
Abstract
Abstract
Background:
Owing to the rising incidence of esophageal adenocarcinoma (EAC), we sought to assess the national trends in the use of different treatment modalities and compare survival outcomes among them.
Methods:
Using Surveillance, Epidemiology, and End Results (SEER) Program registry (2004–2014), we identified adult patients diagnosed with EAC undergoing definitive chemoradiotherapy (dCRT), esophagectomy, or neoadjuvant chemoradiotherapy plus esophagectomy (nCRT/S). Linear trends in the yearly incidence of each treatment were assessed using Poisson regression. An inverse probability of treatment weighted (IPTW) Cox regression was used to estimate the effect of each treatment on mortality. IPTW was used to account for potential confounding by year of diagnosis, patient demographics, and cancer characteristics.
Results:
A total of 10,755 patients were included in the study. From 2004 to 2014, the use of esophagectomy alone decreased from 15% to 5% (P < .0001), whereas nCRT/S increased from 14% to 20% (P < .0001); dCRT remained relatively stable (26% to 29%, P = .08). The 60-month survival rate was 13.0% for dCRT, 33.0% for esophagectomy only, and 36.3% for nCRT/S. After accounting for patient and cancer characteristics, both esophagectomy (hazard ratio [HR] 0.62, 95% confidence interval [CI] 0.55–0.70, P < .0001) and nCRT/S (HR 0.45, 95% CI 0.41–0.48, P < .0001) had significantly the highest survival rates.
Conclusion:
The use of esophagectomy alone has decreased, whereas nCRT/S has increased among EAC patients. Considering the better outcomes achieved with surgical resection, the use of dCRT should be discouraged in surgically fit patients.
Introduction
Cancer is the second leading cause of death in the United States 1 and esophageal cancer represents 4% of these deaths. 2 During 2018, there were 17.3 new cases and 15.9 estimated deaths, per 100,000 adults, 2 with a remarkable peak incidence mostly for men between the seventh and eight decade of life. 3 The two main histologic subtypes are esophageal adenocarcinoma (EAC) and squamous-cell carcinoma, the first one having a dramatic increasing incidence in the United States during the past decades.4,5
Depending on patient comorbidities and tumor stage (TNM value), among other individual characteristics, different treatment modalities are available for EAC patients: esophagectomy alone, definitive chemoradiotherapy (dCRT), and neoadjuvant chemoradiotherapy plus esophagectomy (nCRT/S).
Despite these different strategies, EAC patient's prognosis remains poor and still there is no strong evidence about a specific treatment algorithm. According to data from the Surveillance, Epidemiology, and End Results (SEER) and international cancer registries, EAC patients have a 19% 5-year survival, and ∼40% of the patients have advanced disease at the time of diagnosis. 6
Thus, the purpose of this analysis was to assess national trends in the use of different treatment modalities for EAC and compare survival outcomes.
Methods
Study design and patient population
Using the National Cancer Institute (NCI) SEER Program registry, adults who were ≥18 years old with diagnosis of EAC between 2004 and 2014 were eligible for inclusion.
The SEER program prospectively collects deidentified information on incident cancer cases from 19 population-based cancer registries, and covers roughly 35% of the U.S. population. 6
Treatments of interest included dCRT, esophagectomy alone, and nCRT/S.
Cancer cases were identified using International Classification of Diseases for Oncology, 3rd edition (ICD-0-3) codes 8140–8147 for site and histology, and esophagectomy was identified using SEER surgery codes 30, 40, 50–55, and 80. Cancer staging (primary tumor size, nodal involvement, and systemic disease) was captured using the American Joint Committee on Cancer (AJCC) TNM 6th edition. 7
To attempt to account for immortal person-time bias (i.e., bias introduced when time zero, eligibility, and treatment assignment are misaligned), patient follow-up was started 6 months after diagnosis. 8 This also means that patients who died within 6 months of diagnosis were excluded. By waiting to initiate follow-up, we attempted to exclude patients who were assigned to receive nCRT/S and then were unable to complete their planned treatment (patient choice, progression of disease, worsening performance status, or death), as they would have been inappropriately identified as having undergone dCRT in our analysis and biased the dCRT survival rates.
