
Abstract
Objective:
To summarize and analyze the technique and experience of laparoscopic liver resection (LLR) in children.
Methods:
From Dec 2015 to Dec 2018, surgical outcomes were evaluated in 30 pediatric patients with liver tumors. LLR was performed in 21 patients, including 15 males and 6 females with a mean age of 7.6 ± 3.8 years (range, 2–13 years) and a mean liver tumor diameter of 7.2 ± 2.0 cm (range, 4–10 cm). During the same period, 9 cases of traditional open liver resection were selected as controls, including 6 males and 3 females with a mean age of 7.0 ± 3.7 years (range, 2–13 years) and a mean liver tumor diameter of 7.5 ± 2.2 cm (range, 4.4–10.0 cm).
Results:
The mean operation time and mean hepatic inflow occlusion time were longer in the laparoscopic group, with values of 182.3 ± 66.1 minutes and 83.2 ± 38.2 minutes, respectively, than in the open group, with values of 120.0 ± 54.3 minutes and 49.6 ± 26.5 minutes, respectively. There were no significant differences between the two groups in blood loss (164.4 ± 107.4 mL versus 133.8 ± 87.1 mL), blood transfusion volume (102.2 ± 100.2 mL versus 69.2 ± 81.8 mL), and alanine aminotransferase levels 24 hours after surgery (212.0 ± 101.4 IU/L versus 173.3 ± 97.2 IU/L) and 72 hours after surgery (74.0 ± 32.5 IU/L versus 81.7 ± 57.3 IU/L). The average hospital stay in the laparoscopic group (6.2 ± 1.6 days) was significantly shorter than that in the open group (8.2 ± 2.0 days). The children in both groups recovered well after surgery without serious complications.
Conclusion:
LLR contributes to improved recovery of patients after surgery without increasing the incidence of complication, therefore, LLR is a safe option for liver tumors in children.
Introduction
Along with the development of laparoscopic techniques and improvements in surgical equipment, adult laparoscopic hepatectomy has developed rapidly in recent years and has achieved good results.1–3 Currently, although a wide variety of pediatric surgical diseases are treated with laparoscopy, laparoscopic liver resection (LLR) has not been widely performed in children, which may be due to the low incidence of liver tumors in children and the small number of pediatric liver surgeons.4,5 Due to the difficulty of LLR and physiological characteristics of children, there are only a few published literature introducing pediatric LLR experiences.6–8 These studies have reported that LLR is a viable option for benign liver disease, primary malignancy, and metastatic liver disease.
The following report summarizes 21 cases of LLR performed recently in the Department of Pediatric Surgery of West China Hospital, Sichuan University. The aim is to share our experience with LLR in the pediatric population.
Clinical Data and Methods
General information
From August 2016 to December 2018, 21 cases of LLR in children were performed in the Department of Pediatric Surgery, West China Hospital, Sichuan University. Patients included in the study met the following criteria: older than 1 year of age, tumor diameter no more than 10 cm, distance from the first and second porta hepatis >3 cm, and no invasion of important hepatic vessels and bile ducts. The exclusion criteria were as follows: (1) difficulty in tolerating pneumoperitoneum; (2) poor circulation and respiratory function; (3) intra-abdominal adhesions especially in surgical field affecting view or operation, and the presence of any contraindication to open liver resection (OLR). The selection of the operation method was based on the willing of the parents who were completely informed of the potential risks and benefits.
In laparoscopic group, there were 15 males and 6 females with a mean age of 7.6 ± 3.8 years (range, 2–13 years) and a mean liver tumor diameter of 7.2 ± 2.0 cm (range, 4.0–10.0 cm). Left hepatectomy was performed in 5 patients, left lateral hepatic lobectomy was performed in 6 patients, and nonanatomic hepatectomy was performed in 10 patients. During the same period, 9 cases of traditional OLR were selected as controls, which included 6 males and 3 females with a mean age of 7.0 ± 3.7 years (range, 2–13 years) and a mean liver tumor diameter of 7.5 ± 2.2 cm (range, 4.4–10.0 cm). Three patients underwent left hepatectomy, 2 patients underwent left lateral hepatic lobectomy, and 4 patients underwent nonanatomic hepatectomy.
Preoperative preparation and surgical methods
A comprehensive assessment of the patient's general condition was carried out to evaluate the function of important organs such as the heart, lung, liver, and kidney and to determine the presence or absence of any surgical contraindications. During all laparoscopic hepatectomy procedures, the surgeon should be well prepared for conversion to laparotomy. Before the procedure, color Doppler ultrasound, enhanced computed tomography, and magnetic resonance imaging were used to carefully evaluate and make a preliminary determination of the size, nature, location, and anatomical relationship of the tumor with important tissue structures.
