
Abstract
Robotic surgery through the da Vinci Surgical System has been widely spread for many procedures across the globe for several years. At the same time, robot-assisted gastrectomy for gastric cancer (GC) remains mostly available only in specialized centers in minimally invasive surgery and stomach neoplasm. The robotic platform has been introduced to overcome possible drawbacks of the laparoscopic approach. The safety and the feasibility of robotic radical gastrectomy have been reported in many retrospective case series and nonrandomized prospective studies. However, the superiority of robotic gastrectomy over the laparoscopic access has not yet been proven. This study aimed to report the technical aspects of robot-assisted gastrectomy for GC as well as the latest evidence on this subject.
Introduction
Gastric cancer (GC) is considered a disease of extreme epidemiological relevance, as it is the fifth most prevalent malignant disease and the third leading cause of death due to malignant disease. 1 The main method of treatment is tumor-free margin resection associated with D2 lymphadenectomy. Early diagnosis may improve curability. Still, in advanced cases and with no prospect of cure, surgery plays an important role in treating any possible complications, such as bleeding, obstruction, or perforation of the stomach. 2
Thus, the use of technology has proven useful in the attempt to perform less traumatic procedures, with better postoperative recovery and more adequate oncological results. Along these lines, minimally invasive surgery in GC surgery has grown exponentially in the last decade. Several trials have reported the safety and effectiveness of the laparoscopic approach.3–5 Despite the benefit to the patient obtained through laparoscopic surgery, it is known that this access often causes greater fatigue and more physical effort of the medical staff, as well as other inconveniences, such as the two-dimensional vision. In this sense, robotic surgery for GC was introduced by Hashizume et al in 2003 with the goal to overcome possible intrinsic disadvantages of conventional laparoscopic gastrectomy (LG). 6 Robotic platform provides better visualization with three-dimensional (3D) high-resolution magnification imaging. Still, it assists surgeons in performing more accurate tissue dissection due to tremor filtering and the EndoWrist functions.
Recent publications have shown that minimally invasive gastrectomy with lymphadenectomy, either laparoscopic or robotic, is safe and efficient to treat early GC. It promotes better recovery and long-term results similar to open surgery, despite being one of the most technically difficult procedures among surgeries of the digestive tract.7–9 This study aimed to demonstrate the technical aspects of robot-assisted gastrectomy for GC and its present evidence.
The da Vinci system
In 1995, the Intuitive company was founded with the goal to provide innovation over a super technological human/machine computer interface, which would allow surgeons to overcome possible drawbacks of laparoscopic surgery. The so-called master slave system was developed in the early 90s by NASA (National Aeronautics and Space Administration) and the Stanford Research Institute, in which the operator, located in a workstation, could manipulate objects, viscera, and anatomical structures through robotic arms even at great distances. That was particularly important for working in dangerous areas, such as the battle front or the outer space. The result of this magnificent joint adventure was the creation of the da Vinci Surgical System launched in 1999 and cleared by the FDA (Food and Drug Administration) for general laparoscopic surgery in 2000. Since then, over 5 million surgeries have been performed, more than 40,000 surgeons trained globally, and almost 4500 da Vinci systems used worldwide.
The Da Vinci system is a sophisticated robotic platform that enables the use of articulated instruments through small incisions in the skin and a high-definition 3D video camera, where the surgeon sits comfortably on the console and visualizes magnified images of the surgical field. Using computer technology, the movements of the hands of the surgeon are faithfully reproduced by the arms of the robot in real time (master slave system), through extremely precise and delicate maneuvers obtained by filters that reduce tremors and unintentional movements. The Da Vinci system consists of the console, the cart with all four arms of the robot, a high-performance video structure, and the EndoWrist's patented instruments. A wide variety of devices with different functions are used in various surgical procedures.
Surgical procedure
Robotic gastrectomy (RG) is gaining ground today thanks to Korean studies and experiences. The Yonsei University College of Medicine in Seoul (Korea) is the pioneer in this field. Studies published by Hyung and colleagues have contributed to sharing this technique around the world. The surgical steps and illustrations described below are based on the most present experience in this type of procedure.8,10–15
Initial stage
Positioning of the patient in reverse Trendelenburg by ∼15–30°.
Twelve millimeter trocar (Si) or 8 mm trocar (Xi) placement just below the umbilicus.
Pneumoperitoneum—12 mmHg pressure.
Four trocar placement (1 of 12 mm and 3 of 8 mm), the 1 of 12 mm to the left of the umbilicus used by the assistant for clipping vessels and stapling (Fig. 1).
Trocars 1 and 3 are placed below the costal border anterior to the anterior axillary line. If the hepatic border is located more caudally, the surgeon should attempt to position trocar 3 so that its manipulation is not obstructed by the organ. Trocar 2 is placed midway between the camera and trocar 3. The 12 mm trocar used by the assistant should be positioned equidistant from trocar 1 and the umbilicus and 1 to 2 cm below the virtual line joining them (Fig. 2).
Lifting the liver (Fig. 3).
The liver may be retracted with gauze fixed by suture with a straight needle to the right of the falciform ligament and through the left of lateral segment, this has shown good results. Another option is to use Nathanson liver retractor.
Placement of the “cart” above the patient's head (Si) or to the patient's right lateral side (Xi) (Fig. 4).
Positioning of the robot arms: one for the camera (umbilicus), two for the cadieres, one for the harmonic scalpel to the patient's right, and one for the Maryland on the left.
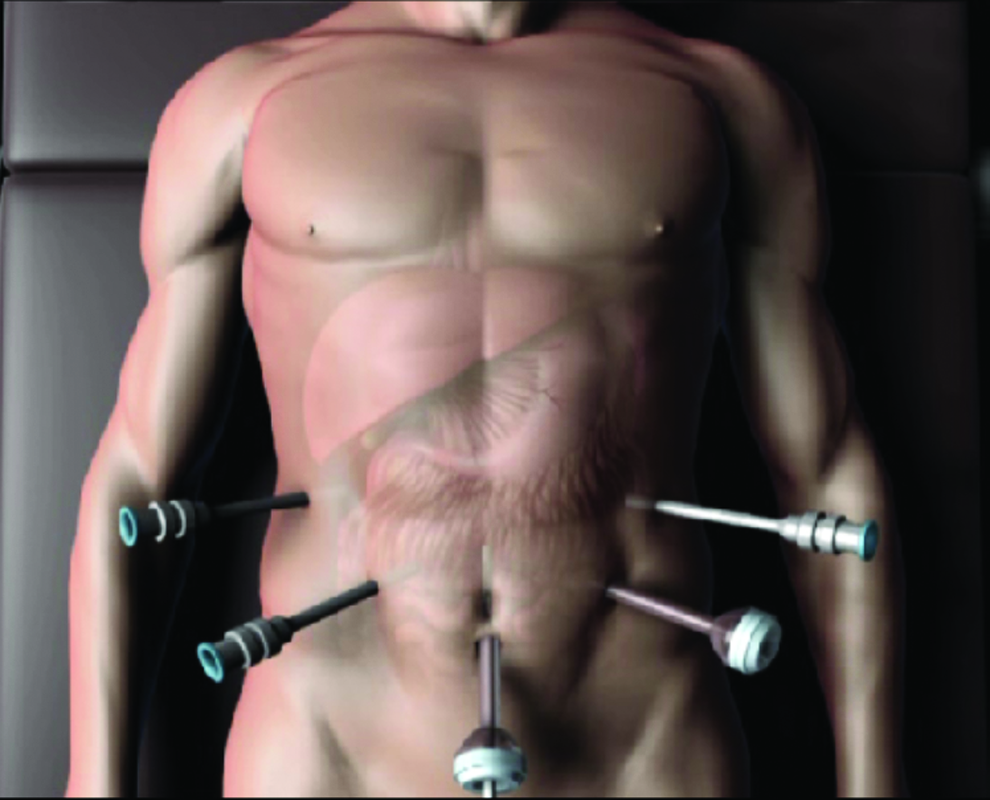
Position of trocars. Illustration: Rodrigo Tonan.

1: Maryland bipolar; 2: harmonic scalpel; 3: cadiere. Illustration: Rodrigo Tonan.

Lifting the liver with gauze or Nathanson liver retractor. Illustration: Rodrigo Tonan.
