
Abstract
Abstract
Background:
There is no consensus on whether lightweight mesh (LWM) is better than heavyweight mesh (HWM) in laparoscopic inguinal hernia repair (LIHR). This study aims to update the previous reviews and to analyze present randomized controlled studies comparing LWM versus HWM in LIHR systematically.
Methods:
We searched PubMed, Embase, and Cochrane Library for randomized controlled trials (RCTs), which compared LWM with HWM in adults with LIHR. All eligible data of outcomes were quantitatively analyzed using Revman 5.3 software or qualitatively described. The outcomes included chronic pain, moderate–severe chronic pain, recurrence, foreign body sensation, influence on sexual life and male fertility (pain with ejaculation, testicular pain, etc.).
Results:
We included 12 RCTs that analyzed 3092 hernias. The difference between LWM and HWM groups at any follow-up time was not significant in chronic pain and foreign body sensation. Compared with HWM group, patients in LWM group had a similar risk of postoperative moderate–severe chronic pain at 3 and 12 months follow-up, a slightly increased risk of developing moderate–severe chronic pain at >12 months follow-up (risk ratio [RR] = 3.20, 95% confidence interval [CI] 1.05–9.75, P = .04), and a higher risk of recurrence rate (RR = 2.28, 95% CI 1.17–4.44, P = .02). At long-term follow-up, the influences of LWM and HWM on sexual life and male fertility were comparable.
Conclusion:
LWMs do not show advantages in chronic pain, foreign body sensation as well as the influence on sexual life and male fertility, and may increase hernia recurrence rates for LIHR. In addition, a higher incremental cost and lower incremental effect of LWMs make conventional HWMs preferred choice for LIHR.
Introduction
Tension-free mesh repair including open and laparoscopic inguinal hernia repair (LIHR) is currently considered the criterion standard because of the lower recurrence rate.1,2 Laparoscopic tension-free hernia repair involves the transabdominal preperitoneal (TAPP) and total extraperitoneal (TEP) approaches. Both types are superior to open inguinal hernia repair for less pain, shorter recovery time plus shorter sick leave period.3–5 As an operative approach of choice, laparoscopic techniques are increasingly used in clinical practice.
Although use of laparoscopic techniques and mesh had led to less postoperative pain compared with suture techniques,3,6 chronic inguinal pain and discomfort are still reported after mesh use.7,8 Possibly because as an extraneous matter in hernia repair, mesh can stimulate the body to produce a strong inflammatory response, 9 thus resulting in chronic pain. Ten to twelve percent of people experience chronic postoperative pain,10,11 which may have a significant influence on their quality of life. As mesh repair is used widely, the focus has shifted to postoperative chronic pain from lower recurrence rates. 12 Since the body inflammatory response to biomaterials is related to the weight of the mesh, lightweight mesh (LWM) was designed to reduce the foreign body material weight. 13 Several previously published clinical studies indicated that patients had less pain after the use of LWM14–16 ; however, the results of two meta-analyses showed that the differences were not significant in early pain, recurrence, and return to work.17,18 To the best of our knowledge, the latest meta-analysis published 6 years ago found the risk of the development of chronic pain after LWM implantation to be significantly reduced. 19
In recent years, a number of studies containing large randomized controlled trials (RCTs) have been published, focusing on the outcomes of long-term follow-up.20–24 We aim to conduct an updated systematic review and meta-analysis of the present RCTs, which compare the incidence of chronic pain using LWM and heavyweight mesh (HWM) in LIHR.
Methods
Identification of trials
RCTs in which LWM was compared with HWM in adults who required laparoscopic Lichtenstein inguinal hernia repair were eligible. The RCTs should be followed up ∼3 months, reported one or more outcome that we were interested in and published in English, while no limit to the country, type of hospital, blinding, and sample size. The exclusion criteria were as follows: (1) nonprospective RCTs (reviews, case reports, cohort study, and case–control study); (2) open Lichtenstein inguinal hernia repair; (3) full text was not available; (4) duplicate of other studies; and (5) other irrelevant articles. For duplicate publications, if different outcomes that were eligible were reported, we included all of them. We defined LWM as a weight <50 g/m2.
The primary outcome was chronic pain. Chronic pain was defined as persistent pain at the site of the operation 3 months after the primary surgery that differed from the pain before the operation. 25 The secondary outcomes were moderate–severe chronic pain, recurrence, foreign body sensation, influence on sexual life and male fertility (pain with ejaculation, testicular pain, etc.). The moderate–severe chronic pain was defined as pain intensity >3 points measured using 10-point visual analog scale (VAS) or 10-point numeric rating scale.
PubMed, Embase, and the Cochrane Library were searched for literature published up to March 1, 2019. We combined the MeSH including “hernia, inguinal” and “laparoscopy” and text word search terms such as “hernias, inguinal,” “inguinal hernias,” “lightweight,” “low weight,” “low density,” and “laparoscopic surgical procedure” with AND or OR. We listed the search strategy of PubMed as an example (Supplementary Table S1). References of the included study were also retrieved for additional studies.
Two reviewers identified the studies for inclusion and exclusion independently. The conflicts were discussed to resolve, or by means of a third author to obtain a final decision.
