
Abstract
Abstract
Background:
Inguinal hernia in children is currently treated through a groin incision with access to the inguinal canal and handling of the spermatic cord. In the face of the growing utilization of laparoscopic surgery in Nigeria, it was important to compare the outcome of laparoscopic and open herniotomy (OH) in our local teaching hospital to create a basis for recommendation.
Objectives:
We compared OH with laparoscopic needle assisted hernia repair (LNAR) in children in Obafemi Awolowo University Teaching Hospital Complex, Ile Ife.
Methodology:
A prospective study involving children who presented with uncomplicated inguinal hernia, carried out within the period of 1 year in our center.
Results:
In the LNAR group, there were 24 (75%) males and 8 (25%) females, while in the OH group, there were 29 (90.6%) males and 3 (9.4%) females. The age range for LNAR was 2–156 (median = 44) months and OH was 2–168 (median = 36) months. Higher complication rate for OH was found to be statistically significant (P = .001). The total operating time was found to be similar between the two groups for both unilateral and bilateral hernias (P = .636 and P = .334, respectively). Two contralateral patent processus vaginalis (PPV) were identified during laparoscopy and were repaired at the same sitting.
Conclusion:
Postoperative complications are significantly lower with LNAR. Duration of surgery for LNAR is similar to OH. Incidence of contralateral PPV seen following unilateral LNAR is low.
Introduction
The principle for indirect inguinal hernia repair in children is the ligation of the patent processus vaginalis (PPV) at the level of internal ring. 1 This can be achieved either by conventional open method or by laparoscopic technique. Laparoscopy is also useful in identifying asymptomatic contralateral PPV, enabling its repair in single sitting. 2
In a bid to reduce operation time, improve cosmesis, and reduce the risk of complications, several techniques have been proposed for open herniotomy (OH). These range from the use of groin crease incision with opening of the external oblique to access of the inguinal canal popularized by Ferguson, 3 or without opening the external oblique (mobilizing the PPV through the external ring) as described by Mitchell-Bank.3,4
In 1999, Koyle et al. 5 utilized a single high scrotal incision, introduced by Bianchi and Squire 6 initially for the treatment of palpable undescended testes, to treat congenital hernias secondary to PPV. Although inguinal and scrotal approaches are effective in obliterating the PPV, it is arguable that the dissection of PPV may be accompanied by an increased risk of injury to the vas deferens and its accompanying vessels, which may be a potential cause of infertility. 7 In addition, patent contralateral deep ring cannot be accessed at OH, making some surgeons to opt for routine contralateral groin exploration for possible PPV.8–11
With the advent of laparoscopy, the examination of contralateral groin can now be done without the unnecessary risk involved in contralateral groin exploration and handling of the spermatic cord. 1
We aim to compare the early postoperative complications of OH with laparoscopic needle assisted hernia repair (LNAR) in children, as well as the duration of surgery, and the frequency of contralateral undiagnosed PPV seen on laparoscopy.
Justification
OH in children is popular in Nigeria; however, its potential complications due to manipulation and dissection of the spermatic cord have created room to welcome improvements. Although foreign studies on laparoscopic herniotomy have highlighted the advantages and how they compare with OH, it was important however to compare the outcome of laparoscopic and OH in our local teaching hospitals as there is no local data to recommend either.
Materials and Methods
This was a prospective randomized study involving children between 1 month and 15 years old who presented with clinical diagnosis of uncomplicated indirect inguinal hernia. This study was approved by the Ethics Committee of the Obafemi Awolowo University Teaching Hospital Complex (Ile Ife) and carried out between January 2017 and December 2017.
Children between 1 month and 15 years of age with a clinical diagnosis of uncomplicated indirect inguinal hernia were included; however, patients with recurrent hernias, urinary bladder outlet obstruction (posterior urethral valve, urethral stricture, and prune belly syndrome), associated undescended testis, associated ambiguous genitalia, and patients requiring working ports/instruments during laparoscopy were excluded.
Sample size estimation
The sample size estimation was powered to detect the frequency of postoperative complications, including wound infection, scrotal/labial edema, iatrogenic undescended testis, postoperative hydrocele, and early recurrence as primary outcome variables; therefore, the secondary outcome variable will include operating time and frequency of contralateral PPV in patients that had LNAR.