Statistical analysis
Patient demographics and cancer characteristics stratified by treatment modality were described using frequency tables and bivariate analyses. Potential linear trends in the yearly incidence of treatment type, among all patients diagnosed with EAC (irrespective of treatment), were assessed using Poisson regression.
Crude and weighted Cox proportional hazards regression was used to assess the marginal (i.e., overall) effect of treatment modality on all-cause mortality.
In brief, multivariable generalized logistic regression was used to estimate the probability of each patient receiving the treatment he or she did, given the year of diagnosis, patient gender, age, race/ethnicity, marital status, region, tumor grade, and derived AJCC 6th edition TNM. Age was modeled as a restricted cubic spline. Inverse probability of treatment weights (IPTW) was then calculated and standardized by the probability of undergoing that treatment in the total patient population. These weighting methods are preferable to traditional adjustment methods because it (1) effectively equalizes the distribution of the mentioned patient and cancer characteristics across each year, removing any confounding, and (2) allows for the marginal (i.e., overall) effect of treatment modality to be estimated, as opposed to the conditional (i.e., adjusted) effect.
To account for missingness of marital status, tumor grade, and AJCC TNM, inverse probability of missing weights (IPMW) was used. The probability of being a complete case (i.e., no missing data) was estimated using multivariable logistic regression, adjusting for year of diagnosis, patient gender, age, race/ethnicity, region, whether it was the patient's first cancer diagnosis, and treatment type. IPMW for