Data extraction
Two reviewers extracted the data back to back. Disagreements were resolved through consultation. The variables extracted as follows: the author, publication year, country, study design, age, gender, intervention and control, sample size, weight and material of mesh, type of mesh fixation, follow-up time and outcome.
Risk of bias in included studies
Assessment of risk of bias in eligible studies was conducted according to Cochrane Handbook 5.1.0. 26 All eligible studies were assessed to ascertain the risk of bias for domains as follows: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other bias.
Statistical analysis
We used the software package Review Manager (Revman) current version: 5.3.5 27 for statistical analysis to gain synthesis results. The risk ratio (RR) and mean difference (MD) with 95% confidence intervals (CIs) were calculated for binary variables and continuous variables, respectively. Random or fixed-effects models were selected to calculate the synthesis results of both types of data according to heterogeneity between studies.28,29 We used the χ 2 test for the exploration of heterogeneity, and P value <.050 was considered significant. I2 was used to quantify heterogeneity. 26 The combined results were displayed using forest plots. Subgroup analysis was conducted to ascertain whether follow-up time or type of techniques influenced the overall incidence of chronic pain. Funnel plot in Revman was selected to explore the publication bias of original studies, when more than nine trials reported a certain outcome.
Results
According to Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement, 30 the literature search strategy and study selection are summarized in Figure 1. Fourth published articles14–16,20–24,31–36 on 12 RCTs,14–16,20,21,23,31–36 encompassing 3092 hernias, were analyzed systematically to gain combined results. Two articles published by Bringman et al.22,23 and Peeters et al.,24,33 respectively, were from the same trials, but with different follow-up durations and outcomes, thus, were all included. Two articles published by Bittner et al.,31,32 with different sizes of hernias and types of meshes, were identified as different publications; one 31 was marked as “Bittner 2011#” in the Revman software to distinguish with the other one. 32 Another two articles published by Langenbach et al.,35,36 but with different sample sizes, types of meshes, and follow-up times, were not repeated publications. For trials24,31,33,35,36 that had one more intervention or control groups, we combined two LWM or HWM groups into a single group recommended by Cochrane Handbook. 26 LWM and HWM groups enrolled 1493 hernias and 1599 hernias, separately. The characteristics of the included studies are shown in Table 1. Properties of meshes of each study are summarized in Table 2.
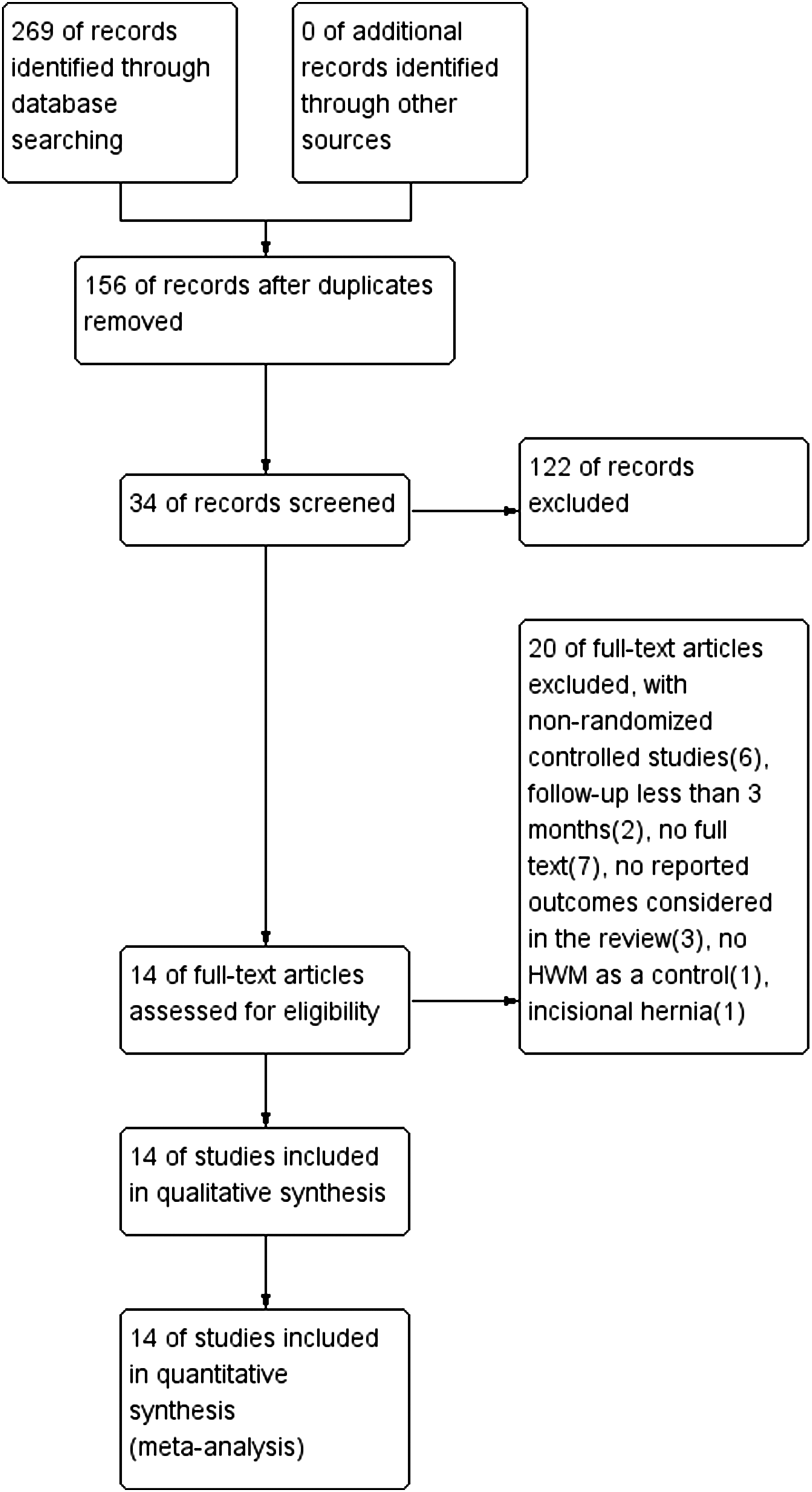
PRISMA flow chart showing study selection methodology. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Characteristics of Included Trials
F, female; HWM, heavyweight mesh; LWM, lightweight mesh; M, male; NA, not available; SD, standard deviation; TAPP, transabdominal preperitonea; TEP, total extraperitoneal.