Using the Sathian formula for difference in proportion, 12
n = minimum sample size per group
p1 and p2 are the proportion estimates from previous studies based on the overall rate of complications of OH (p1) 13 and LNAR (p2) 1
Zβ at desired power of 80% = 0.84
Zα represents the desired level of statistical significance = 1.96

To allow for attrition and increase statistical power 10% was added, making a total of 34 patients per group. Therefore a total number of 68 patients were recruited for the study.
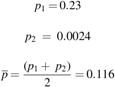
The patients were randomized to groups A and B, corresponding to OH and LNAR, respectively, using simple randomization by balloting. Parents/guardians blindly picked from opaque envelopes containing either A or B in a bag. CONSORT flow chart is shown (Fig. 1).
CONSORT flow diagram.
LNAR technique described by McClain et al. 14 and OH described by Ferguson 15 were adopted for this study. Assessment of postoperative complications was done by a pediatric surgeon who did not participate in the surgery and was based on clinical judgment only. Duration of follow-up was limited to 3 months, and only early postoperative complications were evaluated.
Open herniotomy
A groin crease incision was made and deepened until the external oblique aponeurosis was visualized (Fig. 2). The aponeurosis was divided along the line of its fibers to lay open the inguinal canal. The hernia sac was identified anterior and medial to the spermatic cord and dissected free from the spermatic cord up to the deep ring evidenced by presence of preperitoneal fat, taking care to avoid injury to its contents (Fig. 3). The sac was then divided and transfixed at the most proximal part with 2/0 vicryl suture. The spermatic cord was realigned in the inguinal canal by pulling on the testis from the scrotum. The external oblique aponeurosis was closed with running vicryl 2/0 suture, and the wound was closed with subcuticular suture. The wound was cleaned with antiseptic solution, and sterile dressing was applied (Fig. 4).

Groin crease incision (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).

Sac completely mobilized and opened (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).

Wound closed in subcuticular manner (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).
Laparoscopic needle assisted hernia repair