each patient was stabilized using the overall probability of being a complete case. The IPTW and IPMW were multiplied together and truncated at the 5th and 95th percentiles to create the final overall weight for each patient. Robust sandwich estimators were used to estimate the 95% confidence intervals (CIs) to account for the weights. Weighted Kaplan Meier curves were also created.
All statistical analyses were performed using SAS® 9.4 (SAS, Inc., Cary, NC).
Results
Among the 10,755 included, 5475 (50.9%) underwent dCRT, 1820 (16.9%) underwent esophagectomy alone, and 3460 (32.2%) received nCRT/S. Demographics and cancer characteristics, stratified by treatment modality, are described in Table 1.
Distribution of Patient and Cancer Characteristics, Stratified by Treatment Regimen
AJCC American Joint Committee on Cancer; CI, confidence interval; SD, standard deviation.
During the study period, the percentage of patients undergoing esophagectomy alone significantly decreased from 14.6% to 4.8% (P < .0001), the percentage of dCRT increased from 25.45% to 28.5% (P = .08), and the percentage of nCRT/S significantly increased from 13.7% to 19.8% (P < .0001) (Fig. 1).
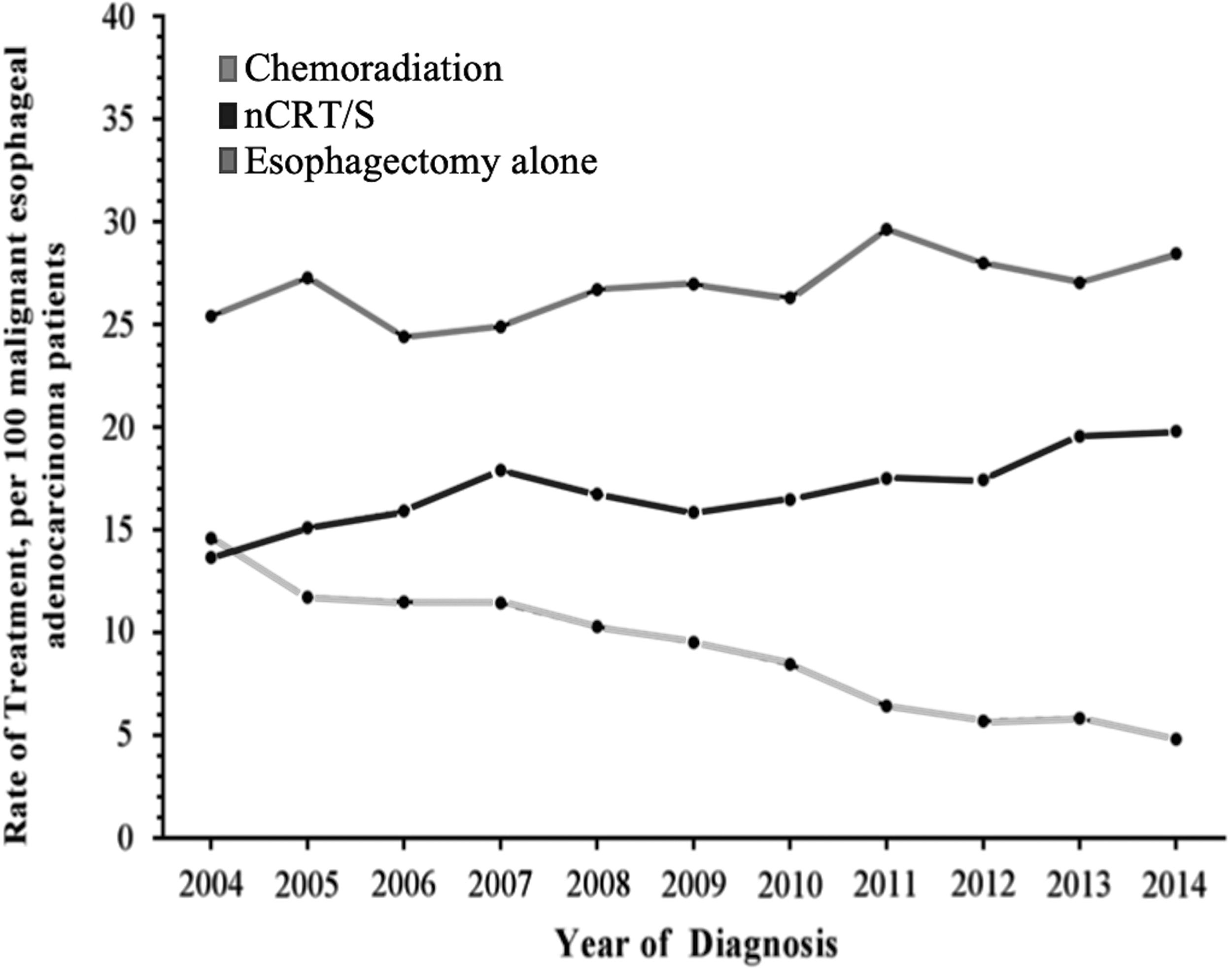
Rate of treatment, per 100 adults with malignant esophageal adenocarcinoma.
With a median follow-up of 15 months (interquartile range 7–33), the 60-month survival rate was 13.0% for chemoradiation only, 33.0% for esophagectomy only, and 36.3% for chemoradiation plus esophagectomy (Fig. 2). After accounting for patient and cancer characteristics, both esophagectomy (hazard ratio [HR] 0.62, 95% CI 0.55–0.70, P < .0001) and nCRT/S (HR 0.45, 95% CI 0.41–0.48, P < .0001) had significantly lower rates of mortality than chemoradiation only (Table 2).