Properties of Meshes of Included Trials
HWM, heavyweight mesh; LWM, lightweight mesh; NA, not available.
According to Cochrane Handbook (version 5.1.0), 26 risks of bias of all eligible studies are presented in Figure 2; majority of the studies are considered to be at low risk of bias in the important domains.
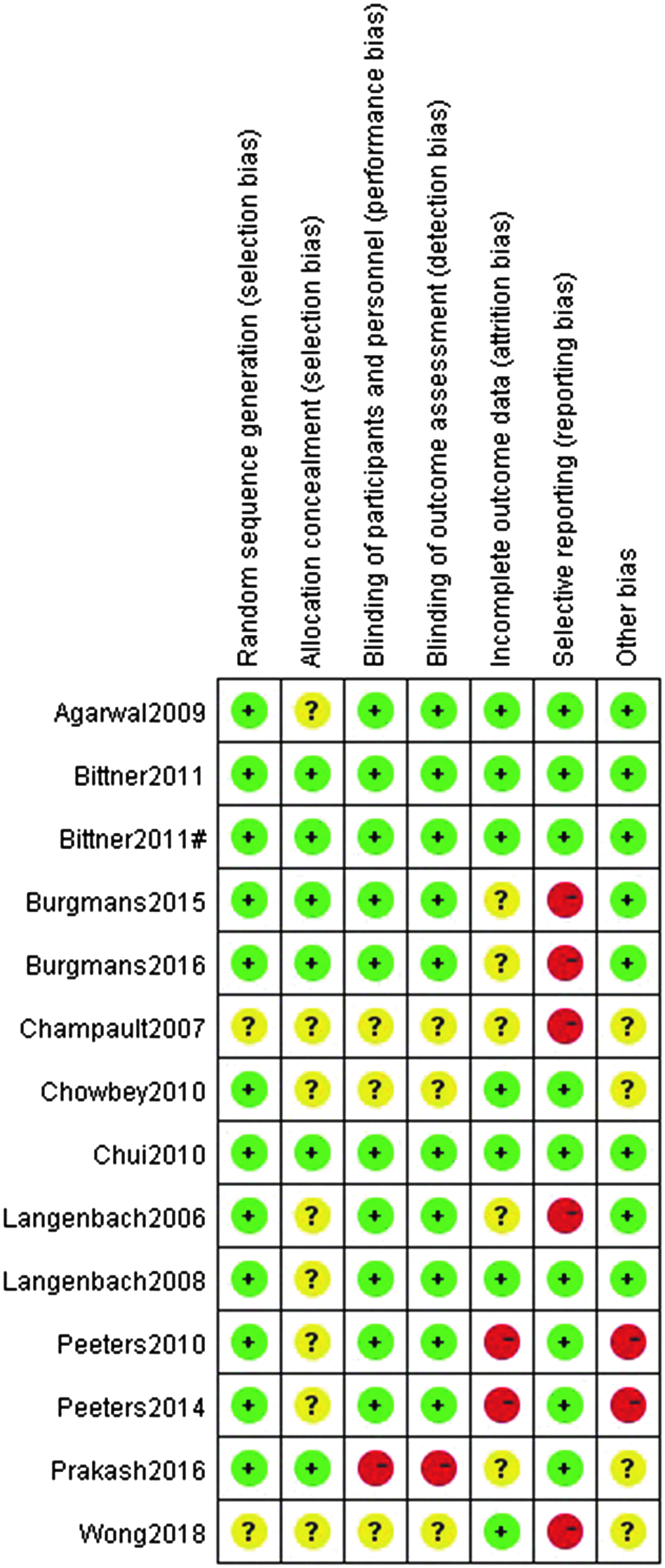
Risk of bias of included studies. Green means “low risk,” yellow means “unclear risk,” and red means “high risk.”
Results of Meta-Analysis
Chronic pain
Eleven studies14–16,20–24,31–36 reported chronic pain as an outcome; we conducted meta-analysis with different follow-up times.