A 5 mm port was introduced through an infraumbilical incision using the Hasson open technique for laparoscopic access, and the peritoneal cavity was insufflated with CO2 at 2 L/minute, to achieve an intra-abdominal pressure of ∼8 mmHg. A 5 mm, 0° telescope was introduced to visualize the peritoneal cavity. No other port was introduced throughout the procedure, and no working instrument was used. The PPV is identified and the contralateral deep ring examined for PPV which, if present, was also repaired in the same sitting. Contents of the hernia were reduced with external pressure to allow safe ligation of the PPV. Patients that required working instrument to allow adequate reduction were excluded from the study to ensure uniformity.
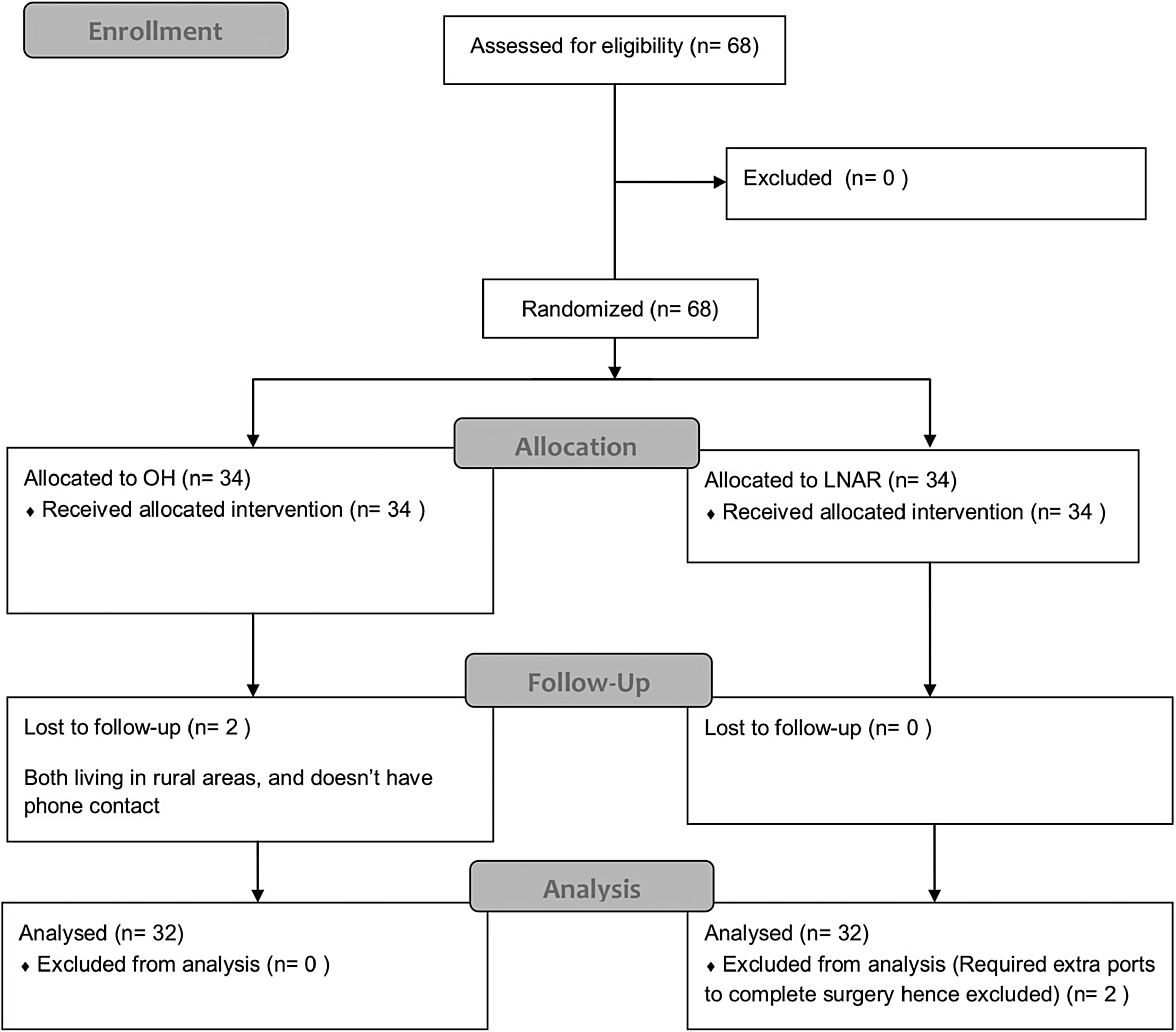
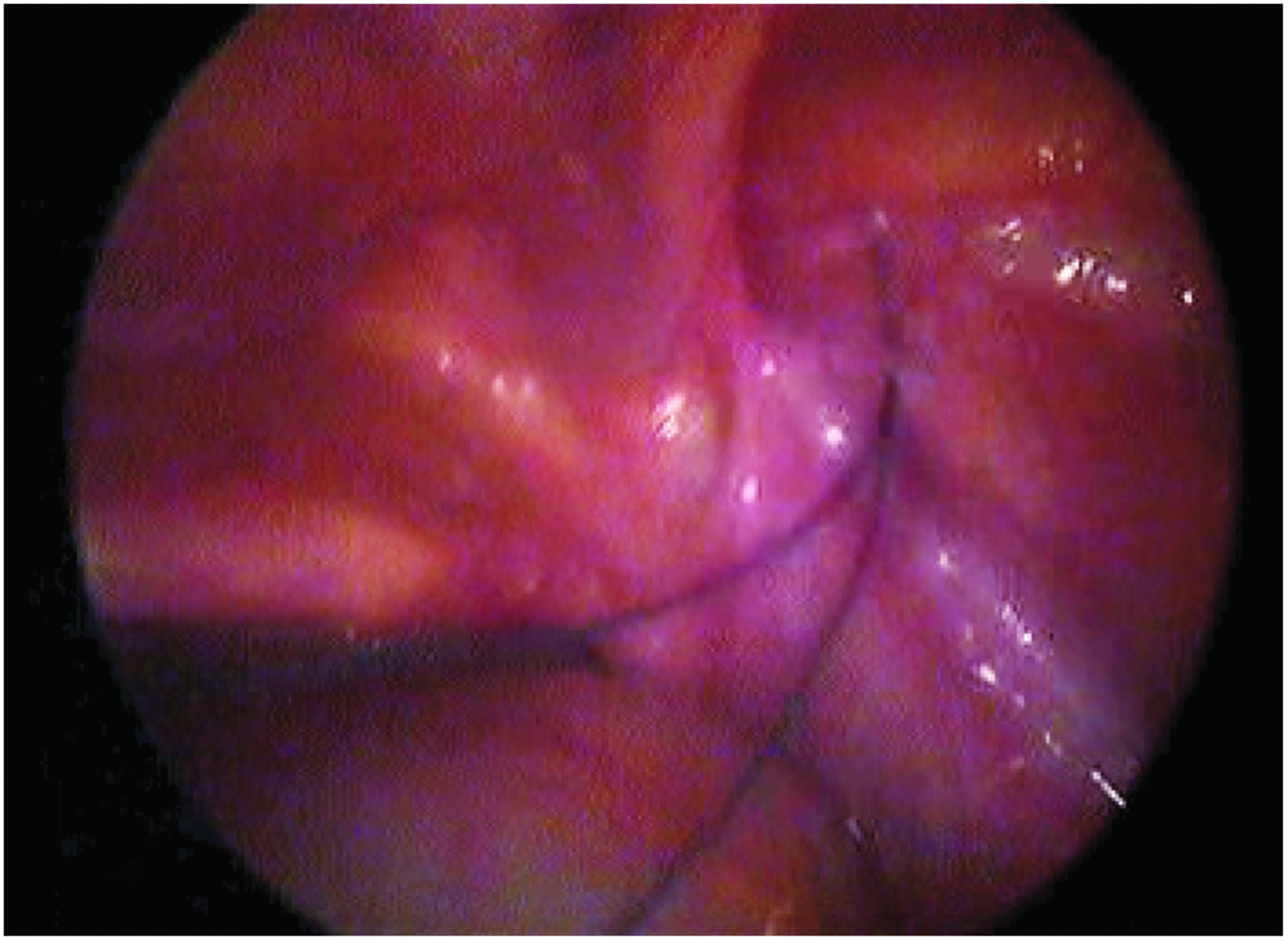
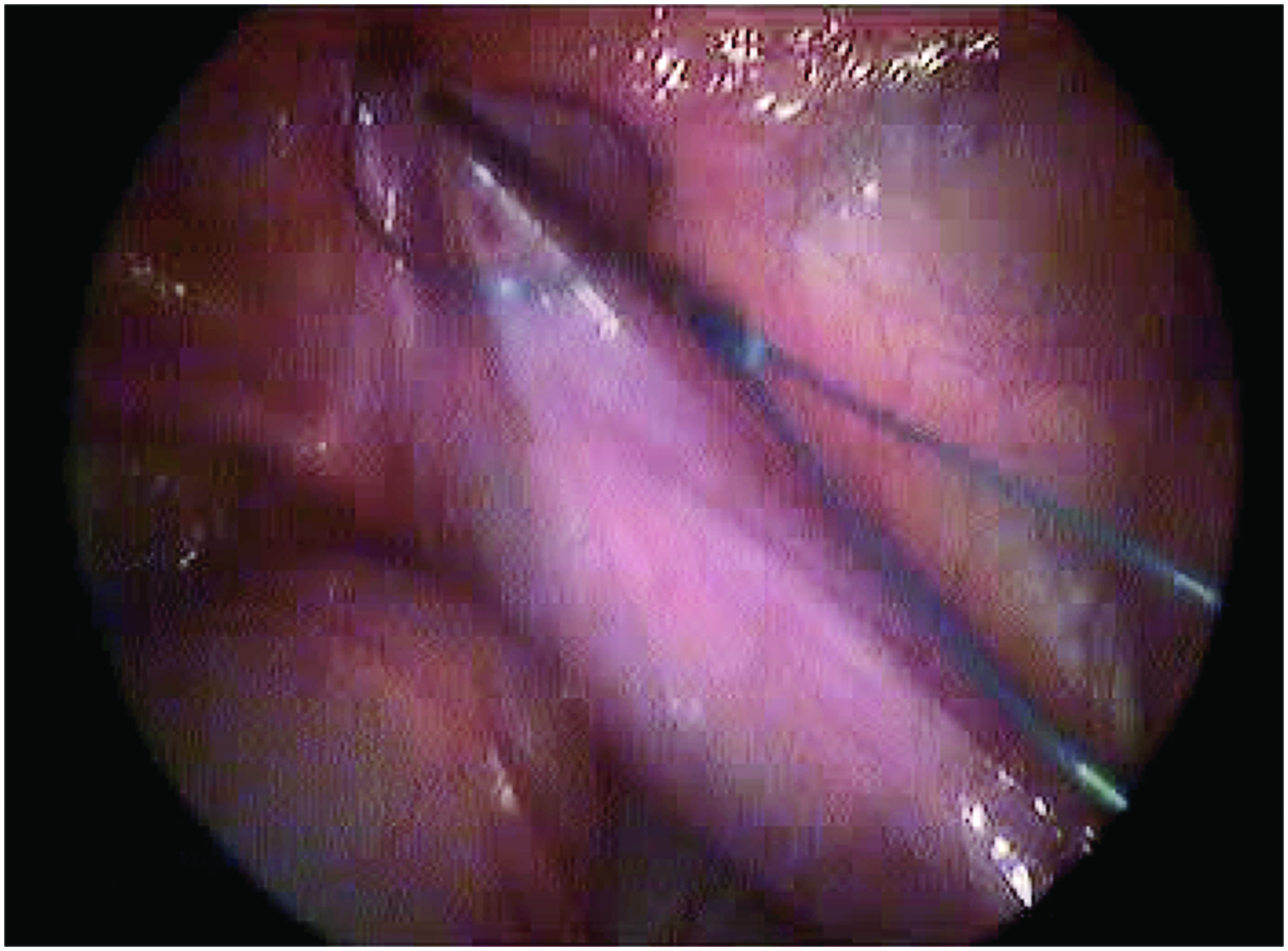
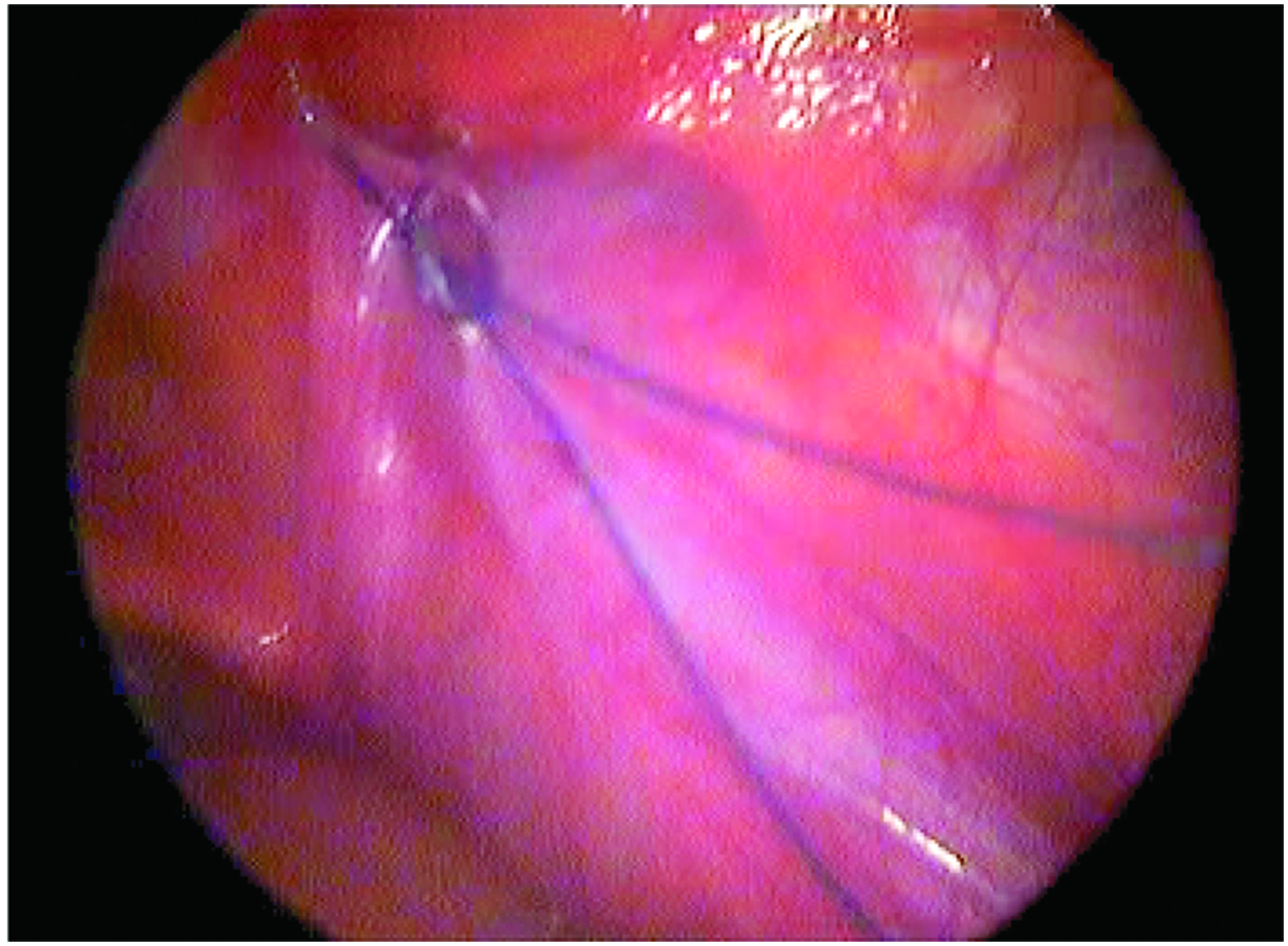
A 22G spinal needle loaded with a 2/0 or 3/0 prolene suture was introduced into the lateral border of the internal ring, a reasonable length of prolene loop was introduced into the peritoneal cavity, and the needle was withdrawn (Figs. 5–7). Another loop of prolene was introduced incorporating the medial border, while avoiding the vas and vessels, and passed through the first loop in the peritoneal cavity (Fig. 8). The first loop was then pulled out, snaring the second loop to the exterior, encircling the deep ring (Fig. 9). The second loop is exchanged with a 3/0 vicryl and then tied extracorporeally.