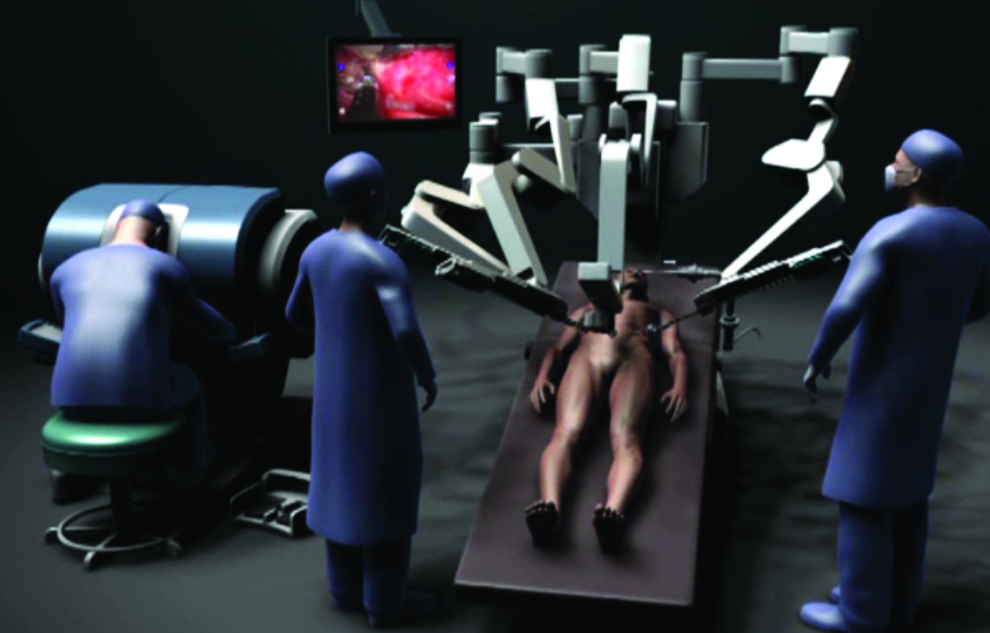
Position of the “cart.” Illustration: Rodrigo Tonan.
Most of the surgical procedure is performed using arm 1 (which simulates the surgeon's right hand) and arm 2 (which simulates the surgeon's left hand). In this situation, usually the arm 1 instrument presents the structures to be dissected by arm 2 instrument. According to the experience and training of the surgical team, the arms and instruments can be conveniently rearranged (Fig. 5).

Photograph showing the beginning of the procedure and the position of the instruments.
Distal Gastrectomy
Section of the gastrocolic ligament using ultrasonic forceps toward the lower pole of the spleen and brief vessels until identification and ligation of the left gastroepiploic artery and vein (Fig. 6).
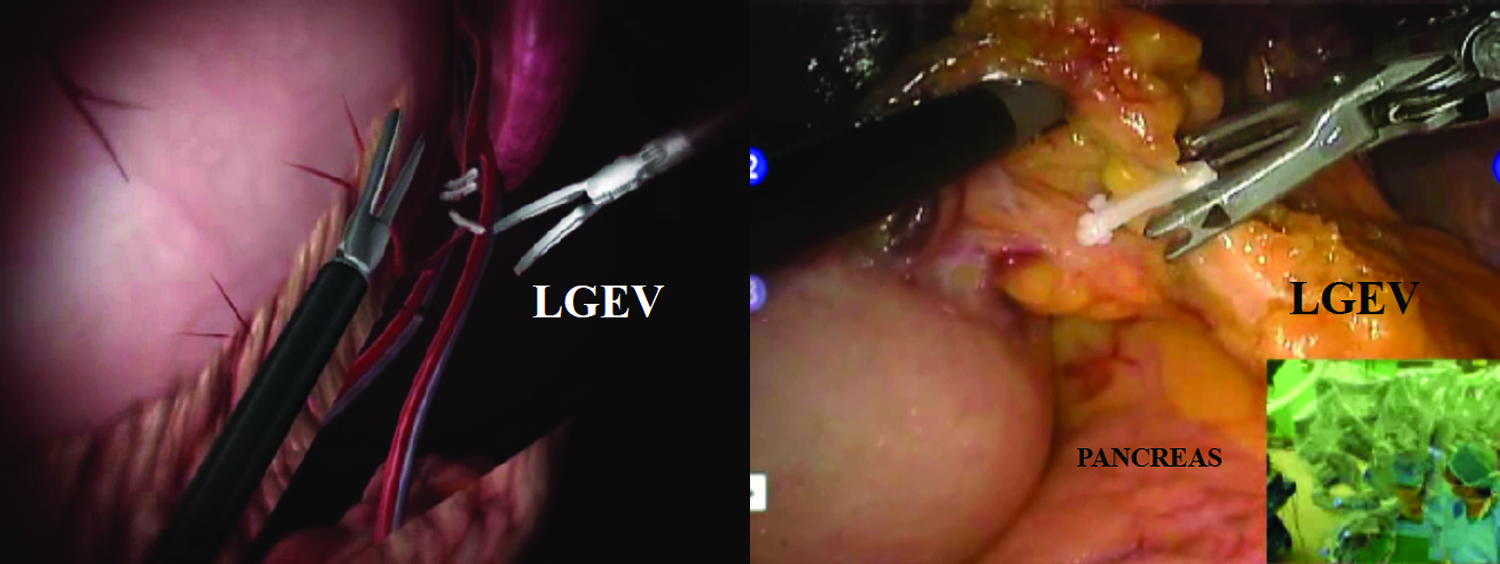
Clipping the vessels. LGEV, left gastroepiploic vessels. Left panel illustration: Rodrigo Tonan.
Dissection performed distally toward the pylorus until identification of the right gastroepiploic vessels. Lymphadenectomy of number 6 LN station (Fig. 7).
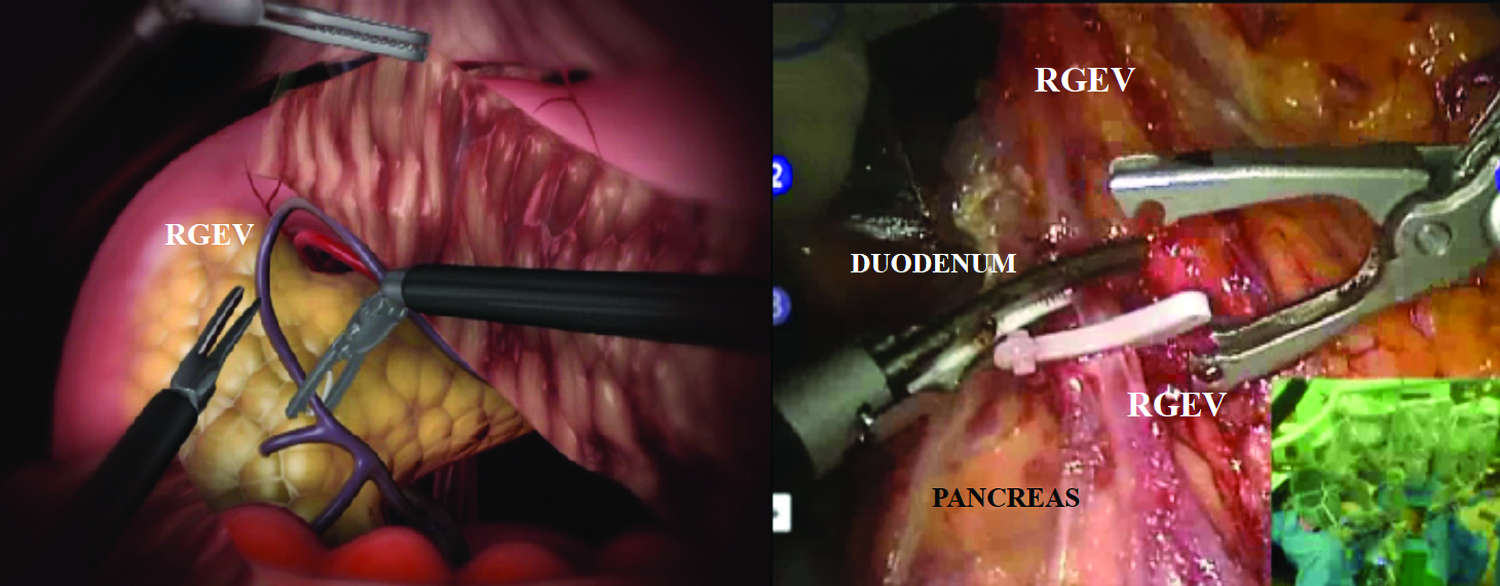
Clipping the vessels. RGEV, right gastroepiploic vessels. Left panel illustration: Rodrigo Tonan.
Opening of the lesser omentum and isolation and transection of the duodenum distally to the pylorus with laparoscopic stapler, performed by the assistant (Fig. 8).
Transection of the duodenum with 60 mm linear stapler white cartridge. Left panel illustration: Rodrigo Tonan.
Opening the lesser sac cranially to the right side of the esophageal hiatus.