Three months
Five trials15,16,21,23,34 reported chronic pain in TEP repair with 3 months follow-up time. Two trials16,23 reported the frequency of chronic pain, no significant difference between LWM group and HWM group (RR = 0.89, 95% CI 0.69–1.15, P = .38) in fixed-effects model (χ 2 = 1.73, P = .19, I2 = 42%) (Fig. 3A). Another three trials15,21,34 reported the intensity of chronic pain measured by 10-point VAS; LWM had no significant advantage over HWM (MD = −0.24, 95% CI −0.62 to 0.13, P = .21) in random-effects model (χ 2 = 7.73, P = .02, I2 = 74%) (Fig. 3B).
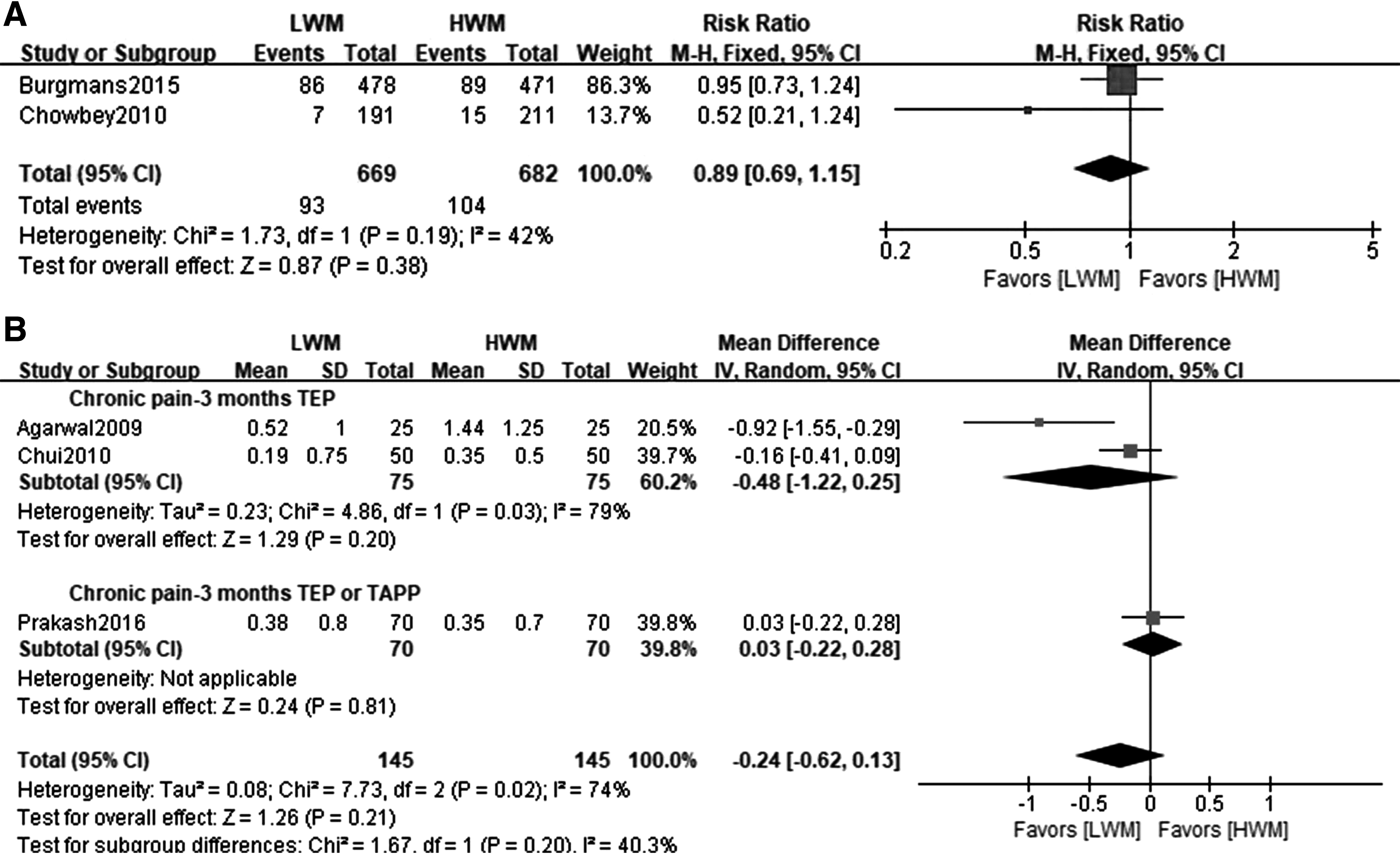
Forest plot of chronic pain at 3 months.
Six months
Four trials21,31,32,34 reported postoperative chronic pain after 6 months. Two trials31,32 reported the frequency of chronic pain in TAPP repair; there was no statistically significant difference in the incidence of chronic pain between LWM and HWM groups (RR = 0.80, 95% CI 0.45–1.42, P = .45) in fixed-effects model (χ 2 = 0.08, P = .78, I2 = 0%) (Fig. 4A). Two trials21,34 reported the intensity of chronic pain measured by 10-point VAS, showing that a higher average pain score was observed for the side of HWM compared with LWM; the difference was not significant yet (MD = −0.07, 95% CI −0.18 to 0.04, P = .22) (Fig. 4B).