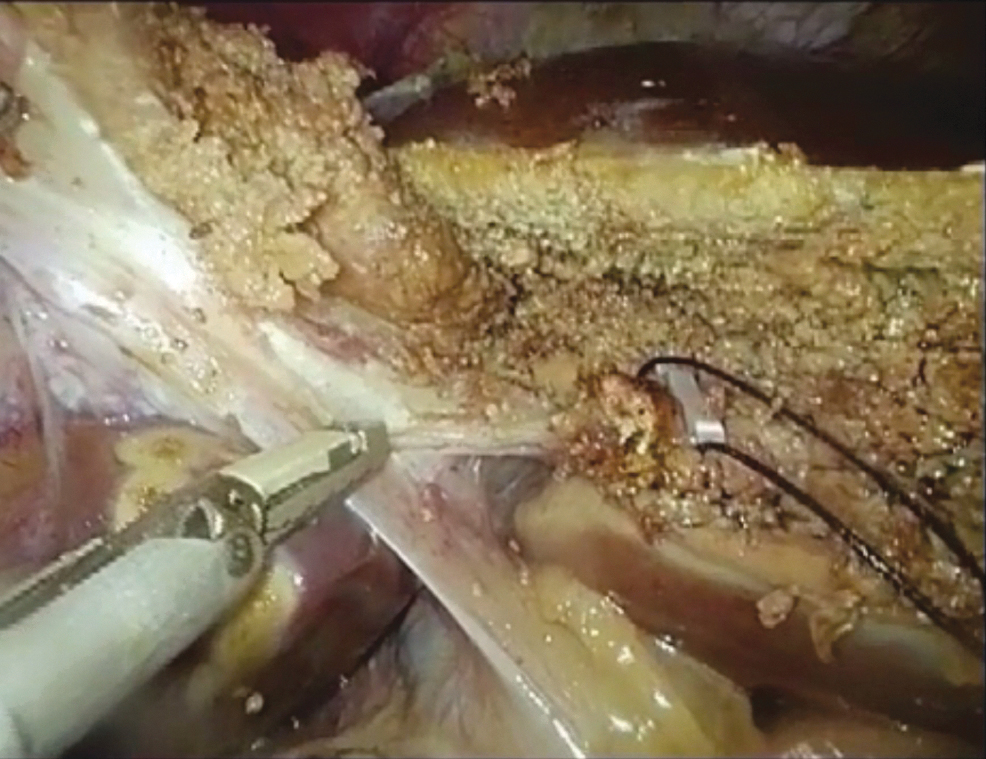
The pneumoperitoneum pressure was maintained between 6 and 12 mmHg depending on the age of the child. During the operation, an ultrasonic scalpel (Ethicon Endo-Surgery), LigaSure (Covidien), and a laparoscopic cavitron ultrasonic surgical aspirator (CUSA; Integra) were used to precisely resect the tumor. The ultrasonic scalpel was used to directly sever ducts with a diameter smaller than 2 mm. A titanium clip or synthetic clip was used to clamp ducts with a diameter between 2 and 5 mm before they were severed. A linear cutter stapler was used to cut off important ducts with a diameter larger than 5 mm. Surgical forceps can also be used to isolate the hepatic parenchyma by bluntly compressing small regions using the fine clamping method to fully expose and then cut the small intrahepatic ducts. An occlusion band was routinely placed in the first porta hepatis, and total hepatic inflow occlusion was performed in some cases. For the left hepatectomy (Fig. 1), the left porta hepatis was dissected as completely as possible to perform selective occlusion.
