
Abstract
Abstract
Background:
The incidence of trocar site hernia (TSH) in single-port laparoscopic cholecystectomy (SPC) is still a debated issue. Aim of this retrospective study was to compare the incidence of postoperative hernia and cosmetic results among patients undergoing SPC and multiport laparoscopic cholecystectomy (MPC) performed at a single institution.
Methods:
A series of 60 SPC and 60 MPC patients operated on between July 2016 and May 2018 were compared. Primary endpoint was to assess the incidence of TSH at long term. All the patients were admitted as outpatients for physical examination and scar measurement. Secondary endpoints were the cosmetic results assessed by a cosmesis score (CS) and the body image questionnaire (BIQ).
Results:
After a median 18-month follow-up (range: 6–29 months), a hernia in umbilical trocar site was detected in 4 (7.1%) SPC patients and 1 (2%) MPC patient, the difference not being statistically significant (P = .216). BIQ was almost equivalent in SPC and MPC groups (5.15 versus 5.27; P = .518), respectively. Statistically significant differences in favor of SPC were found in CS (22.3 versus 19.72; P = .001) and in total length of scars (1.2 cm versus 4 cm; P < .001).
Conclusions:
SPC technique has proved to be safe and effective in experienced hands. Superior cosmesis of SPC over MPC is confirmed, but close attention to fascial closure is a vital component of SPC, and surgeons performing single-site surgery need to be aware of this increased potential for hernia formation.
Introduction
To minimize the number of skin incisions and ports required and to enhance the benefit of the laparoscopic approach, in recent years surgeons have developed the use of single-incision laparoscopic surgery. Single-incision laparoscopic cholecystectomy was first described in 1995 by Navarra et al. 1 in a report of 30 patients with favorable outcomes.
It is recognized that single-port laparoscopic surgery requires a larger fascial incision than traditional multiport laparoscopy. This need can imply a potentially increased risk of surgical-site complications, such as herniation. In recent randomized trials, the incidence of hernia varies from 1.3% to 8.4%.2–4
However, these multicentric studies often combine experiences and techniques that are not always identical. They have no long-term follow-up and a number of cases per center that sometimes does not reach the number fixed by the learning curve. These drawbacks can partially explain the wide range of results. As for the cosmetic aspect, the most recent randomized controlled trials (RCTs) report a significantly higher cosmetic benefit of single-port laparoscopic cholecystectomy (SPC) than for multiport laparoscopic cholecystectomy (MPC).5–7 Nevertheless, it must be said that there is an extreme variability of the devices used for single-port surgery. This can affect both the fascial and skin incision with possible consequences on cosmesis and on parietal closure. In our retrospective study, we wanted to evaluate the impact of the Unimax Medical Systems single-port device by comparing the long-term incidence of trocar site hernia (TSH) and by assessing the cosmetic aspect between a group of MPC patients and a group of SPC patients.
Materials and Methods
Since the introduction of the single-port technique in our department in October 2016, all the SPCs and MPCs were registered consecutively in a prospective database. To obtain the number of 60 laparoscopic cholecystectomies per group, 15 MPCs performed before October 2016 were added to the study group.
Ultimately, 120 patients underwent MPCs and SPCs between July 2016 and May 2018. Patients' characteristics included patient age, gender, body mass index (BMI), previous abdominal surgery, and associated comorbidities. Patients with symptomatic gallbladder stones were included. Acute cholecystitis and chronic cholecystitis were not considered a contraindication to SPC and, therefore, included in the study. The procedure outcome parameters such as duration of surgery, hospital stay, and morbidity (according to Clavien–Dindo classification) were also collected. Between November and December 2018, the patients were contacted and visited on an outpatient basis. At the visit, a clinical examination to detect the presence of a TSH was carried out; a measure of the scars' length was made as well. In case of clinical doubt, an ultrasonography was performed. Patient satisfaction with cosmesis and body image were assessed by means of the validated cosmesis score (CS, ranging from 3 to 24, with a higher score indicating a greater degree of satisfaction with the scar) and the body image questionnaire (BIQ, ranging from 5 to 20 points, with a low score signifying better body image). 8 Fourteen patients from the whole group were lost to follow-up. Eight patients could not be contacted, 3 patients declined, and 3 patients were already deceased. Ultimately 106 patients (88.3%) attended the follow-up examination, 56 in the SPC group and 50 in the MPC group.