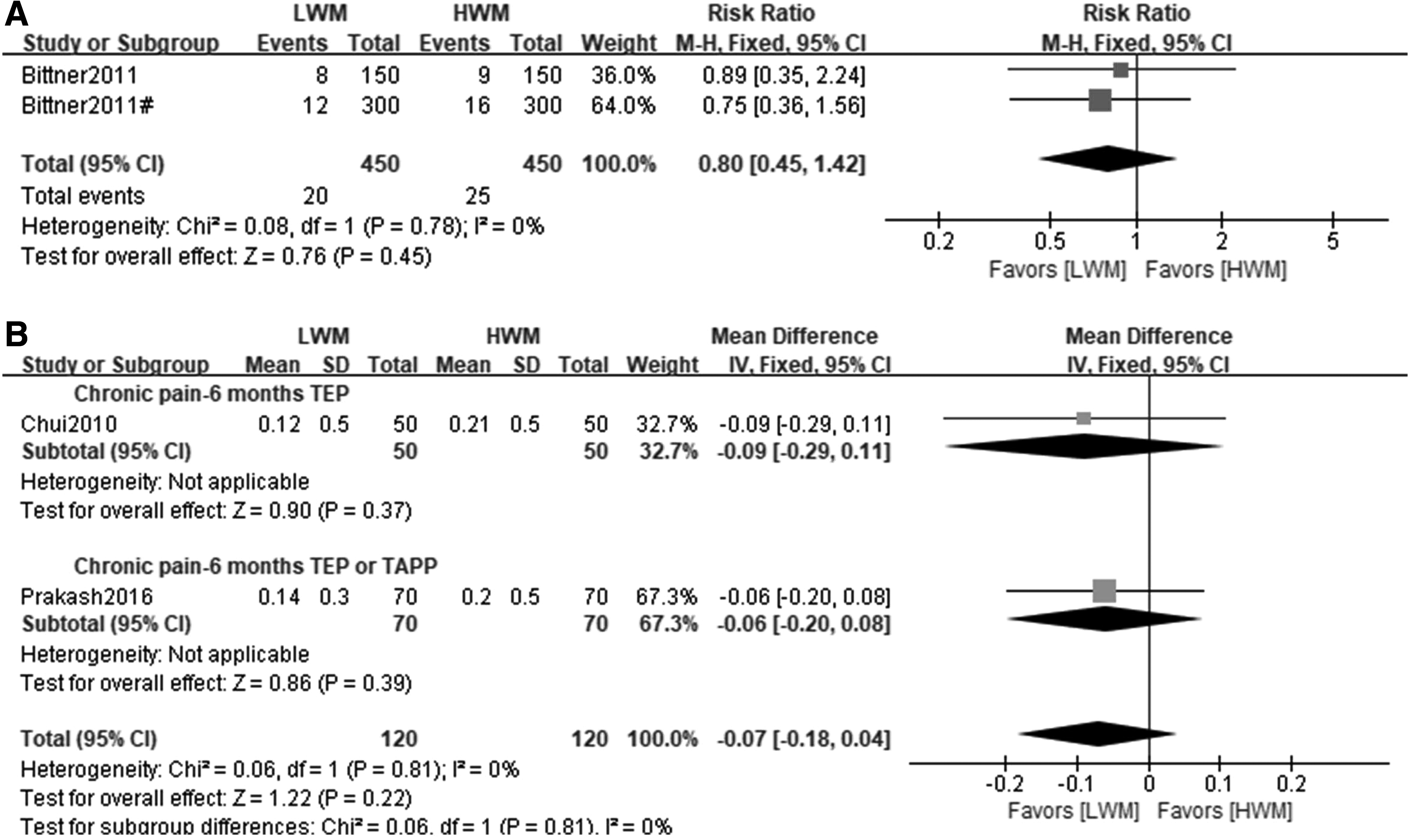
Forest plot of chronic pain at 6 months.
Twelve months
Eight studies15,16,21,22,24,31,32,34 reported the postoperative chronic pain with 12 months follow-up time. Five studies16,22,24,31,32 reported the frequency of chronic pain; compared with HWM, the use of LWM did not lower the incidence of chronic pain significantly (RR = 0.93, 95% CI 0.69–1.26, P = .66) in fixed-effects model (χ 2 = 5.27, P = .26, I2 = 24%). In the subgroup analysis, there was no significant difference in two groups for TEP repair (RR = 0.96, 95% CI 0.68–1.35, P = .82) and for TAPP (RR = 0.85, 95% CI 0.45–1.60, P = .62) (Fig. 5A). There were also three studies15,21,34 reporting the intensity of chronic pain measured by 10-point VAS in TEP. In fixed-effects model (χ 2 = 2.13, P = .34, I2 = 6%), the meta-analysis showed that HWM was not significantly better than LWM (MD = 0.02, 95% CI −0.04 to 0.08, P = .49) (Fig. 5B).