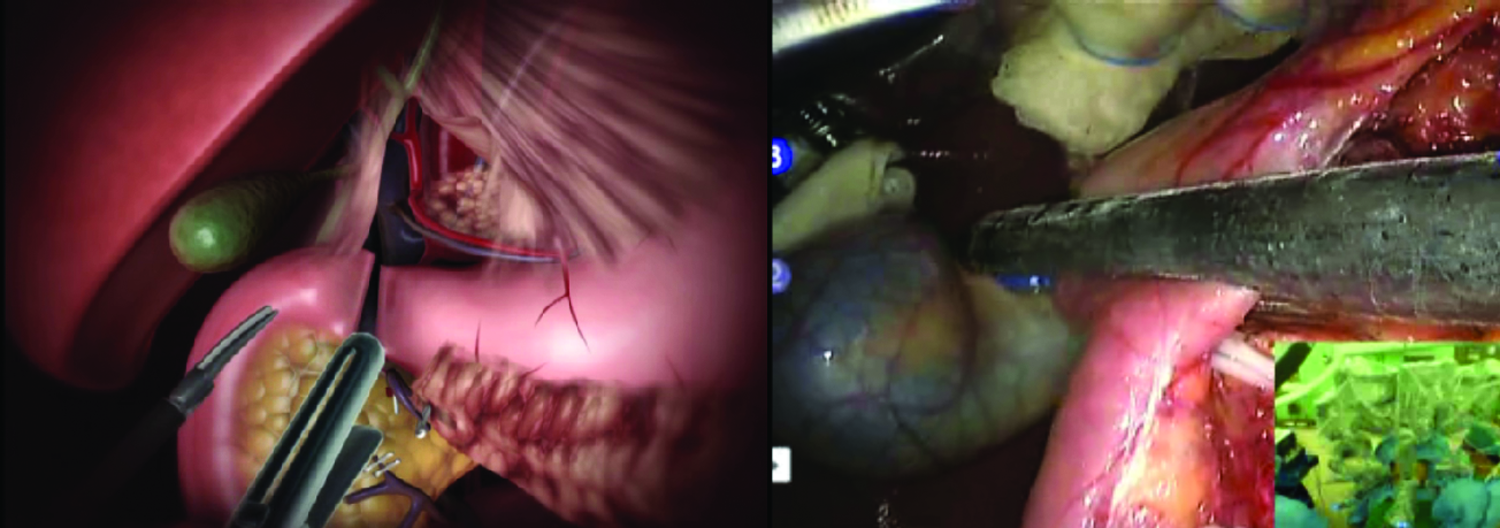
Exposure of the right gastric artery and section in its origin, and removal of the tissues of the 12 LN station around the proper hepatic artery and medially to the portal vein (Fig. 9).
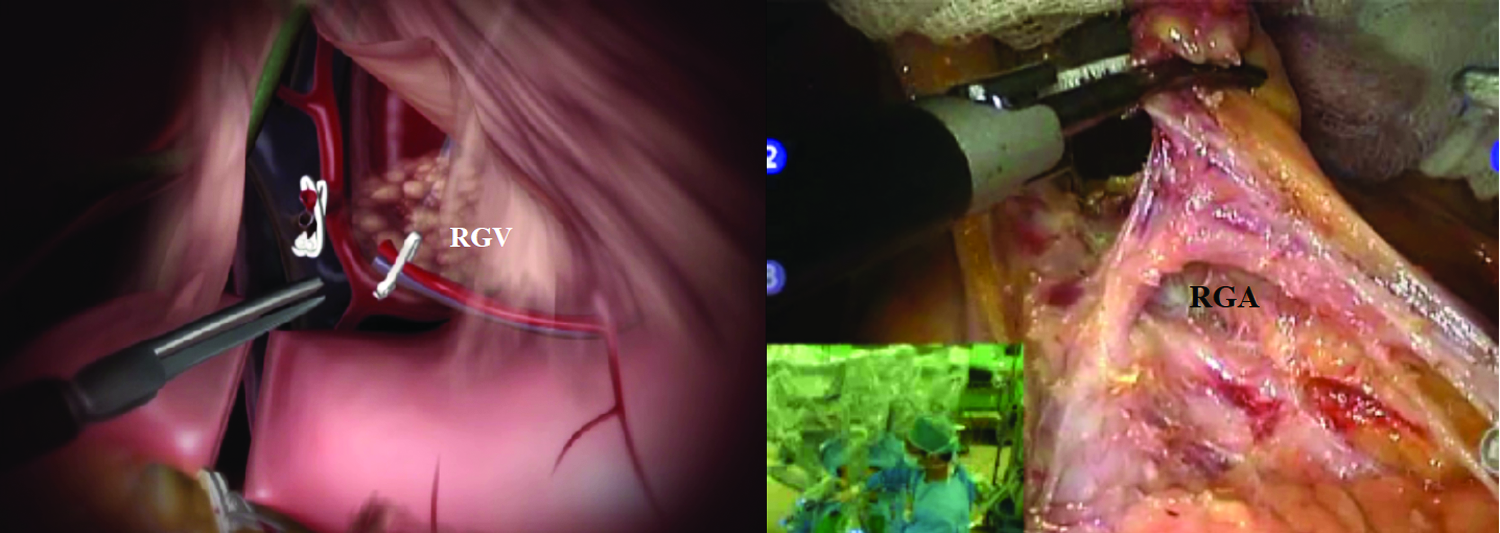
Isolation and ligation of the RGA and RGV at their origin. RGA, right gastric artery; RGV, right gastric vein. Left panel illustration: Rodrigo Tonan.
Exposure and section of the left gastric vein near the upper border of the common hepatic artery or pancreas during removal of the LN 8 station by anterior lifting of the stomach with the cadiere (Fig. 10).
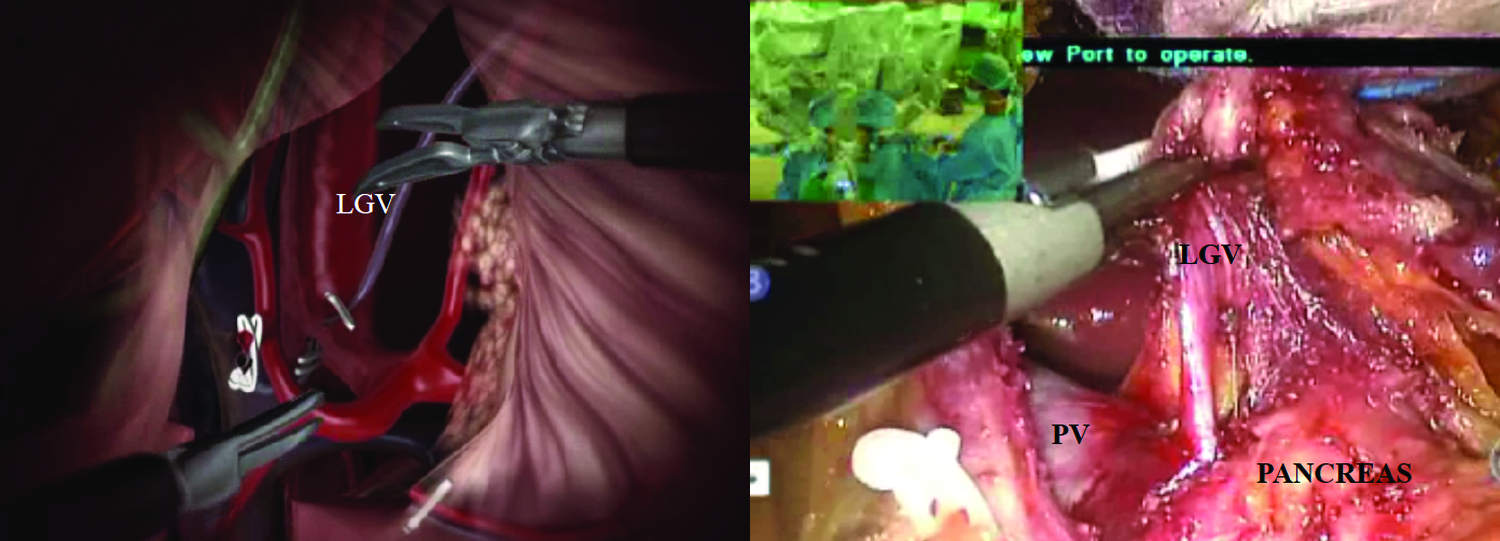
Isolation and ligation of the LGV proximal to the PV after lymphadenectomy of the region. LGV, left gastric vein; PV, portal vein. Left panel illustration: Rodrigo Tonan.
Exposure and section of the left gastric artery and lymphadenectomy of LN stations 7 and 9 (Fig. 11).
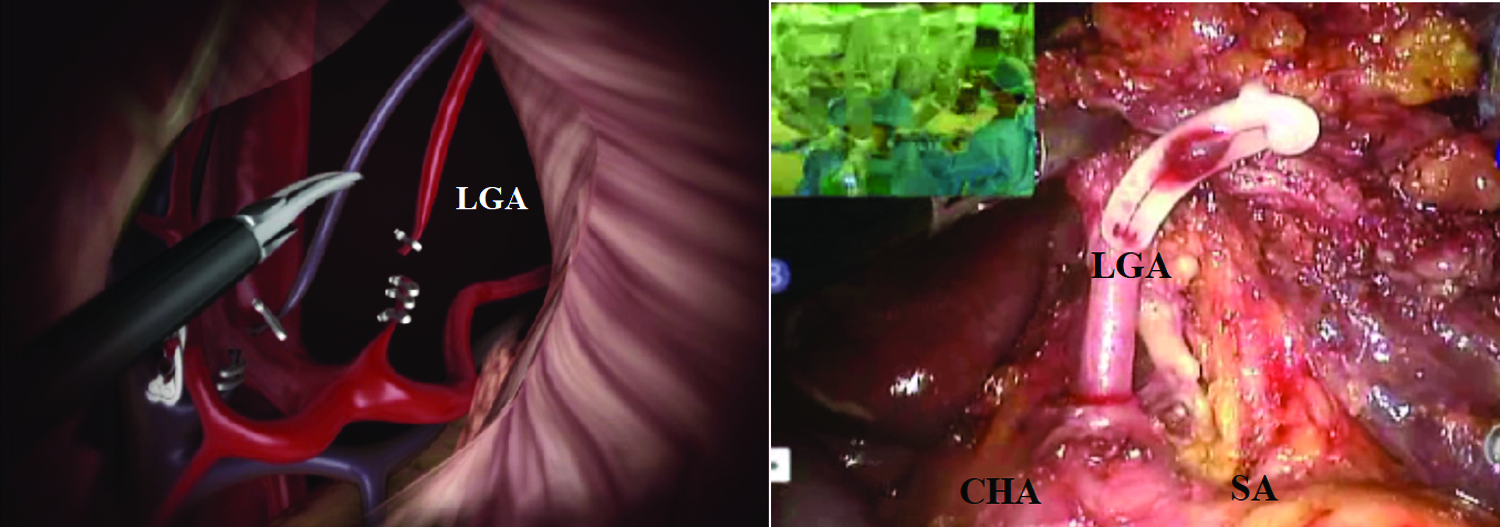
Celiac trunk exposure and its branches. CHA, SA, and ligation of the LGA. CHA, common hepatic artery; LGA, left gastric artery; SA, splenic artery. Left panel illustration: Rodrigo Tonan.