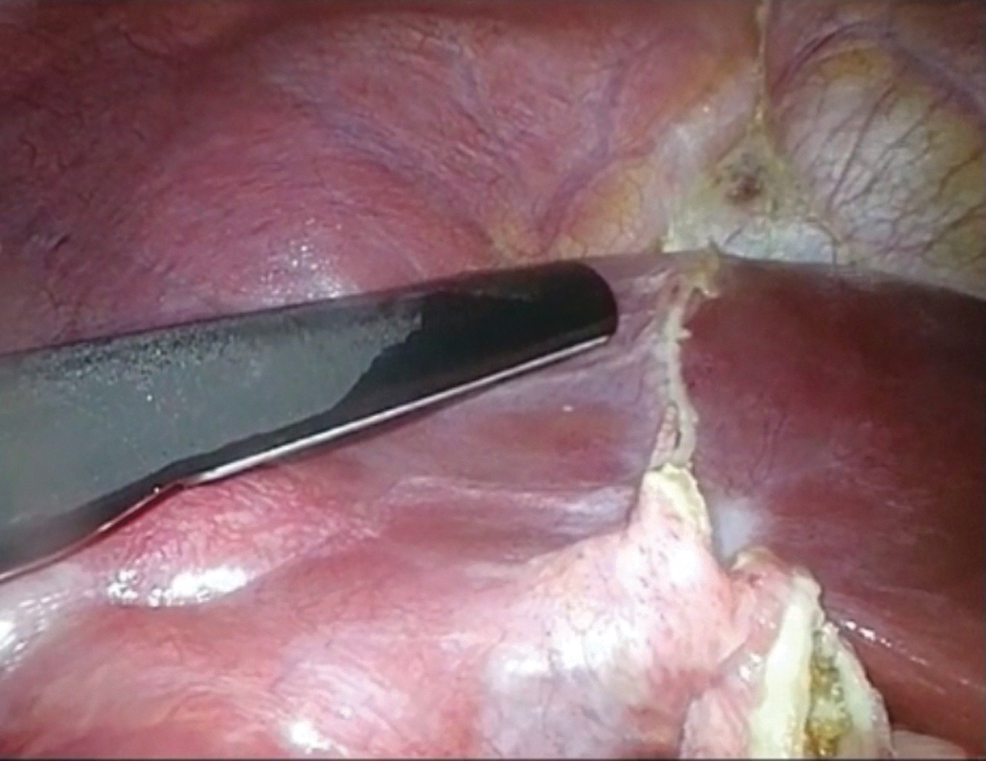
Using intraoperative ultrasound to assist in determining the tumor boundary.
When the relationship between tumor boundaries and blood vessels or bile ducts was difficult to judge, intraoperative ultrasound (Fig. 2) and intraoperative indocyanine green (ICG; Karl Storz Endoskope, Germany) fluorescence imaging techniques were used to assist in determining the tumor boundary and its anatomical relationship with important ducts and their paths as well as to explore the presence or absence of tumor residue and the blood supply to the residual liver after the resection of the lesion.
Dissecting the left porta hepatis with ultrasonic scalpel.
After resection of the lesion, a transverse abdominal incision of 5–8 cm was made in the lower abdomen, and the lesion was wrapped in a retrieval bag and removed through the incision (Fig. 3 and Fig. 4).

The surgical ports and abdominal incision.
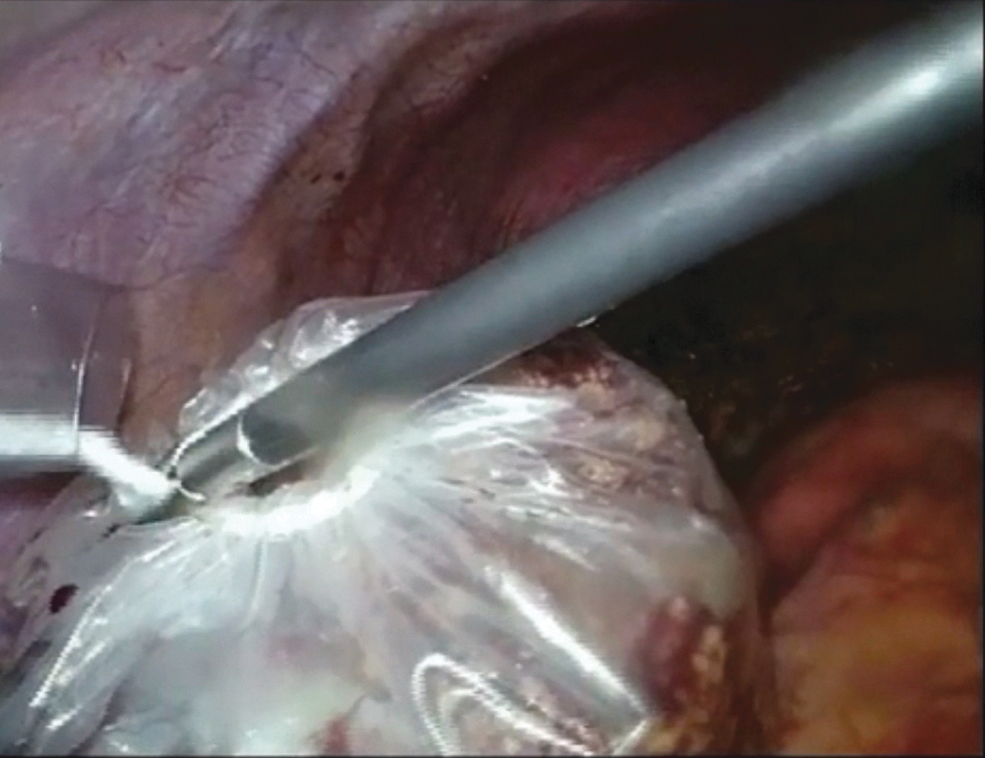
The lesion was wrapped in a retrieval bag and removed through the abdominal incision.