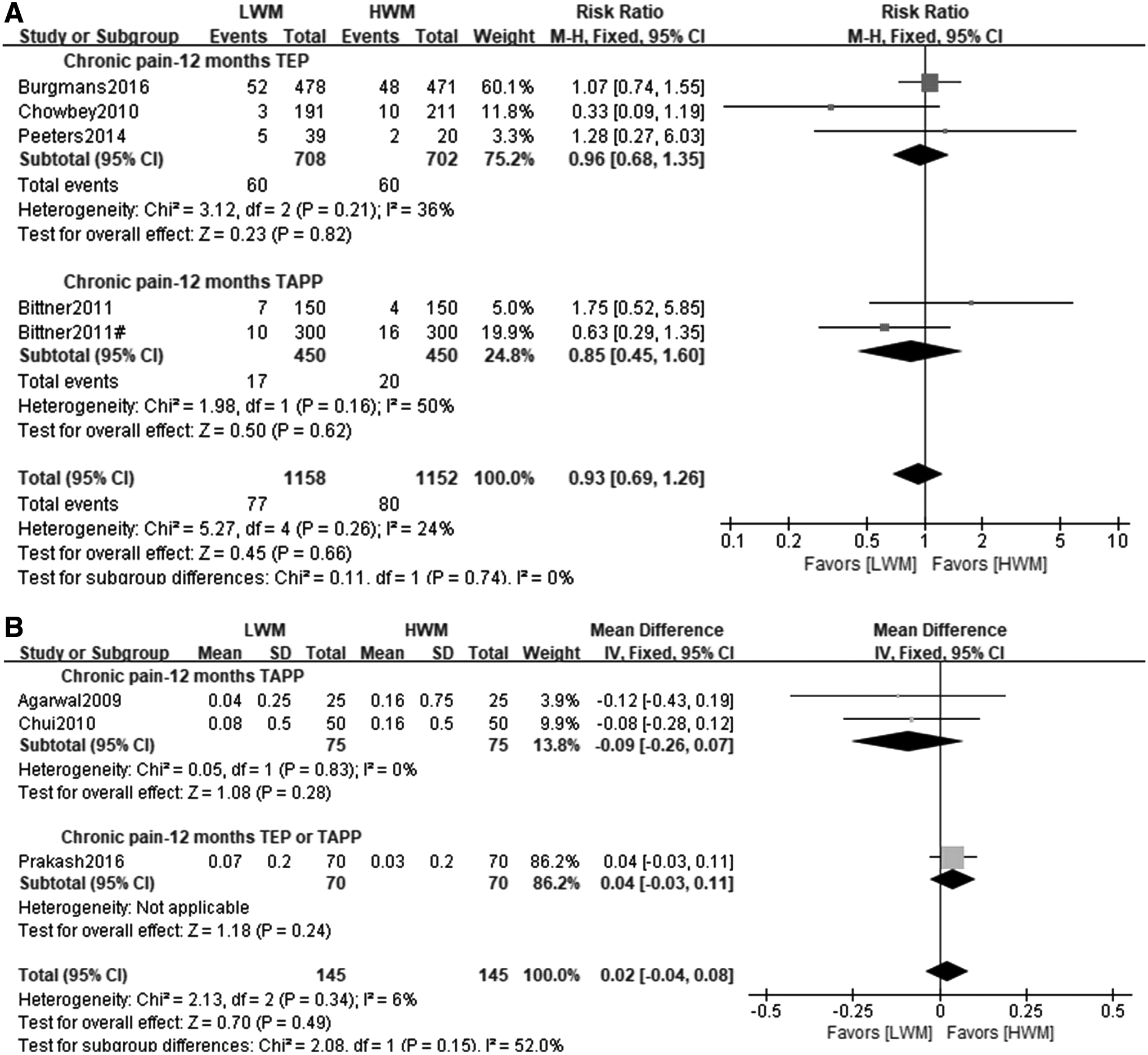
Forest plot of chronic pain at 12 months.
Over 12 months
Three studies14,22,24 reported the chronic pain with follow-up time >12 months. In random-effects model (χ 2 = 9.01, P = .01, I2 = 78%), there was no significant difference in the risk of developing chronic pain with LWM versus HWM (RR = 0.72, 95% CI 0.20–2.55, P = .61) (Fig. 6). The heterogeneity among trials disappeared while deleted in the study published by Champault et al. 14 In fixed-effects model (χ 2 = 0.06, P = .81, I2 = 0%), the difference was still not significant between LWM and HWM groups (RR = 1.35, 95% CI 0.95–1.92, P = .09).
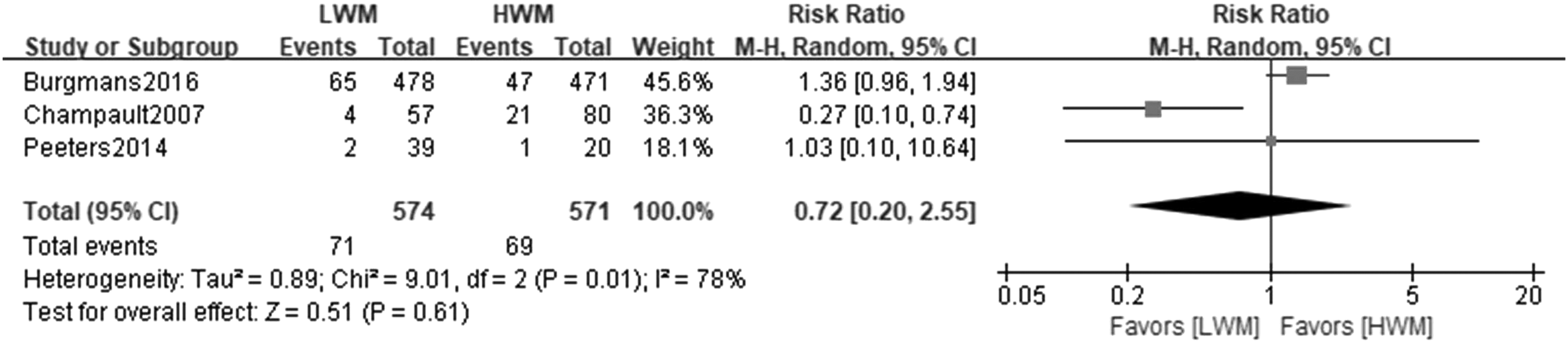
Forest plot of chronic pain (reported as frequency) at >12 months. Forest plot comparing chronic pain (reported as frequency) after the use of LWM versus HWM in laparoscopic TEP inguinal hernia repair at >12 months follow-up. A Mantel-Haenszel random-effects model was used for meta-analysis. Risk ratios are shown with 95% confidence intervals.