22G spinal needle loaded with a 2/0 or 3/0 prolene suture introduced into the lateral border of the internal ring (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).

First loop introduced through the lateral border of the internal ring (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).
The needle is withdrawn leaving the loop in the peritoneal cavity (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).
Another loop of prolene passed from the medial border avoiding the vas deferens and passed through the first loop (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).
The loop is pulled and snares the second suture through the peritoneum to the exterior, encircling the ring (intraoperative picture from Pediatric Surgery Unit, Obafemi Awolowo University Teaching Hospital Complex).
The umbilical fascia was closed with a vicryl 2/0 suture and the skin incision closed with subcuticular vicryl 3/0. The groin needle stab wound was closed with Steri-Strips™. In both groups, patients were discharged home the same day on oral analgesia (paracetamol at 10 mg/kg 8 hourly for 3 days) and seen at 5th day post op for wound inspection, then in the clinic in the following week. Subsequently, 2 weeks later, 4 weeks and 3 months follow-up were done in the outpatient clinic.
Data were recorded in a predetermined pro forma and analyzed using Statistical Package for Social Sciences (SPSS™) version 23. A P value of <.05 was considered significant.
Results
Among those that had LNAR, 1 patient required extra ports to effectively reduce the hernia as the left ovary was held down by adhesion in the inguinal canal, while a second patient was discovered to have a right undescended testis, which was missed in the clinical examination; hence, they were excluded. They however received appropriate treatments for their conditions.
Among those that had OH, 2 were lost to follow-up. Therefore, 32 patients in each arm were analyzed (Fig. 1).
A total of 64 patients completed the study, including 53 males and 11 females, with a male:female ratio of 5:1. The ages of the children ranged between 2 and 168 months with a median age of 36 months. There was no statistically significant difference between patients in the OH and the LNAR groups in terms of age, gender, and sidedness of the hernia as shown in Table 1.
Sex and Age Distribution
LNAR, laparoscopic needle assisted hernia repair; OH, open herniotomy.