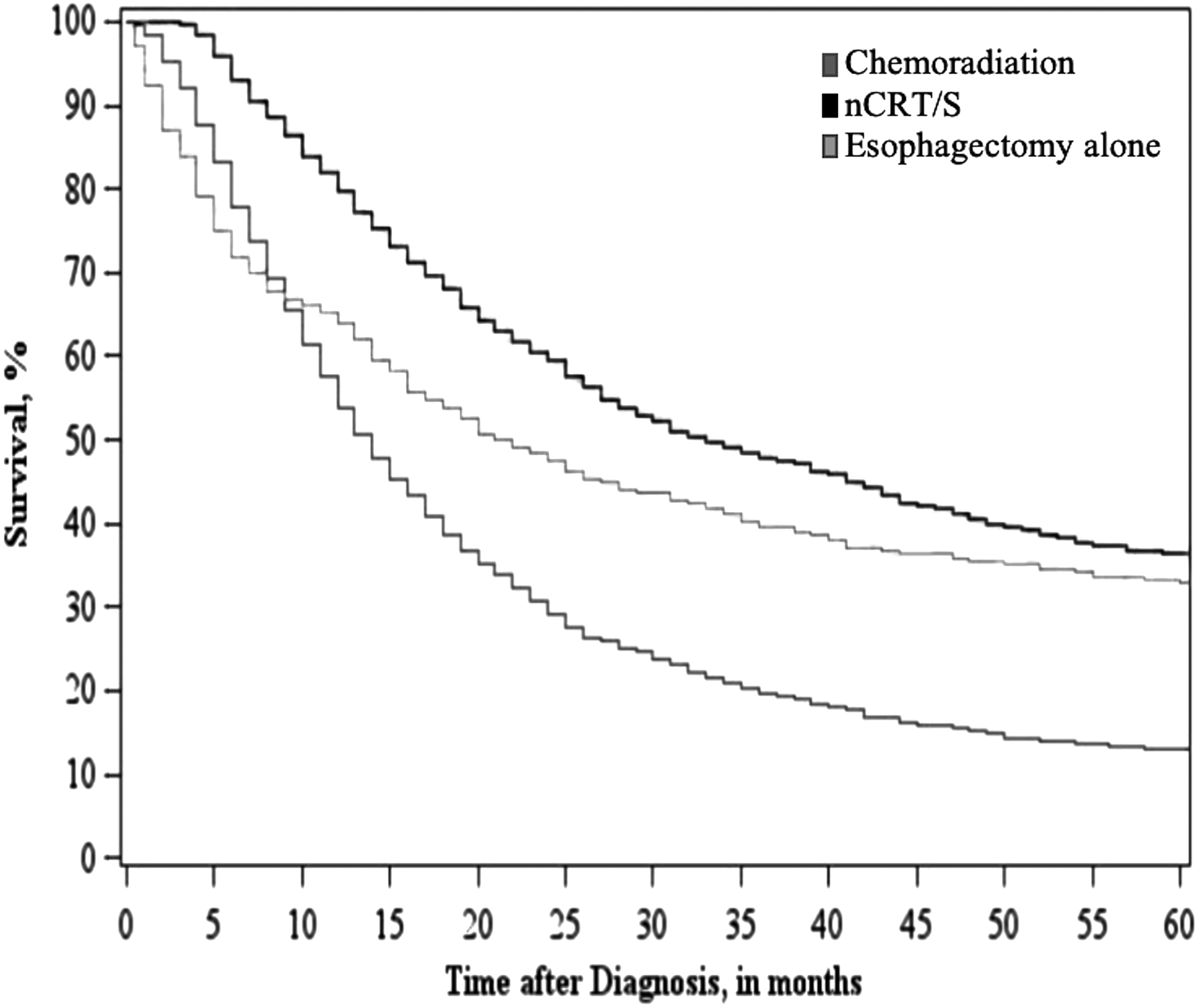
Standardized survival of adult patients with malignant esophageal adenocarcinoma, stratified by treatment regimen.
Crude and Standardized Hazard Ratios Comparing the Potential Effect of Treatment Regimens on All-Cause Mortality
Stabilized inverse probability of treatment weights was created adjusting for year of diagnosis, patient gender, age, race/ethnicity, marital status, region, cancer grade, first cancer diagnosis, derived AJCC T, 6th edition value, derived AJCC N, 6th edition value, and derived AJCC M, 6th edition value; inverse probability of missing weights was used to account for missing data; inverse probability of censor weights was created adjusting for year of diagnosis, patient gender, age, race/ethnicity, marital status, region, cancer grade, and first cancer diagnosis.
Confidence intervals were estimated using robust sandwich estimators to account for the weights.
AJCC, American Joint Committee on Cancer; CI, confidence interval; HR, hazard ratio.
Discussion
By performing this population-based analysis, we aimed to assess the national trends in the use of dCRT, esophagectomy alone, and nCRT/S, and compare survival outcomes among these treatment modalities for EAC patients. The results of our study showed a significant decreasing trend of esophagectomy alone, a significant increase of nCRT/S, and a trend toward increase of dCRT. Furthermore, we found that the 5-year survival rate for both esophagectomy alone and nCRT/S was significantly higher than that for dCRT.