Moderate–severe chronic pain
Five studies16,21–23,33 reported moderate–severe chronic pain with different follow-up times. The studies involved in pooled analysis were homogeneous. According to meta-analysis of three studies, there was no significant difference in the development of chronic pain between LWM and HWM groups at 3 months (RR = 1.54, 95% CI 0.69–3.41, P = .29) and 12 months (RR = 2.56, 95% CI 0.98–6.68, P = .05) in fixed-effects model. However, at >12 months follow-up, LWM was correlated with the higher incidence of chronic pain (RR = 3.20, 95% CI 1.05–9.75, P = .04) (Supplementary Fig. S1).
Recurrence
Ten trials15,16,20–22,24,31,32,34,35 reported the hernia recurrence, but there was zero event in two trials,15,34 thus we only combined the results of eight trials16,20–22,24,31,32,35 to analyze. There was no heterogeneity among studies (χ 2 = 5.85, P = 0.56, I2 = 0%). The risk of recurrence was significantly increased in patients receiving LWM (RR = 2.28, 95% CI 1.17–4.44, P = .02). In the subgroup analysis, for TEP repair, recurrence rate in LWM group was significantly higher than that in HWM group (RR = 2.62, 95% CI 1.19–5.78, P = .02), while no significant difference was observed in two groups for TAPP repair (RR = 1.59, 95% CI 0.45–5.59, P = .47) (Supplementary Fig. S2).
Foreign body sensation
Seven studies20–23,31,32,34 reported foreign body sensation postoperation, and six studies21–23,31,32,34 can be quantitatively synthesized. At different follow-up times, there was no significant difference in the incidence of foreign body sensation between LWM and HWM groups at 3 months (RR = 0.76, 95% CI 0.39–1.45, P = .40) in random-effects model, 6 months (RR = 0.33, 95% CI 0.10–1.16, P = .08) and 12 months (RR = 1.00, 95% CI 0.73–1.39, P = .99) in fixed-effects model. In addition, there were two studies31,32 reporting the intensity of foreign body sensation measured by 100-point VAS at 12 months follow-up; the pooled analysis showed that the two groups were similar (MD = −0.14, 95% CI −0.43 to 0.14, P = .31) in fixed-effects model (χ 2 = 0.01, P = .91, I2 = 0%). The remaining study on TEP repair conducted by Wong et al. 20 also obtained similar results that there was no significant difference between LWM and HWM in postoperative foreign body sensation in different positions with 12 months follow-up time.
Influence on sexual life and male fertility
Eight trials15,21–24,33,35,36 reported outcomes regarding influence on sexual life and male fertility; the pooled analysis of two studies35,36 showed that the participants who received HWM had significantly higher incidence of pain with ejaculation (RR = 0.26, 95% CI 0.07–0.93, P = .04) compared with those receiving LWM at 3 months after operation due to TAPP repair. However, at >12 months follow-up, the difference was not significant (RR = 1.00, 95% CI 0.09–10.81, P = 1.00). Three studies21,35,36 reported testicular pain at 3 months follow-up; the meta-analysis showed that LWM was not statistically better than HWM (RR = 0.65, 95% CI 0.29–1.45, P = .29).
We conducted a descriptive analysis of three studies that could not be quantitatively synthesized. A study published by Agarwal et al. 15 showed that participants did not report any discomfort in response to sexual life outcomes at 3 months follow-up. The remaining two articles published by Burgmans et al.22,23 also reported no major differences in testicular pain and pain related to sex and discomfort between LWM group and HWM group at 3 and 24 months follow-up.
With regard to male fertility, Peeters et al.24,33 indicated that LWM could reduce sperm motility compared with HWM at 12 months follow-up (P = .013), but the difference was not significant at 3 years (unilateral, P = .99; bilateral, P = .83). There were no differences in sperm concentration between LWM group and HWM group at 12 and 36 months follow-up.
Discussion
By summarizing the results of this review, we found that the chronic pain and foreign body sensation were similar between LWM and HWM groups, at any follow-up time, in spite of the use of TEP or TAPP. LWM was related to a similar risk of postoperative moderate–severe chronic pain at 3 and 12 months follow-up, an increased risk of developing moderate–severe chronic pain at >12 months follow-up, and a higher incidence of recurrence. It was not significantly different between LWM and HWM with respect to influence on sexual life and male fertility at long-term follow-up.