Perigastric retroperitoneum lymphadenectomy along the small curvature to the diaphragmatic crura and lymphadenectomy of the LN stations 1 and 3. After complete mobilization of the stomach, its section is practiced using a laparoscopic linear stapler (Fig. 12).

Lymphadenectomy of stations 1 and 3 and gastric section with 60 mm linear stapler blue cartridge. Illustration: Rodrigo Tonan.
The surgical specimen is placed inside a pouch.
In Roux-en-Y reconstructions, the gastrojejunal and jejunojejunal anastomoses can be done with endostaplers used by the assistant in synchrony with the surgeon's maneuvers. To avoid manual sutures, it has been preferred to close the entrance holes of the stapler blades using another load of the same instrument (Fig. 13).
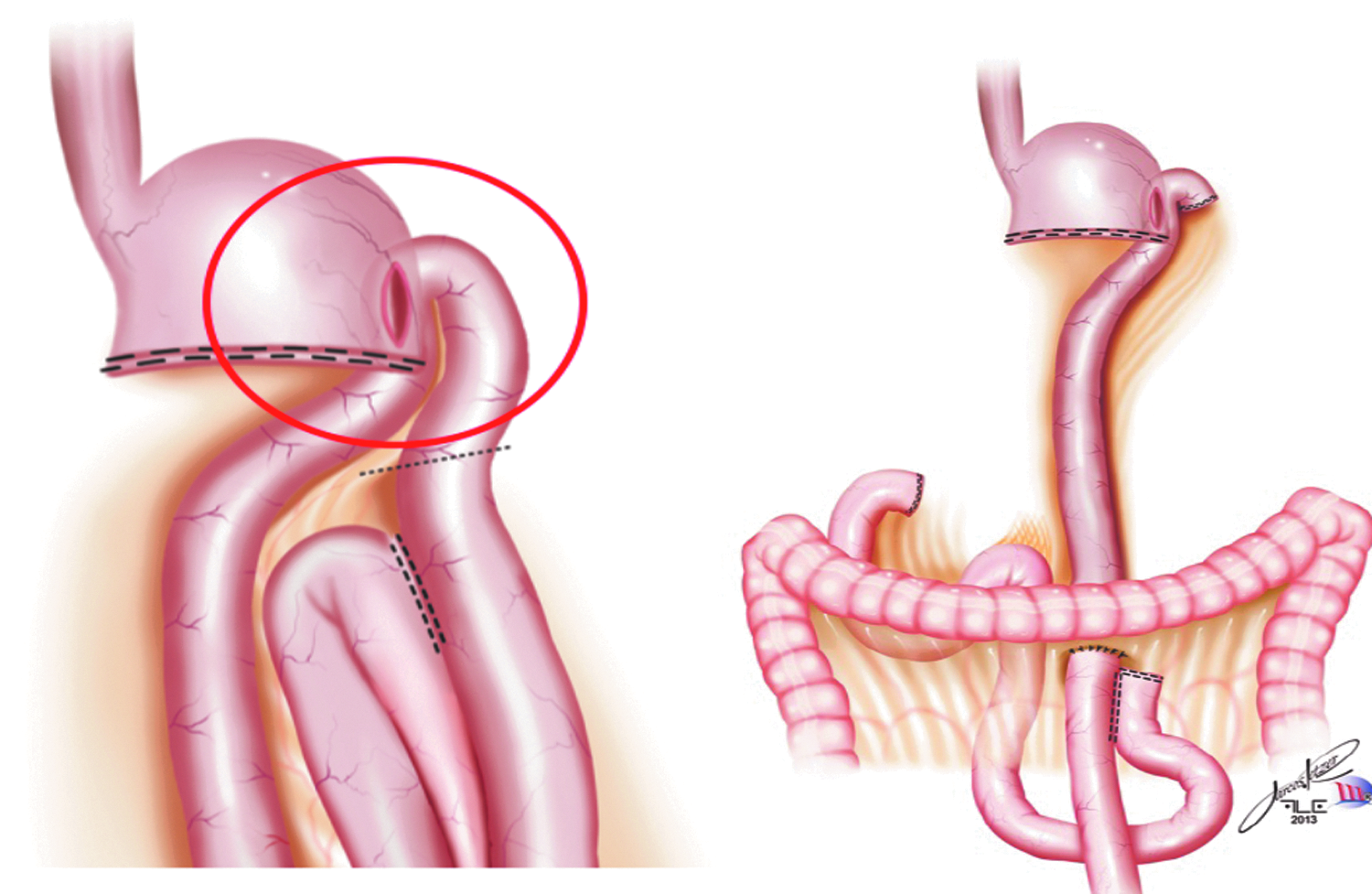
Roux-en-Y reconstruction. Gastrojejunostomy (red circle) and jejunojejunostomy (black dots). Illustration: Rodrigo Tonan.
The surgical specimen is removed by a median periumbilical incision or through a small Pfannenstiel incision, paying attention to adequate protection of the abdominal wall.
Total Gastrectomy
The procedure is similar to that described for partial gastrectomy, with the exception for dissection of short gastric vessels along the gastrosplenic ligament and the esophagojejunal anastomosis (EJA).
The dissection of the large curvature is completed by the section of the gastrosplenic ligament, after the control of the left gastroepiploic vessels to the diaphragmatic hiatus, removing the LN stations 4sa and 4sb (Fig. 14).
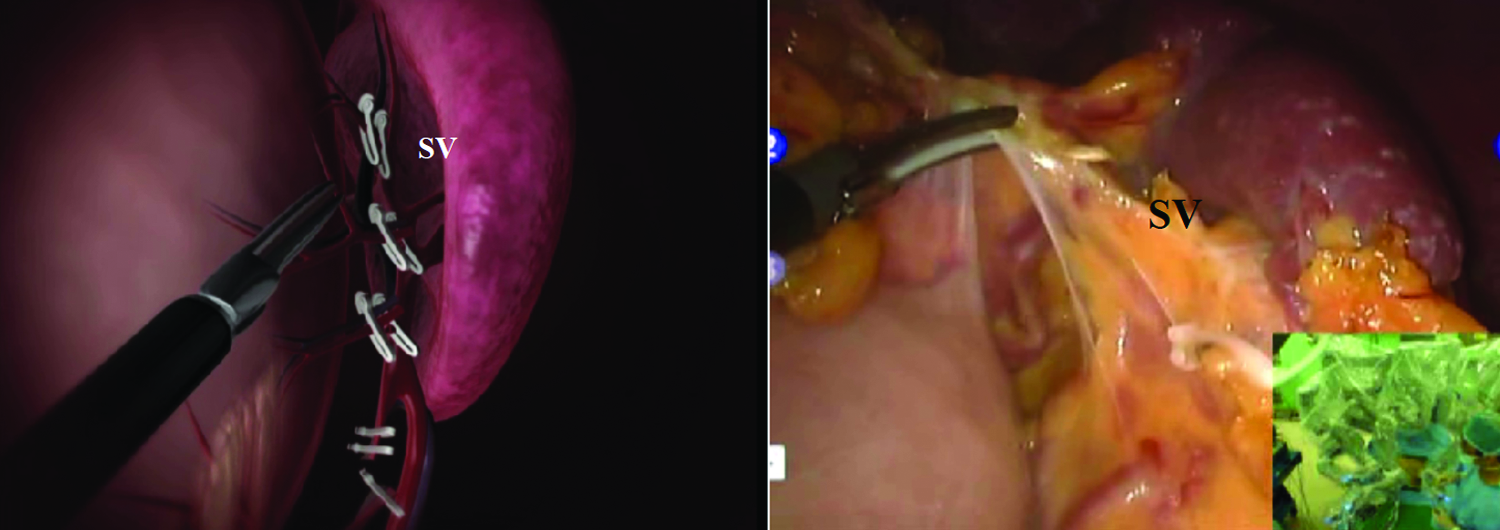
Isolation and ligation of the SV. SV, short vessels. Left panel illustration: Rodrigo Tonan.
The dissection of LN stations 10 and 11d depends on the type of lesion, and splenectomy may or may not be performed.