Prevention of complications and postoperative monitoring
During the operation, we tried our best to avoid damaging the hepatic vein and other large vessels so that the risk of vascular air embolism and tumor thrombus could be reduced. The application of specimen bags was also an effective method to reduce the incidence of tumor implantation and metastasis. During and after surgery, we paid attention to the presence of bile leakage. Strict tumor-free surgical techniques were also applied to prevent intraoperative implantation of the tumor. After the surgery, the vital signs of the patient and the nature and quantity of drainage materials were closely monitored to maintain fluid, electrolyte, and acid-base balance. Liver function was tested 24 and 72 hours after the surgery.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 statistical software. Mann–Whitney U test was used. P < .05 was considered statistically significant.
Results
There was no significant difference in age, body weight, tumor diameter, and Child-Pugh score between the two groups. The mean operation time and mean hepatic inflow occlusion time were longer in the LLR group, with values of 182.3 ± 66.1 minutes (range, 60–300 minutes) and 83.2 ± 38.2 minutes (range, 0–130 minutes), respectively, than in the OLR group, with values of 120.0 ± 54.3 minutes (range, 60–200 minutes) and 49.6 ± 26.5 minutes (range, 0–80 minutes), respectively; the differences were statistically significant (P < .05).
The mean blood loss and mean blood transfusion volumes were 164.4 ± 107.4 mL (range, 20–300 mL) and 102.2 ± 100.2 mL (range, 0–200 mL), respectively, in the LLR group, and 133.8 ± 87.1 mL (range, 50–300 mL) and 69.2 ± 81.8 mL (range, 0–200 mL), respectively, in the OLR group; there were no significant differences between the two groups (P > .05). Total bilirubin did not increase significantly after surgery in either group. The mean values of alanine aminotransferase at 24 and 72 hours after surgery were 212.0 ± 101.4 IU/L and 74.0 ± 32.5 IU/L, respectively, in the LLR group, and 173.3 ± 97.2 IU/L and 81.7 ± 57.3 IU/L, respectively, in the OLR group; the differences between the two groups were not statistically significant (P > .05). The mean hospital stay in the LLR group (6.2 ± 1.6 days [range, 5–10 days]) was shorter than that in the OLR group (8.2 ± 2.0 days [range, 6–12 days]), and the difference was statistically significant (P < .05).
Both groups of children recovered well after surgery, and there was no occurrence of abdominal bleeding, gas embolism, liver insufficiency, bile leakage, abdominal infection, lung infection, or other complications. The postoperative pathological diagnosis confirmed 9 cases of hepatoblastoma, 4 cases of focal nodular hyperplasia of the liver, 2 cases of hepatocellular carcinoma, 2 cases of hepatic echinococcosis, 1 case of undifferentiated embryonal sarcoma, 1 case of hemangioendothelioma, 1 case of inflammatory myofibroblastic tumor, and 1 case of hamartoma. There were 7 cases of hepatoblastoma, 1 case of focal nodular hyperplasia of the liver, 1 case of hepatic echinococcosis in the OLR group.
Children whose tumor was greater than 5 cm in diameter and confirmed as hepatoblastoma or liver cancer by postoperative pathology received 3–6 courses of transarterial chemoembolization postoperatively via the femoral artery, depending on the size and nature of the tumor. Both groups of patients were followed up for a period of 8 months–2 years, and no liver tumor recurrence was observed. Table 1 presents the surgical results of the two groups.
Comparison of Surgical Results of the Two Groups
P < .05.
LLR, laparoscopic group; OLR, open group.
Discussion
Since Reich et al. first reported on the laparoscopic resection of benign liver lesions in 1991, hepatobiliary surgeons have actively and cautiously explored laparoscopic hepatectomy. 9 Recently, advances in laparoscopic surgical techniques and laparoscopic equipment have led to the rapid development of LLR for adult liver surgery. However, because the liver has an abundant blood supply, the risk of surgical bleeding is high. Visualization of the liver under laparoscopy is difficult, and laparotomy techniques such as suturing are difficult to use, particularly in pediatric patients. At present, no studies on a large number of cases of laparoscopic hepatectomy in children have been reported.