A mesh is requisite in Lichenstein techniques of inguinal hernia repairs. As a common complication, chronic pain affects ∼11% of participants after mesh-based repair. 37 The factors of chronic pain may be the local tissue inflammation to the foreign material, the biological incompatibility, and the abdominal wall compliance reduction. 9 Chronic pain is still reported in some patients, even the risk appears to reduce by using LIHR. 38 Among potential causes, it was assumed that mesh weight (g/m2) may influence the occurrence of pain.39,40 HWM provides maximum mechanical stability at hernia defect, leading to the formation of stiff and nonflexible scar. 19 On the contrary, stiffness and foreign body sensations can be developed due to the excessive tensile strength. 41 The LWMs involve composite meshes containing both absorbable and nonabsorbable material and meshes containing a reduced weight of nonabsorbable components. 41 Compared with conventional HWM, the LWM has better biocompatibility, and its elasticity is similar to that of the abdominal wall. 42
Some studies14–16,43 showed that patients using LWM instead of HWM had lower incidence of chronic pain. However, several randomized trials in recent years found that it was not significantly different between the two types of meshes concerning chronic pain in LIHR.16,21,31,32,34 Furthermore, a large randomized clinical trial 22 indicated that the presence of relevant chronic pain was significantly higher after the use of LWM when compared with HWM at long-term follow-up. The results of the present review are consistent with a previous systematic review and meta-analysis 18 and the newly published literature,44–46 while inconsistent with another one, 19 which included 11 RCTs. We owe the dissimilarity to the inclusion of new studies. At >12 months follow-up, there is significant heterogeneity among studies, and heterogeneity is disappeared upon excluding the study published by Champault et al. 14 Probably because the trial enrolled recurrent hernia, while the other two trials only included primary hernia. For moderate–severe chronic pain, the result from one trial 22 conducted by Burgmans et al.22,23 is a reversal of the conventional wisdom, where LWM is associated with significantly higher incidence at >12 months follow-up. In this trial, even authors adjusted for the confounding factors (age, body mass index, operation time, surgeon, hernia type, severe preoperative pain, and recurrence), and the result remained unchanged. One explanation for the increase of chronic pain with LWMs may be that the sample sizes of previous studies were possibly too small to show a difference, because the incidences of chronic pain are low. In addition, LWMs contain less material and have larger pores, and may have insufficient strength to avoid bulging, which can create pressure that might cause pain after surgery. 22
The present review shows that the development of foreign body sensation is comparable between LWMs and HWMs at any follow-up time. This is broadly consistent with published studies. Previous concerns about the high recurrence rate of LWMs are confirmed in this review. But it is not significant in the subgroup of TAPP repair, and may be due to the sample size not being large enough to make a difference between the two groups, under the premise of low recurrence rate. This may also be why earlier systematic review 19 did not find significant difference. The reasons hernia recurrence rate is higher in LWM group may be as follows: first, low weight and large pore size of LWM, leading to the mesh-aponeurosis scar tissue formation by itself, making it difficult to achieve the desired effect for the large hernia; second, the bending strength and friction of LWM are insufficient, so it tends to migrate after implantation; third, among the inclusion of 10 studies, 3 studies16,20,22 showed more recurrence events in LWM group, in which the mesh type used was Ultrapro mesh. The absorption of poliglecaprone contained in Ultrapro mesh by hydrolysis causes a different inflammatory response, possibly impairing fibrosis formation. 47
Inflammatory response induced by the mesh may lead to dysfunction of vas deferens and spermatic vessels, because the mesh is placed in close contact to these structures in LIHR. Dysfunction of vas deferens and spermatic vessels could be troublesome in fertility and sexual life. 48 Theoretically, for reduction in foreign body reaction and better protection of the spermatic structures, the use of LWMs in LIHR could be more beneficial. 33 However, this review finds that, for the influence on sexual life and male fertility including pain with ejaculation, testicular pain, sperm motility, and sperm concentration, LWM is similar to HWM after long-term follow-up.
Compared with earlier published meta-analyses,18,19 the strength of this review is that we systematically analyze the incidence and intensity of chronic pain separately according to different follow-up times, thereby specifically presenting the results of each follow-up time point. Furthermore, as the follow-up time of most trials14–16,20–22,24,31–35 included in this review was ∼12 months, long-term effects of LWMs versus HWMs on patients can be obtained. One limitation of this review is that the inclusion and exclusion criteria among included RCTs were not completely uniform, such as the gender, types of hernias, and size of hernias. In addition, the mesh fixation techniques used in eligible trials were versatile, which may consider to have potential influence on pain score, because mesh fixation was likely to be an important risk factor for the development of chronic pain. 32
Conclusions
LWMs do not show advantages in chronic pain, foreign body sensation as well as influence on sexual life and male fertility, and may increase hernia recurrence rates for LIHR. In addition, compared with conventional HWMs, LWMs induce higher incremental costs and inferior incremental effect on the basis of cost–utility analysis. These results indicate that there is no benefit for LWMs and conventional HWMs are preferred choice for LIHR. More large and high-quality trials are necessary to validate these findings.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.