Fifty-seven patients had unilateral hernias (29 had LNAR, while 28 had OH), while 7 patients had bilateral hernias (3 had LNAR, while 4 had OH) as shown in Table 2.
Duration of Surgery
LNAR, laparoscopic needle assisted hernia repair; OH, open herniotomy; SD, standard deviation.
There were a total of 17 postoperative complications irrespective of the group and the type of complication. For the LNAR group 2 complications were observed, while in the OH group 15 complications were observed. This difference was statistically significant (P = .001). The specific complications are shown in Table 3.
Postoperative Complications
LNAR, laparoscopic needle assisted hernia repair; OH, open herniotomy; SSI, surgical site infection.
Surgical site infection
One (2.9%) of the LNAR group had SSI, and 6 (16.7%) herniotomies had SSI in the OH group; however, this difference was not statistically significant (P = .058). All SSI were superficial except 1 OH that had deep SSI with associated superficial wound dehiscence and purulent discharge; this required daily wound dressing with saline and oral antibiotics. Wound healed by second intention.
Scrotal or labial edema/hematoma
Eight herniotomies in the OH group had scrotal edema at postoperative day 5 (18.8%), while none of the LNAR group has scrotal/labial edema. This difference was statistically significant (P = .005). All edema resolved spontaneously within 2 weeks postsurgery.
Postoperative hydrocele
One patient in LNAR group had postoperative hydrocele discovered at postoperative day 5. This was amenable to percutaneous aspiration alone. None of the OH group had postoperative hydrocele. This difference however was not statistically significant (P = 1.000).
Early recurrence
We also noted one recurrence at 2nd month postoperation in the OH group and none in the LNAR group (P = 1.000).
Iatrogenic undescended/ascending testis
There were no cases of iatrogenic ascending testis in both groups.
In unilateral hernias the duration of surgery was slightly lower for the LNAR group (30.6552 ± 8.28629 minutes) compared to the OH group (31.6429 ± 7.30912 minutes), but not statistically significant (P = .636). The mean surgery duration for bilateral hernias is also slightly shorter for LNAR (39.33 ± 2.31) than OH (47.25 ± 12.37), and also not statistically significant (P = .334).
Out of the 32 patients that underwent LNAR, 3 had bilateral ligation of PPV. Among these 3 patients, contralateral PPV was discovered intraoperatively in 2. They had closure of the PPV in the same sitting and were analyzed as bilateral PPV. In all, 2 (6.42%) patients had contralateral PPV discovered at laparoscopy.
Discussion
In this study, we observed that there were more patients with SSI in the OH than in the LNAR group. This is similar to findings of Bharathi et al. 16 with 5.8% in OH and 0% for laparoscopic herniotomy using similar techniques. Esposito et al. 17 reviewed several articles comparing open and laparoscopic herniotomy within a 20-year period and observed that all reported a lower rate of SSI in laparoscopy irrespective of the technique.
The prevalence of SSI for OH in this study was similar to that of Bamigbola et al. 18 in Ilorin, who observed an SSI rate of 14.6%. Usang et al. 19 in an earlier study in this institution observed a lower incidence of about 4.8%; however, their criteria for assessing SSI were limited to the presence of purulent effluent with evidence of inflammation, in contrast to this current study where we utilized the Southampton grading system, which considers the presence of nonpurulent exudate and in fact evidence of inflammation without any exudate as some form of SSI. In this study, only 1 patient (3.1%) in the OH group had purulent discharge requiring oral antibiotics and daily wound dressing.
We observed a significantly higher rate of scrotal edema in the OH group compared to LNAR group. Nazem et al., 3 Bharathi et al., 16 and Shalaby et al. 20 similarly observed that OH increases the risk of edema and hematoma in comparison to LNAR. This is explicable by the fact that more dissection is done in the OH group along the inguinal canal, while for the LNAR group no dissection in the inguinal canal. Several local and foreign studies also noted that most of the scrotal edema resolved spontaneously and significant hematoma requiring drainage was not frequent, as was also observed in this study.13,21–24
Postoperative hydrocele was noted on the 5th day in one of the patients in the LNAR group. This was amenable to sterile needle aspiration only. There were no postoperative hydroceles following OH in this study. Saha et al. 25 and Bharathi et al. 16 also noted a similar statistically insignificant higher incidence of hydrocele following LNAR than OH, and none required surgery. We thought this to be because the PPV is commonly divided and any residual hydrocele is drained following OH, whereas in LNAR, the PPV is only ligated at the deep ring; therefore, a residual hydrocele may become more evident postoperatively.