SPC technique
The four-channel single-port system (Single port; Unimax Medical Systems, Inc., Taipei, Taiwan) (Fig. 1) is inserted through a 2-cm fascial incision in the umbilicus. After creation of pneumoperitoneum, a 5-mm 30° angle telescope is introduced. One transabdominal stay suture is passed in the fundus and used for transcutaneous retraction of the gallbladder. In case of a really long gallbladder, an additional suture is passed into the infundibulum. This suture allows a “puppeteering technique” for mobilization of the infundibulum, enabling complete visualization of Calot's triangle by suture traction. 9
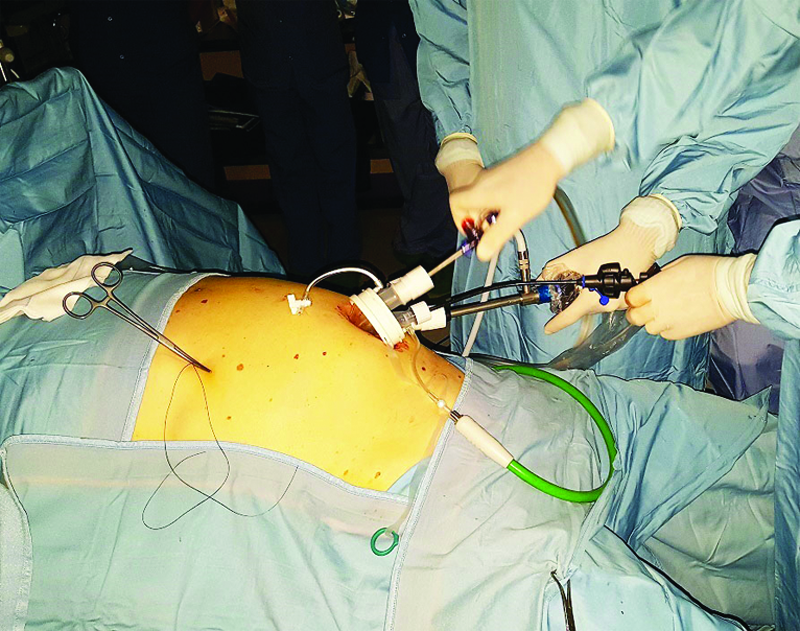
Intraoperative view. The four-channel Unimax single-port positioned at the umbilicus for a laparoscopic procedure.
Dissection is conducted with a reusable 5-mm laparoscopic hook and a 5-mm reusable prebent grasper (Olympus Medical Systems, Hamburg, Germany). The cystic artery and duct are isolated after the “critical view of safety” principles, closed with clips (10 mm Endoclip®; Microfrance, Saint Aubin le Monial, France), and divided by reusable scissors. No specimen retrieval bag is used as the Unimax device already acts as a wound protector.
MPC technique
We performed standard laparoscopic cholecystectomy in accordance to the American technique. 10
The pneumoperitoneum is achieved through the umbilicus by an open technique; a 10-mm trocar is inserted to accommodate a 30° angle telescope. Another 10-mm trocar is inserted into the epigastrium, which is the main right working port for the surgeon. One 5-mm trocar in the right lumbar region is used for gallbladder fundus traction and another 5-mm trocar is used in the right midclavicular line, below the costal margin for the surgeon's grasper. All the instruments are reusable like in the SPC. After following surgical steps identical to SPC, the gallbladder is placed in a disposable sterile bag and extracted from the umbilical port.
Statistical analysis
Correlations were assessed by the Spearman rank correlation coefficient. Comparisons between groups were carried out by the nonparametric Mann–Whitney U test for continuous variables and by the chi square test for binary variables. A P value <.05 was considered statistically significant.
A logistic regression model was used to identify variables affecting the probability of TSH occurrence in univariate analysis. All parameters with a P value <.05 at univariate analysis were included in a multivariate model through a backward selection procedure to evaluate potential independent predictors for TSH occurrence. Statistical analysis was performed using the software package SPSS Version 13.0 (SPSS, Inc., Chicago, IL).