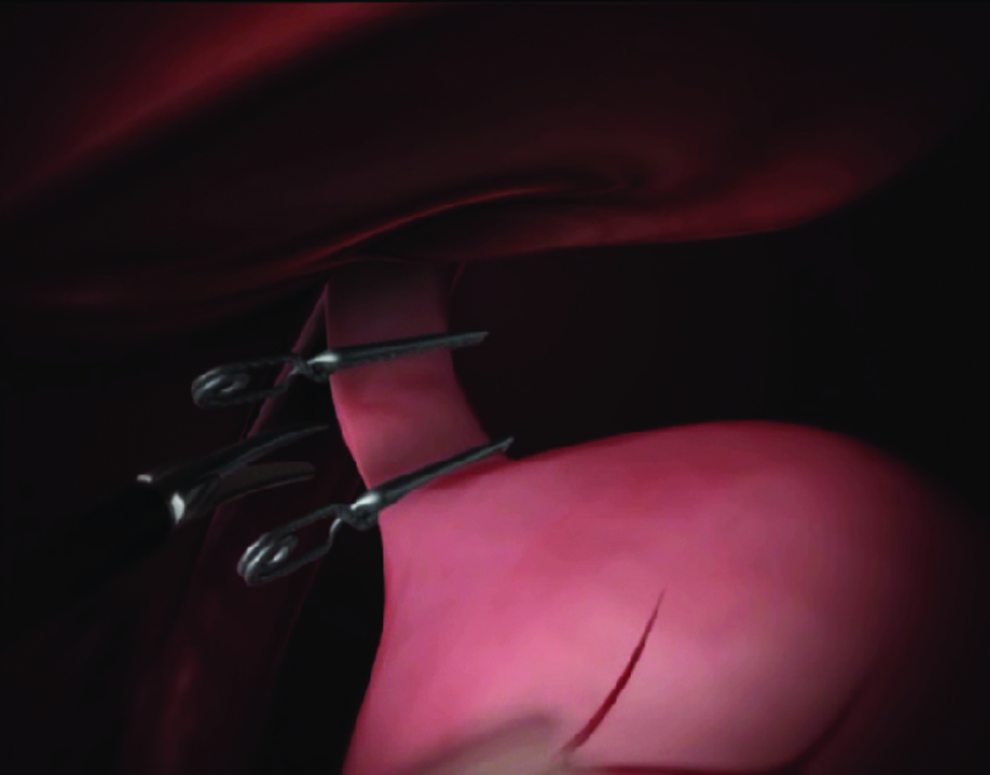
In Figure 15, we can see the dissection of LN station 11 from the celiac trunk, superior to the pancreatic border, toward the spleen, after mobilization of the stomach with arms 1 and 3 instruments.

Lymphadenectomy of stations 11p and 11d. SA, splenic artery. Illustration: Rodrigo Tonan.
The insulation of the abdominal esophagus is practiced through the section of the phrenoesophageal membrane and the vagus nerves. The stomach, once fully released, can be transected by a stapler (Fig. 16).
Transection of the esophagus with linear stapler white cartridge. Illustration: Rodrigo Tonan.
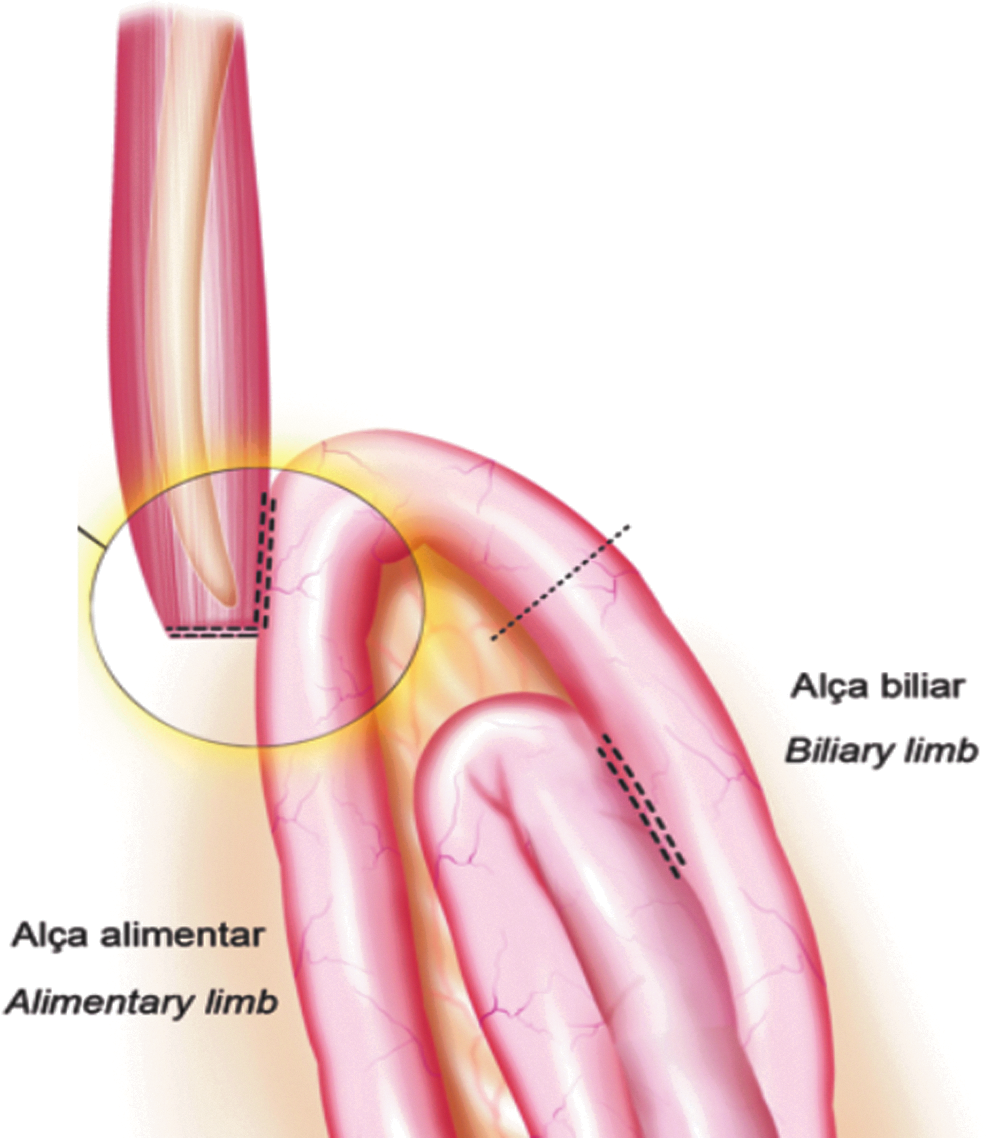
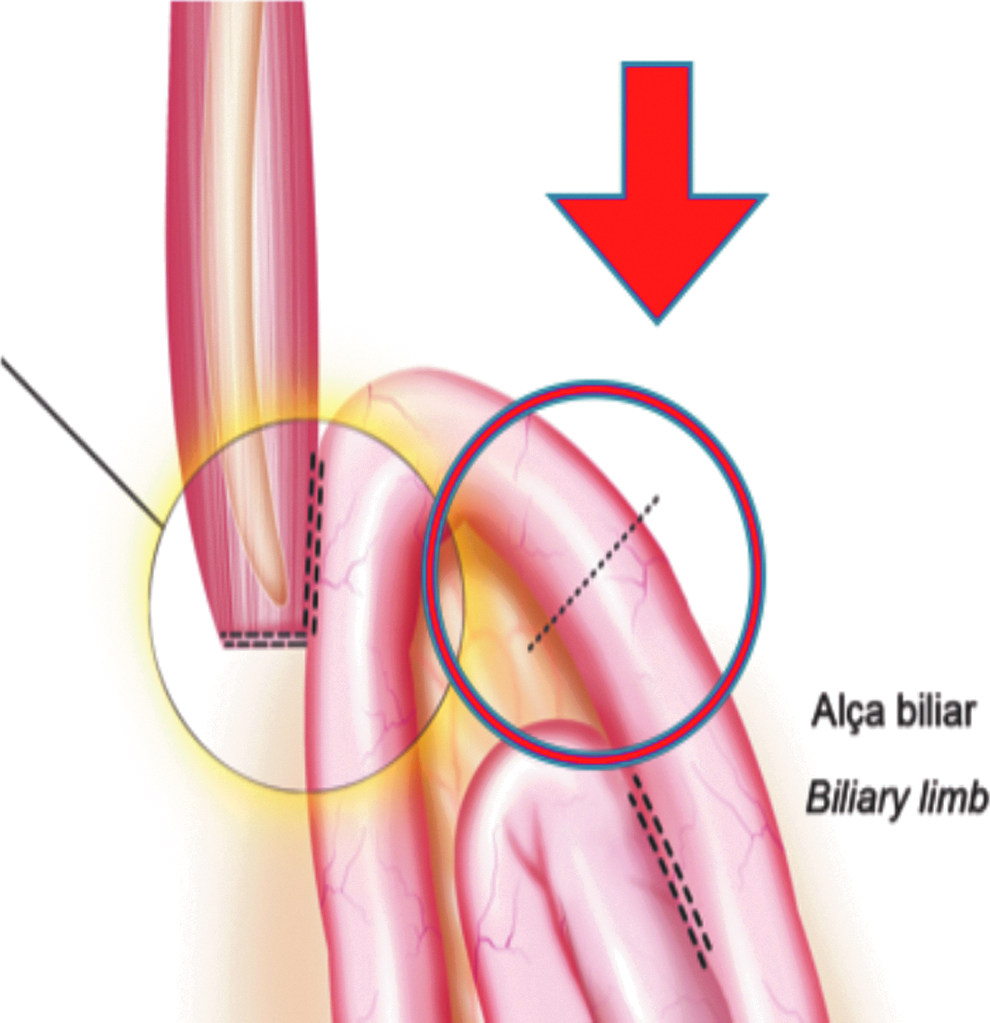
Identification of the first jejunal loop and measurement for anastomoses (Fig. 17).