One of the patients in the OH group had recurrence within the first 2 months of follow-up, and none occurred with LNAR. Similarly Saha et al. 25 in their study noted that 1 case (3.3%) out of 30 in laparoscopic group and 2 cases (6%) out of 32 in open surgery group had developed recurrent inguinal hernia in about 1 year follow-up, while Endo et al. 1 observed a recurrence rate of 0.11% in LNAR and 0.65 in OH. Recurrence may result from failure to ligate the sac high enough at the internal ring, injury to the floor of the inguinal canal due to operative trauma, failure to close the internal ring in girls, and postoperative wound infection and hematoma. 1
In LNAR technique, the PPV is always visualized once pneumoperitoneum is created, allowing adequate ligation to be done under direct visualization. However, recurrence can occur if a significant portion of the PPV is skipped while avoiding the vas and vessels and if a rapidly absorbable suture is used.23,26 Interestingly, a meta-analysis involving 2699 children from 10 comparative studies observed that Laparoscopic techniques were associated with a trend toward higher recurrence rate when follow-up is extended for more than 6 months. 27
In keeping with the findings in most literatures, none of the patients for LNAR was converted to OH.14,16,28,29 Reasons for conversion in one study was due to anatomical variations, including direct hernias, hydrocele of the cord/canal of Nuck, difficulty to reduce the hernia, undescended testis, and suspected intersex, 30 none of which applied to the cases in this study.
Iatrogenic undescended testis did not occur in either of the groups postoperatively; this was similar to observation of Saha et al. 25 while comparing both open and laparoscopic repair. Shalaby et al., 20 comparing LNAR and OH had an incidence of 4.35% for OH and none for LNAR. In addition, Endo et al. 1 noted that OH can be associated with iatrogenic testicular retraction, while this is almost nonexistent in laparoscopic repair.
Concerning the secondary outcome variables, we observed that the operating time for both LNAR and OH was similar. This is in contrast to the findings of Shalaby et al. 20 who using similar methodology and surgical techniques noted a significantly lower operation time for LNAR. This may be due to the experience of the operating surgeon as pediatric laparoscopic surgery is still in its infancy in our environment.
The mean duration of surgery for the OH group in this study is similar to what was obtained in a number of local and foreign studies.13,21–24 Similarly, the mean duration of surgery obtained in the patients who had LNAR was similar to reports of studies by Endo et al. 1 and Nasir et al. 31 In contrast it is worthy of note that intracorporeal suturing may significantly increase surgical time, and this may be an advantage of the LNAR technique we adopted in this study.16,23
Two patients out of 31 patients planned for unilateral LNAR were observed to have a contralateral PPV at laparoscopy in this study, and repair was done in the same sitting. Alzahem 27 in a meta-analysis involving 10 previous studies noted that the incidence of contralateral PPV at laparoscopy ranges from 21% to 47% of patients initially planned for unilateral herniotomy. In addition, Esposito et al. 17 in a systematic review quoted an incidence of contralateral PPV between 19.9% and 66% from 25 studies. These are significantly higher than what was observed in this study, probably because most of them were among neonates and premature infants, who were not included in this study. 17 Nevertheless, this suggests that LNAR may be helpful in preventing a future hernia from a contralateral PPV.
The short duration of the study made it impossible to assess the long-term complications. Nevertheless the authors are following up the patients and will hopefully report long-term complications in a larger series.
Conclusion
This study has shown that LNAR offers a significant reduction in the incidence of complications especially postoperative scrotal edema/hematoma and wound infection.
The duration of surgery for LNAR is similar to that of OH for both bilateral and unilateral hernias. The study has also revealed that the incidence of contralateral PPV in the patients with unilateral inguinal hernia planned for laparoscopy is low among children in this environment.
Footnotes
Acknowledgments
The authors thank all the parents and children that participated in this study for their confidence in our ability to offer the best care using a relatively new technique. We also appreciate all the resident doctors in pediatric surgery that contributed to the success of this work.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.