Several studies had analyzed these modalities independently one from each other. For instance, Schlottmann et al. 9 demonstrated an overall decreasing trend of patients undergoing esophagectomy for EAC in the United States from 2004 to 2014. Interestingly, this decreasing rate was only statistically significant for patients >70 years of age. On the contrary, in an England population-based analysis of EAC patients only, Chadwick et al. 10 reported that esophagectomy remained the initial treatment of choice for early-stage EAC. In our analysis, we found a significant increase in the use of nCRT/S for EAC patients. Coinciding with these data, the Dutch cohort study 11 showed a significant increase in rate of multimodality treatment for EAC patients within the study period (2000–2012); nCRT/S was used in 85% of patients.
Our study suggests that EAC patients may obtain better long-term survival with a combination of chemo- and radiation therapy followed by esophagectomy, dCRT was associated with the lowest survival rate.
In 1999, dCRT was established as the optimal treatment modality for EAC patients by Cooper et al. 12 It was the first trial (RTOG 85-01) combining radiotherapy with chemotherapy for esophageal carcinoma (for both adenocarcinoma and squamous cell carcinoma). They enrolled 129 patients with localized disease (T1-3 N0-1 M0). Of those, 123 were eligible for the randomized trial: 62 for the radiotherapy arm (64 Gy only) and 61 for the combined modality arm (50.4 Gy+cisplatin +5-FU). In this randomized part of the trial, they showed a 26% 5-year survival for the combined therapy versus 0% for radiotherapy alone. For the nonrandomized part of the trial, combined therapy led to a 14% 5-year survival. Later, several studies such as the INT 0123 phase III trial performed by Minsky et al. 13 compared different radiotherapy doses to assess locoregional recurrence. Interestingly, the higher dose of radiotherapy failed to control the locoregional recurrence, and treatment-related mortality was greater in patients with higher radiotherapy doses.
In contrast, the Chemoradiotherapy for Esophageal Cancer followed by Surgery Study (CROSS) trial 14 enrolled 368 patients of whom 366 were included in the analysis (EAC 75%). A R0 resection was achieved in 92% of nCRT/S patients but in 69% in the surgery group (P < .001). The overall 5-year survival rate for the nCRT/S group was 47% versus 34% for the esophagectomy alone group. The neoadjuvant therapy proposed by this trial (paclitaxel/carboplatin—41.4 Gy/23 fractions+esophagectomy) has become the standard of care for locally advanced EAC. This landmark study was later confirmed by the longer follow-up results, showing better locoregional and systemic recurrences control with this proposed combined therapy.15,16
Hopefully, the ongoing Irish randomized Neo-AEGIS trial (ICORG 10–14) 17 will help finding the optimal standard of care for EAC patients.
Remarkably, few studies have compared long-term survival outcomes between dCRT and nCRT/S in these patients. Recently, a retrospective population-based analysis including 2633 EAC patients showed a 13% 5-year survival rate after dCRT and a 27% 5-year survival rate after nCRT/S (P < .0001) for stage III EAC. 18 Sjoquist et al. 19 recently conducted a meta-analysis including 4188 patients providing strong evidence for a survival benefit of nCRT/S over surgery alone in patients with EAC. Finally, contrary to our results, Haefner et al. 20 showed no statistical difference in the 5-year survival rate between dCRT and nCRT/S.
The main limitations of this study are inherent to its retrospective nature. In addition, several limitations are due to the lack of information in the SEER database. Our study period analyzed 11 years worth of data, in which only 10,755 patients were enrolled. Considering both, that the SEER database covers 34.6% of the U.S. population and the concerning rising incidence of EAC, our study population represents <10% of all new EAC cases in the United States. Furthermore, owing to the lack of information about patient quality of life and comorbidities, we cannot determine why patients classified under the same TNM were treated with different modalities. Despite these limitations, to our knowledge, this is the first study comparing national trends of treatment modalities and survival for EAC.
Conclusions
In the United States, the use of esophagectomy alone has decreased while the use of nCRT/S and dCRT has increased for EAC patients. Considering the better outcomes achieved with surgical resection, the use of dCRT should be discouraged in surgically fit patients.
Footnotes
Disclosure Statement
No competing financial interests exist.