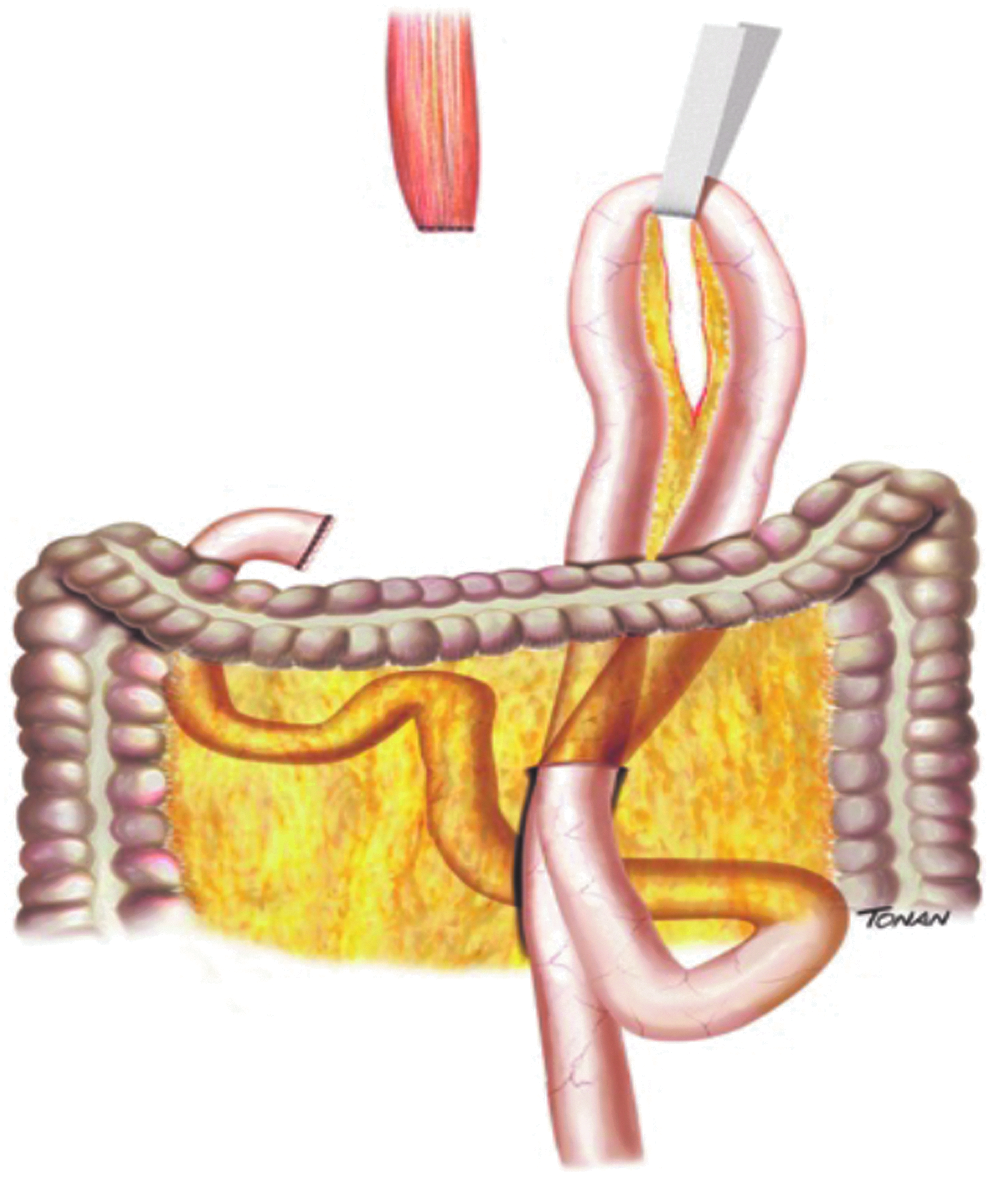
Mobilization of the jejunal loop to perform esophagojejunostomy. Illustration: Rodrigo Tonan.
The Treitz's angle is identified at 30–40 cm distal from it and a jejunal loop is identified, anchored by a Penrose drain and transposed by the assistant through the supramesocolic space, using a transmesocolic or precolic route; it is helpful if the jejunal loop is anchored by a stitch to the left lateral wall of the abdominally transected esophagus.
Esophagojejunal anastomosis (Fig. 18).
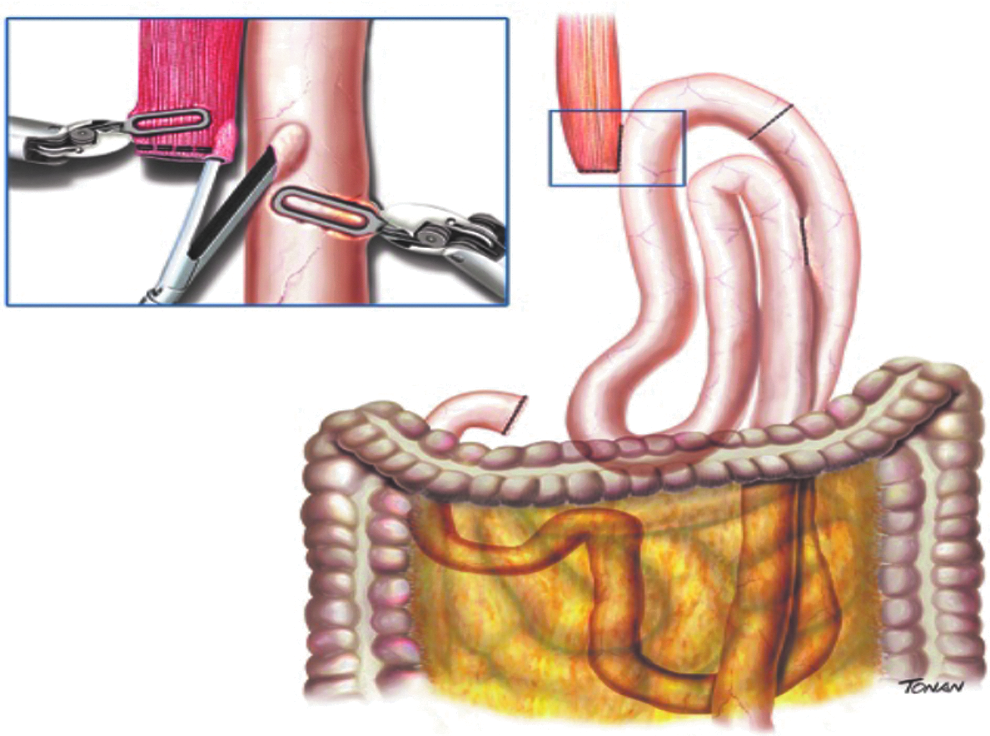
Laterolateral esophagojejunostomy with 45 mm linear stapler white cartridge. Illustration: Rodrigo Tonan.
The anesthesiologist introduces a 32 French bougie orally for easier exposure of the esophageal stump. A 60 mm linear stapler with white cartridge is utilized to perform the laterolateral EJA.
It is very important that, in this part of the procedure, the assistant who is holding the stapler stands still while the surgeon in the console manipulates the jejunal limb and the esophagus into the stapler.
Roux-en-Y reconstruction.
After completion of the mechanical anastomosis, the bougie already exposing the esophagus is introduced into the jejunal loop to ensure the diameter of the anastomosis and facilitate the closure of the common entry hole by hand sewing with an extramucosal 3–0 PDS® (polydioxanone) suture.
Next, an alimentary limb is isolated with a length of about 70 cm, brought into the upper abdomen close to the biliary limb, to perform the jejunojejunostomy of the Roux-en-Y reconstruction (Fig. 19).
Esophagojejunostomy (yellow circle). Jejunojejunostomy performed in the upper abdomen (black dots). Illustration: Rodrigo Tonan.
This anastomosis is performed with a 45 mm white cartridge linear stapler, once more with the assistant holding the stapler and the surgeon on the console manipulating the bowel into the stapler. The stapler entrance is closed by hand sewing with extramucosal 3–0 PDS®.
After both anastomoses have been completed, they are tested by instilling methylene blue solution through the esophageal bougie to ensure their integrity without leaks. Once tested, the biliary and alimentary limbs are divided and separated by utilizing the linear stapler with a 45 mm white cartridge (Fig. 20). In the transmesocolic route, the alimentary limb is tractioned and the enteroenterostomy is placed in the inframesocolic space (Fig. 21). The mesenteric gap is closed with a manual interrupted suture.
