At clinical 10-month follow-up, both patients continue to report resolution of abdominal pain and vomiting, and have returned to normal body weight.
Operative Time for Robotic Cases, Including Total Operative Time, Docking Time, and Console Time
Discussion
MALS is a disease that affects patients in both the adult and pediatric populations. Although the syndrome is a rare clinical diagnosis, studies have been done regarding various methods of diagnosis and treatment of MALS. However, due to its rarity, it is difficult to perform large studies on diagnosing and treatment and there is yet to be a gold standard imaging or surgery for diagnosis and treatment.
Multiple imaging modalities can be utilized to diagnose MALS. Normally, the MAL, a fibrous band that joins the diaphragmatic crura, passes over the aorta just superior to the celiac trunk. 15 In MALS the ligament crosses over and impinges on the origin of the celiac trunk. Compression of the celiac trunk increases with expiration and decreases in inspiration. 16
US is an excellent first-line screening modality useful in delineating the celiac trunk as it uses no radiation and the application of Doppler can detect alterations in celiac artery systolic velocity. The ability to evaluate the celiac vessel in real time allows dynamic interrogation of the vessel with inspiration and expiration.17,18 The easy availability of US also allows for postsurgical follow-up. US criteria of stenosis such as an elevated peak systolic velocity >200 cm/s, celiac aorta peak systolic ratio >3, and flow turbulence and celiac artery angel of deflection of >50% are indicative of MALS when associated with clinical symptoms.19,20
CT angiography and MR angiography are useful to delineate more accurately celiac trunk narrowing and identify other secondary causes of compression, collaterals, or aberrant vasculature. The typical narrowing just distal to the celiac origin caused by compression creates a “J” shape or hooked configuration that can be reconstructed on CT angiography 3D volume rendered and maximum intensity images to assess the degree of narrowing and poststenotic dilatation. 21 Imaging should be performed in inspiration and expiration during the same contrast injection to best assess dynamic changes in caliber of the celiac trunk with only a momentary pause between respiratory phases.16,21,22 Patient cooperation is needed for the aforementioned protocol, which may be difficult to obtain in pediatrics, in addition to the concerns with the increased radiation exposure with CT.
The mainstay of therapy is surgical release of the MAL. The surgeries were originally completed open and now are more commonly performed laparoscopically. The laparoscopic technique was first described in the literature in a case report by Roayaie et al. in 2000. In 2012, a meta-analysis revealed that open and laparoscopic techniques led to similar outcomes and symptomatic relief 6 in the pediatric population, laparoscopic MAL release has been shown to be safe, improving celiac trunk blood flow, resolving symptoms, and improving psychosocial quality of life in symptomatic patients.12,23
Although there is no reported use in the literature of robotic-assisted MAL release in the pediatric population, MAL release in the adult population are now often performed robotically. The first robotic-assisted laparoscopic approach for MAL release was reported in 2007 and concluded improved optical enhancement, improved dexterity, and enhanced microdissection. 24 Although many institutions are performing MAL releases robotically, only institutional studies are currently in the literature. One study demonstrated robotic techniques that allowed shorter hospital stays and reduced estimated blood loss. 14 Another small institutional study comparing laparoscopic and robotic approaches in 16 patients—12 undergoing laparoscopic release and 4 robotic—showed no differences in hospital stay, clinical improvement, or symptoms or complication rate but longer operative time (101.7 laparoscopic versus 145.8 robotic minutes). 25 However, a more recent institutional study contrasting robotic and laparoscopic approach from 1999 to 2018—16 laparoscopic and 18 robotic cases—showed similar complication rates and clinical improvement, but shorter operative times with the robot (179.5 laparoscopic versus 106 robotic minutes). 26 This suggests that operative times with the robot may be institution and surgeon dependent due to differences in familiarity of the surgeon and other operating room staff with using it. However, these small studies suggest that the robotic approach is equivalent or potentially superior to the laparoscopic approach for a MAL release in the adult population. Further studies are necessary on a wider level to evaluate the robotic approach to MAL release. In addition, with successful reports of use of the robot in the adult population, the robotic-assisted MAL release needs to be explored within the pediatric population as well.
Conclusion
MALS is a relatively rare disease, but those affected suffer greatly from chronic abdominal pain and associated psychosocial comorbidities. Laparoscopic MAL release has been shown to be effective in pediatric patients for symptoms resolution and improved quality of life for the child and their parents.12,23 There is no current literature regarding robotic MAL release in the pediatric population.
Robotic technique in the pediatric population is largely used for urological, hepatobiliary, and cardiothoracic surgeries with some case reports for other procedures. 27 The emergence of robotics in children has been slow due to inherent technical difficulty in small children with small work space as well as the increased expense. Use of the da Vinci robot is expanding as availability in hospital centers increases. Although many pediatric hospital centers have access to a robot, a recent survey of pediatric surgery fellowships in the United States has shown limited use in pediatric procedures and deficiencies in robotic training. 28 However, given the success of robotic MAL release in the adult population, performance in the pediatric population also needs to be further studied. Owing to the importance of a careful and complete dissection,11,14 the extra dexterity from the robotic approach compared with laparoscopic approach supports the use of the robot. Immediately after and up to 10-month follow-up, our patients reported complete resolution of their symptoms. Our institution provides information about this approach in 2 patients and invites more studies on the use of robotic MAL release in the pediatric population.
Footnotes
Acknowledgments
We thank Nicklaus Children's Hospital for providing the patients and resources used for this article.
Disclosure Statement
B.R. and R.P. have no competing conflicts of interests. F.A. serves as educator and consultant for Intuitive Surgical.
Funding Information
No funding was recieved for this study.