Results
SPC and MPC patients did not differ significantly regarding age, gender, BMI, and comorbidity (Table 1). In both groups, patients were overweight and 11 (27.5%) SPC patients and 7 (14%) MPC patients had a BMI >30 kg/m2 (P = .444). Duration of surgery was longer in the SPC group (78.8 ± 30.6 minutes versus 67.5 ± 22.2; P = .094). Length of hospitalization was significantly shorter for patients operated on by SPC than patients operated on by MPC (P = .007). Postoperative complication rates were 10.7% in the SPC group and 6% in the MPC group (P = .2). In both groups, mostly minor complications such as fever as only symptom (4 SPC patients and 1 MPC patient) and one prolonged abdominal pain were experienced. All complications except for 1 SPC patient were classified as Clavien class I that was managed conservatively. In this case, the patient needed reoperation through a laparotomy to manage a bile leak from the liver bed.
Characteristics of Patients and Postoperative Results Grouped for Laparoscopic Procedure
Values are meant as median (SD) unless indicated otherwise.
BMI, body mass index; MPC, multiport laparoscopic cholecystectomy; SD, standard deviation; SPC, single-port laparoscopic cholecystectomy.
After a median follow-up of 16 months (range: 6–25 months) for the SPC group and 20 months (range: 6–29 months) for the MPC group, the clinical data of patients were collected through physical examination and questionnaires (Table 2). Of the whole group, 106 (88.3%) patients attended the follow-up examination. A hernia in the umbilical trocar site was detected in 4 (7.1%) SPC patients and 1 (2%) MPC patient, the difference not being statistically significant (P = .216).
Long-Term Clinical Data of Patients Grouped for Laparoscopic Procedure
Values are meant as median (SD) unless indicated otherwise.
BIQ, body image questionnaire; CS, cosmesis score; MPC, multiport laparoscopic cholecystectomy; SD, standard deviation; SPC, single-port laparoscopic cholecystectomy; TSH, trocar site hernia.
All hernias were of small dimensions and the parietal defect was measured between 2 and 3 cm in diameter. Only in 1 SPC patient, the hernia was symptomatic and was treated 14 months after cholecystectomy. The other patients who came to visit were unaware of having a TSH. An ultrasonography was performed in only 1 case of SPC that confirmed the presence of incisional hernia. Two patients reoperated, the first for incisional hernia and the second for a bile leak, were not evaluated cosmetically. All patients called to follow-up visit completed the BIQ and CS questionnaires.
BIQ score was 5.15 (range: 4–7) in SPC patients and 5.27 (range: 5–7) in MPC patients. CS was 22.3 (range: 10–24) in SPC patients and 19.72 (range: 12–24) in MPC patients, the difference being statistically significant (P = .001). A significant difference was found in the total length of scars between SPC and MPC groups (1.2 cm; range: 0–2.5 cm versus 4 cm; range: 3–6 cm; P < .001). Clinical parameters able to influence the occurrence of TSH such as gender, age, BMI, and associated comorbidities were analyzed in both groups, but no significant correlation was found.
Discussion
In this study, the preliminary long-term results of a prospective study regarding TSH occurrence and cosmesis of SPC compared with traditional MPC have been represented.
Median length of follow-up is longer in the MPC group. Anyway, a 16-month follow-up in the SPC group is judged sufficient. Hernia develops in the first year in 50% of patients, and in 25% of these patients, hernia develops only after 2 years. A TSH can be diagnosed as such only after ∼12 months.11,12
All RCTs report an extremely variable rate of incisional hernia. In the first RCT released in 2013, Marks et al. 3 reported a significant difference in TSH occurrence in favor of MPC (1.2% versus 8.4%; P = .03) and concluded by doubting the use of this approach given the high rate of hernia formation. However, just the following year, Jorgensen et al. 4 reported a 2% recurrence rate, identical for both groups. In the multicenter RCT conducted on 600 patients (MUSIC trial) by Arezzo et al., 2 a 1.3% TSH rate was reported in the SPC versus 0.6% in the MPC. The authors conclude by saying that the incidence of incisional hernia was so low in both groups that many more cases would be needed to achieve significance if confirmed. In our study, similarly to what is reported in the literature, TSH rate favors multiport over single-port technique, even if the difference is not significant (2% versus 7.1%; P = .216).