Transection of the biliary limb after anastomosis was tested with blue dye. Illustration: Rodrigo Tonan.
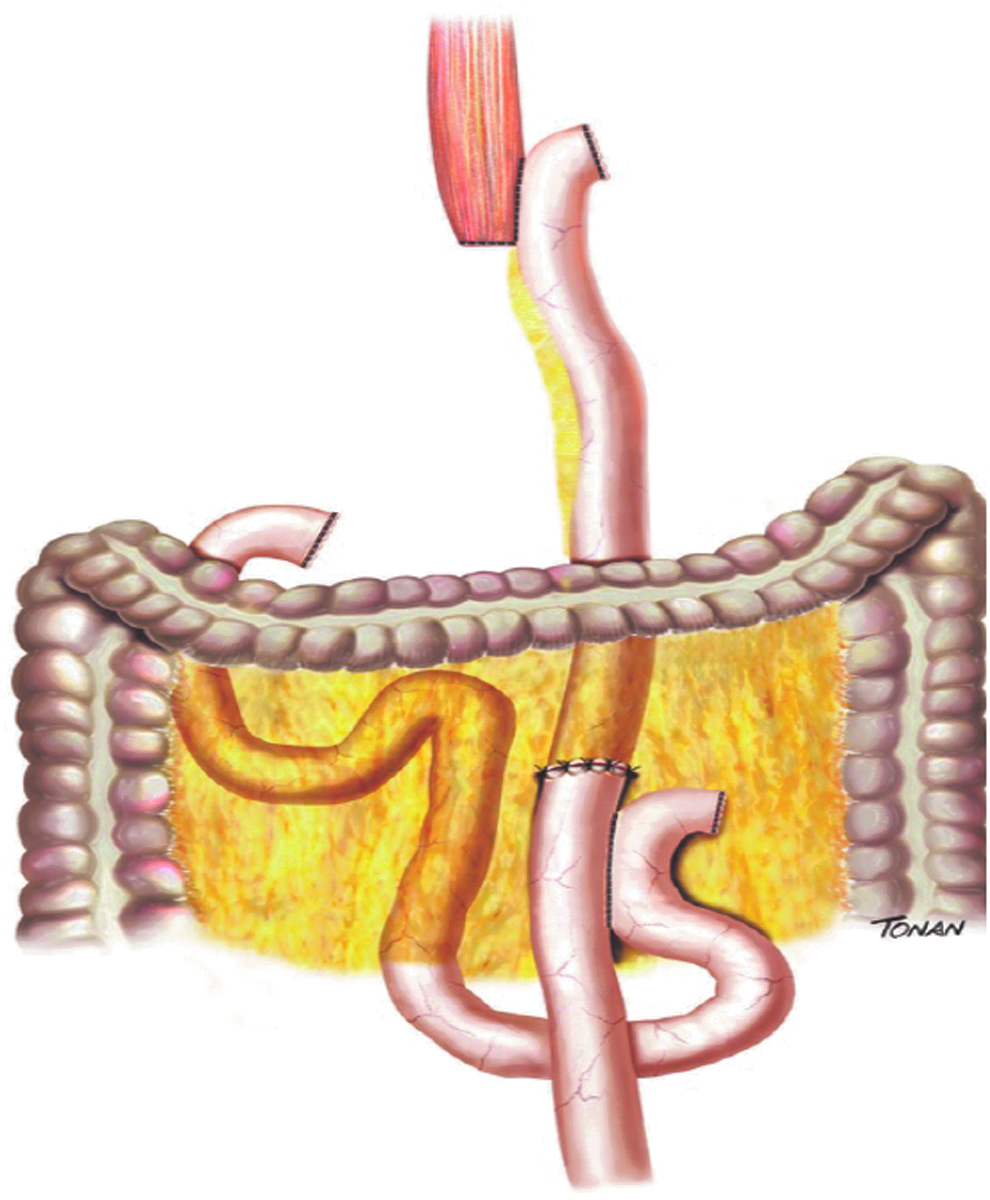
Final aspect of the digestive tract reconstruction. Illustration: Rodrigo Tonan.
After that, surgical revision, removal of the trocars under direct vision, drainage of the cavity, and synthesis of the abdominal have been practiced.
Present Evidence and Ongoing Data
The application of robotic surgery for GC remains open to discussion. Whereas several trials have reported the superiority of LG over the open approaches,9,16–18 the role of robotics in such a complex operation is yet to be elucidated. One of the main reasons is the lack of randomized trials addressing that issue. Other reasons stated are the exiguity of standardization as well as the stratospheric costs of robotic surgery.
Disadvantages of RG
Operation time
One of the main handicaps related to RG is the longer operative time. Both the time for setup, which includes the robot preparation and docking, and the console operation time are longer when compared with laparoscopic surgery in most of the case series, retrospective studies, and meta-analysis. A recent meta-analysis published by Wang et al. with 3744 GC patients included showed that the operation time was significantly shorter in the laparoscopic group. 19 Some studies indicate that operative time may decrease with the improved experience of the surgical staff. Hyun et al. demonstrated similar operative time between RG and LG after 20 initial cases (234 minutes versus 220 minutes; P = .198), suggesting that the learning curve effect plays an important role on the duration of the operation. 20 In fact, Liu et al. investigated the reasons why more time is needed in RG when compared with laparoscopy. The study included the overall operation time, operation time in each step, time required for instrument changes, and the number of intraoperative instrument changes and camera cleanings. The effective time was only 15.3 minutes longer for robotic distal gastrectomy than laparoscopic distal gastrectomy (145.9 minutes versus 130.6 minutes, respectively; P = .094). All other parameters were significantly longer in RG. The authors recommend that a smarter and simpler system for setup and swifter instrument changes should be developed to reduce the operative time. 21
Costs
Undoubtedly, robotic surgery has higher costs than open and laparoscopy surgery. With respect to robotic surgery for GC, studies that analyze its economic aspects are scarce. The analysis of the economic aspects or the economic evaluation of robotic surgery could be defined as the comparative analysis of alternative treatments in terms of costs and consequences. Kim et al. were one of the first to report the higher final costs of robotic surgery in a multicenter prospective nonrandomized study (robotic US$13,432 versus laparoscopic US$8090 per patient; P < .001). 13 Similar result was obtained in another Korean study, in which RG was 3189€ more expensive per patient when compared with laparoscopic surgery. 22 Interestingly, Lu et al. reported no difference in the direct costs between the two groups. However, RG was associated with higher indirect and total costs when compared with laparoscopic surgery (1.3 times, P < .001). 23 The monopoly established by the da Vinci Intuitive Surgical has led to rising costs and the relatively slow innovation. Recently, two other platforms have warranted regulatory approval in some countries (Senhance Surgical Robot and REVO-I Robot Platform) and are now in clinical use. Hopefully in the near future, added to new platforms that are still in the development process (Miro from Medtronic, Auris Robotics from Cambridge Medical Robotics, Verb Surgical from Google and Johnson & Johnson and Vecna Technologies), healthy competition will lead to innovation and lower prices. 24
Nonsuperiority of RG
Blood loss
Blood loss usually occurs during lymphadenectomy and is caused by vascular injuries. The 3D high-resolution images allow surgeons to identify small vessels with more accuracy. Still, the stable camera associated with the tremor filtering function concedes a better and more precise dissection. Several studies have demonstrated that blood loss is reduced in RG when compared with laparoscopic.25–27 A meta-analysis published by Hu et al. comparing the efficacy and safety of RG and LG with 3580 patients showed less intraoperative blood loss in the robotic group [weighted mean difference (WMD) of 29.85 mL, P < .05]. 27 These results were followed by other meta-analyses (Chen et al. WMD = 24.38 mL, P < .01 and Wang et al. WMD = 23.68 mL, P = .01).19,26 At the same time, it is important to emphasize that, although statistically significant, the difference in amount of blood loss identified in those studies may be clinically irrelevant. Excellent outcomes regarding blood loss have already been accomplished in LG, leaving little space for RG to demonstrate superiority.3,7,28
Number of harvested lymph nodes
Extended lymphadenectomy (D2) is considered the standard treatment for advanced GC.29–31 The removal of the suprapancreatic nodes (LN station numbers 8, 9, 11p, and 11d) is the most demanding step in LG and is directly related to survival.32,33 Initially, it was expected that the assistance of the robotic platform could improve the number of dissected lymph nodes. However, that was not observed in a nonrandomized prospective trial. 13 The nonsuperiority of RG regarding the number of harvested lymph nodes was confirmed in other meta-analyses.19,26 Conversely, other studies reported a greater number of lymph nodes dissected in RG.27,34 Still, recent reports stated that there is a clear benefit of RG when dissecting the N2 area and splenic preserving gastrectomy (LN station n.10) when compared with LG.35,36 Another potential benefit of RG is the removal of lymph nodes in obese people, which could be very difficult in LG, jeopardizing the oncological principles of radical gastrectomy.14,37
Length of hospital stay
Unquestionably, RG provides shorter hospital stay when compared with open gastrectomy.20,38 Nevertheless, the benefit of RG over LG remains unclear. Whereas most studies show no difference in the length of hospital stay between the two approaches,19,39,40 some studies reported the opposite. In a recent retrospective study, Liu et al. reported faster recovery and shorter hospitalization in the RG group (11 days versus 12 days; P < .0001). 41 Another report showed significantly improved hospital stay following surgery (robotic 14 days versus laparoscopic 15 days, P = .021). 42 Based on the present contradictory evidence, the benefit of RG regarding the length of hospital stay is yet to be elucidated.
Morbidity/mortality
The first large series to compare retrospectively open and laparoscopic- and robot-assisted gastrectomy was published by Kim et al. in 2012. There were 5839 patients included (4542 open, 861 laparoscopic, and 436 robotic). The authors found that the overall complication rate was similar between the three approaches, as well as the mortality rate. However, anastomotic fistula significantly occurred more frequently in the laparoscopic and robotic group. 43 Nevertheless, recent studies have proven the safety and feasibility of the minimally invasive digestive tract reconstruction method regarding anastomotic fistula.44,45 A nonrandomized multicenter prospective study compared the short-term outcomes between RG and LG. The rates of overall complications [11.9% (robotic) versus 10.3% (laparoscopic); P = .619] and major complications [1.1% (robotic) versus 1.1% (laparoscopic); P > .999] were similar between the two groups. There was no mortality rate in either group. That trial failed to demonstrate the superiority of the robotic approach over the laparoscopic one. On the contrary, it granted the safety and feasibility of robot-assisted gastrectomy for GC. 13 The high rate of conversion to open surgery has been related with higher complications and worse outcomes. However, most meta-analyses reported the same comparable outcomes regarding morbidity, conversion to open surgery and mortality rate between the two techniques.19,26,27,46,47 According to Hu et al., the incidence of complications in the robotic group was lower than in the laparoscopic group. Still, there was only one death in the robotic group, which was lower than in the other one (seven deaths). Notwithstanding, none statistical difference was found. 27
Oncological effectiveness
Data regarding the long-term outcomes and the oncological effectiveness after RG are still scarce. Much of the knowledge comes from a retrospective cohort, single-arm studies, or nonrandomized trials. The potential technical superiority of the robotic system over laparoscopy did not improve the oncological outcomes in a propensity-matched cohort analysis published by Obama et al. No statistically significant differences for 5-year overall survival (OS) or relapse-free survival (RFS) were observed. The median follow-up of 85 months in that study was long enough to evaluate long-term survival and recurrence. 48 In a meta-analysis published by Pan et al. concerning the long-term oncological outcomes involving 1614 GC patients, the OS, disease-free survival, and the recurrence rate were comparable between RG and LG. 49 Analogous results were obtained in a single-institution retrospective cohort study. No differences in 3-year OS (RG, 86.9% versus LG, 88.8%; P = .636) or 3-year RFS (RG, 86.9% versus LG, 86.3%; P = .905) were observed between the groups. 50 More reliable and elusive information regarding the long-term oncological effectiveness will be provided through ongoing randomized trials. 51 Comparable long-term outcomes of these two approaches were also found in a retrospective analysis for advanced cases. The respective OS rate in the propensity score matching between the robotic and laparoscopic groups was 76.1% and 79.8% (P = .552), and the respective RFS rate was 73.0% and 68.7% (P = .386). 52
Advantages of RG
Learning curve
In general, RG is performed by surgeons with great experience in LG. It has been reported that it takes between 40 and 60 cases for surgeons to reach a satisfactory perioperative outcome in LG. 53 On the contrary, an average of eight robotic procedures for laparoscopic surgeons to diminish the operative time is necessary. 22 Therefore, the learning curve of RG is overcome much faster than in the laparoscopic approach.54–56 Due to the technological superiority of robotic instruments and the absence of the fulcrum effect, the experience of performing robotic surgery is closer to open surgery. In this context, the robotic system may reduce the transition period between open and minimally invasive oncological gastrectomy. In fact, a recent report by An et al. showed that even for surgeons without experience in LG, the operative time rapidly decreased from the first to the fourth case in RG. The authors concluded that RG can be safely performed by a surgeon with extensive experience in open gastrectomy after 25 cases. 57 Moreover, hand sewing, including anastomosis, might be a very challenging and technical skill that is demanding in laparoscopic surgery. The robotic approach permits full hand-sewn (“robot-sewn”) anastomoses to be performed more easily. 58
Teaching and mentoring
The increasing utilization of a preoperative virtual reality simulator in robotic surgery plays an important role in decreasing the learning curve of robot-assisted operations. It allows surgeons to practice and improve basic robotic skills outside the operation room. To date, there are five commercially available virtual reality robotic surgical simulators (dVSS; Intuitive Surgical, Sunnyvale, CA), the Mimic dV-Trainer (dV-Trainer; Mimic Technologies, Inc., Seattle, WA), the Robotic Surgical Simulator (RoSS; Simulated Surgical Systems, Buffalo, NY), RobotiX Mentor (Simbionix USA, Inc., Cleveland, OH), and SimSurgery Educational Platform (SEP, SimSurgery, Norway). 59 Proficiency-based training has been the most effective training style. Other purposes of the virtual reality simulator models include utilization in assessment for recredentialing, advanced procedural-based training, and as a rehearsal tool before surgery. 60
In fact, Lee et al. developed an advanced real-time multidisplay educational system (ARMES) based on large experience in RG. The ARMES platform was based on standardization, key steps, and videos of gastrectomy with D2 lymphadenectomy. Finally, all instructional video clips were integrated into the robotic surgical console via a software. During the operation, the surgical view of the console shows the real-time surgery and the mentoring video next to each other, working as a guide for every step of the procedure. 61 Another pathway in the era of robotic surgery is telementoring and telesurgery. Surgical telementoring is the guidance to one surgeon by another expert in a different geographical location during a procedure, in which the expert is watching a real-time video feed of the operation. Telesurgery is a surgeon performing surgery on a patient from a remote site. The advancement of robotics and wireless communication technology allows both to become reality. 62 The world's first telesurgery was done in 2001 using the ZEUS robotic system. A female patient at a hospital in Strasbourg (France) had a successful cholecystectomy performed by a surgeon in New York. 63 Almost 20 years later after the “Lindbergh operation,” there are two main issues to be solved. Apart from the high costs, a major problem with telesurgery is the latency time (delay time), which could produce significant surgical inaccuracy and hazard the safety of the patient. The other one is the lack of the “haptic feedback,” which occurs not only in telesurgery but also in the regular bedside robotic surgery. At present, to feel the consistency of the tissue and the tension within the sutures is mostly relied on a visual feedback. Indeed, new prototypes and new technologies are on their way to overcome these lasting problems. 64
Navigation surgery and augmented reality
The elaboration of cameras that can use infrared spectral band technology with indocyanine green (ICG), a fluorescence dye, has innovated the way to visualize tumors, vascular structures, lymphatic channels, and lymph nodes. Such devices are not exclusively used in robotic surgery and are available in open and laparoscopic surgery. 65 Although the 3D high-resolution magnified vision present in the robotic platform highlights this technology. Kwon et al. have demonstrated the possibility of finding more metastatic nodes in RG with the use of navigation surgery with ICG (Firefly) when compared with historical controls. 66 Another study reported that the ICG fluorescence technique facilitates the identification of the infrapyloric artery during RG or LG, which is one of the most difficult time-consuming step in minimally invasive gastric resection. 67 Another advancement in robotic surgery is the possibility of using augmented reality, which can be defined as a fusion of projected computer-generated images and the real environment. In abdominal surgery, it is mostly used in pancreatic and liver resections, enabling better projection of large vessels, tumor sites, and accurate identification of individual's anatomy after neoadjuvant chemoradiotherapy. Still, it is useful for optimal placement of trocars. 68
Reduced-port gastrectomy
Reduced-port or single-incision laparoscopic surgeries were introduced with the expectation of better cosmetics, less pain, and to enhance patient's recovery after surgery. Studies indicate that morbidity was not higher in single-port cholecystectomy, although it may be considered a distressing approach. 69 In more complex procedures such as oncological gastrectomy, reduced-port or single-incision laparoscopies might be even more challenging. Thus, robotic surgery rectifies the disadvantages of laparoscopic reduced-port surgery as instrument collision decreased triangulation and difficulty in traction and contratraction maneuvers. Lee at el. outlined the safety and feasibility of reduced-port totally robotic distal gastrectomy with lymph node dissection in a phase I/II clinical trial, with no intraoperative event requiring conversion to laparoscopic or open surgery, and with no major complications. 70 These results were followed by Seo et al. in 40 consecutive patients who underwent reduced-port robotic distal gastrectomy with acceptable short-term outcomes. 71
Conclusion
RG has gained ground and has become a promising surgical approach. It is a useful tool in the hands of skilled and experienced surgeons in laparoscopy and should preferably be performed in reference centers with a large volume of procedures. At present, the high costs and the low availability often make it difficult to be spread out. The oncological results and publications of other institutions have demonstrated its safety and feasibility in GC treatment. Yet, the routine role of robotic surgery in GC is still under evaluation.
Footnotes
Disclosure Statement
This study was not funded and the authors declare no conflict of interest.