Marks et al. 3 stated that incisional adverse events, calculated with a Fisher's exact test, were the only variable shown to be a predictor of port-site hernia occurrence. More recent studies failed to find parameters able to affect TSH occurrence.4,5,13
It is well known that obesity is a risk factor for the occurrence of ventral/incisional hernia and leads to higher recurrence rates and perioperative-related complications. 14 In our study, although the population examined in both groups was overweight, the obese patients in the SPC group were in proportion more than double compared with the MPC patients. Moreover, of the 4 SPC patients who developed a TSH, 2 were obese with a BMI >34 kg/m2 and 1 was overweight (BMI = 27.3 kg/m2). Given the low incidence of TSH, very large casuistries are needed to find potential predictive parameters. In fact, in our study the univariate analysis did not find predictive factors of TSH occurrence.
About the subject of TSH, the definitive word is still far from being said. Indeed Haueter et al. in a meta-analysis comprising 35 RCTs and a total of 3051 patients concluded that only 3 of the 37 included trials had an overall low risk of bias. 15 Shortcomings of the RCTs include small number of patients in most of the trials (20–50 patients per group), which sometimes do not reach the number fixed by the learning curve. Another problem is the high rate of patients lost to follow-up and its brevity. Only eight studies reported a follow-up of 1 year or longer.
In addition to this, we believe that a poorly addressed critical aspect is that these multicentric studies combine experiences and techniques that are not always identical. Sakran et al. describe a hybrid technique with three conventional trocars through a single 15 mm umbilical incision and a single 2–3 mm epigastric port. 16 Dapri et al. use three conventional trocars through a single umbilical skin incision, but in three different fascial incisions. 17 Moreover, most surgeons use multichannel single-port systems especially built for single-port use but of very different shapes and sizes.
Technical aspects such as trocar size, trocar type, trocar placement technique, fascia closure, and, importantly, the type of sutures used may influence the formation of trocar-associated hernias.18,19
Although there is still uncertainty on the TSH subject, evidence on cosmesis already exists and has been exposed in the European Association for Endoscopic Surgery guidelines. 20 If a patient is looking for better cosmesis, SPC could be preferred to conventional four-port laparoscopic cholecystectomy. Unfortunately, the grade of recommendation of this statement is still weak. Our study showed similar BIQ and superior CS for the SPC group compared with the MPC group after a median 18-month follow-up. The BIQ score measures the patients' perception of their body as well as their attitude toward their appearance. Although this attitude appears to be similar in the two groups, patients' satisfaction with respect to the appearance of their scars significantly favors SPC over MPC. This can be explained by the difference in the length of the scars at follow-up, which is decidedly lower in the case of the SPC than MPC. Indeed, this is also due to the fact that in many SPC patients, the umbilical incision was no longer visible. Our results are similar to the study of Lurje et al. 5 that evaluated cosmesis at 1 year, which gave superiority to SPC with regard to CS and scar length, but also to BIQ. The esthetic aspect is not to be overlooked because it is connected to pain perception. In fact, scar length is proportional to postoperative pain. This is now confirmed by most studies that give SPC an advantage in postoperative pain.6,21
In conclusion, although our study has the merit of homogeneity with regard to the instrumentation used and the technique adopted, it has some drawbacks. The shortcomings of this study are the relatively small number of patients and its nonrandomized character. SPC technique has proved to be safe and effective in experienced hands, representing a valid alternative to the traditional four-port laparoscopic cholecystectomy for the treatment of symptomatic cholelithiasis. Superior cosmesis of SPC over MPC is confirmed, but close attention to fascial closure is a vital component of SPC, and surgeons performing single-site surgery need to be aware of this increased potential for hernia formation.
Authors' Contributions
All authors were responsible for the drafting of the article, analysis, and interpretation of data, and critical revision of the article for important intellectual content. The study was approved by all authors in the present format.
Footnotes
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.