The number of cases in this study is small, but valuable data have been obtained. There are only a few cases of liver tumors in children suitable for laparoscopic surgery. Hepatoblastoma is the most common primary liver malignancy in childhood, accounting for ∼50%–60% of primary liver malignancies in children, with an incidence of ∼1.2–1.5 per million.10–12 However, hepatoblastoma is mostly atypical in the early stage of the disease, and early cases are difficult to detect. At our center, ∼30 patients with pediatric hepatoblastoma are admitted and treated each year; half of these patients have hepatoblastomas that are surgically resectable, and only a few are suitable for laparoscopic resection.
The safety of the operation requires the surgeon to be familiar with the anatomy, careful operation, and full preparation for conversing to open approach. We have summarized experience of applying some of the surgical techniques and safety considerations. The surgical methods for LLR primarily include total laparoscopic hepatectomy and hand-assisted laparoscopic hepatectomy (HALH). 13 The surgeon can choose the technique based on his or her proficiency and the location and size of the liver tumor. One patient in our study underwent HALH, which greatly reduced the difficulty of the operation and accelerated the speed of the procedure. Laparoscopic anatomic hepatectomy is used whenever possible for the resection of liver lesions 14 ; in this technique, the hepatic inflow and outflow vessels are dissected, isolated, and occluded before the transection of the hepatic parenchyma. Laparoscopic nonanatomic hepatectomy can be used for lesions at the edge of the liver. Exposure of the lesion during LLR is critical. Pediatric patients, and especially infants, have a small abdominal volume; thus, the pneumoperitoneum pressure cannot be too high. Our experience is that the pneumoperitoneum pressure should be set at 6–7 mmHg at the beginning of the operation finishing the initial operation such as separation of perihepatic ligaments. When the liver is cut during surgery, the mesentery and the intestinal tract may be distended, and the abdominal cavity space may be further reduced due to longer hepatic inflow occlusion. At this time, the pneumoperitoneum pressure may be appropriately increased; it can be increased to 8–10 mmHg for infants. An abdominal wall retractor can also be used to help expose the lesion, expand the field of view, and complete the procedure as quickly as possible.
The method used for controlling bleeding during laparoscopic hepatectomy is an important consideration. To our experience, the administration of inflow occlusion is safe in pediatric patients although it may cause concerns of ischemic change in the remnant liver. If the lesion is located at the junction of the right and left lobes, hepatic inflow occlusion can be used, but the duration of each occlusion should not be very long. If the lesion is located in the left or right lobe, hemihepatic vascular occlusion is generally used. Laparoscopic hemostasis is difficult, and blood tends to fill the entire field of view or contaminate the lens; thus, effective prevention of bleeding is critical.15,16 Before the operation, the images should be thoroughly reviewed, to determine the resection plane avoiding the damage of adjacent major vascular structures. Also, advanced auxiliary diagnostic techniques can be used whenever possible. 17
Compared to open resection allowing palpation of the liver to determine margins, laparoscopic ultrasound can confirm resectability intraoperatively. ICG fluorescence imaging techniques can also be used to accurately predict the extent of the lesion to be resected and the vessels that need to be treated. The various hepatic ducts should be treated with precision during surgery, and the central venous pressure should be maintained between 4 and 6 cm H2O when the liver is resected to reduce blood reflux of the hepatic vein. Gas embolism cannot be ignored in LLR18,19; once it occurs, the mortality rate is extremely high. Therefore, care should be taken when dissecting the second porta hepatis to avoid tearing the hepatic vein or inferior vena cava. When the large venous branches of the liver parenchyma are severed, they should be handled carefully and clamped in a timely manner. In this study, there was no significant difference in the mean intraoperative blood loss and mean blood transfusion volume between the laparoscopic group and the laparotomy group.
Laparoscopic transection of liver parenchyma achieves essentially the same outcome as laparotomy, but requires the surgeons to exercise greater caution. At present, commonly used hepatectomy devices include the laparoscopic ultrasonic scalpel, water-jet scalpel, LigaSure, and CUSA. First, surgical forceps can be used to gently clamp the liver tissue in small sections. After crushing the liver parenchymal cells, the duct tissue is clearly exposed, and then titanium clips can be used for clamping. When the tumor is close to the hepatic portal or important large vessels and bile ducts, the laparoscopic CUSA can be used to carefully separate the tissues around the ducts before treatment. The hepatic transection time and the hepatic portal occlusion time were longer in the LLR group than in the OLR group. However, there were no significant differences between groups in the postoperative change in alanine aminotransferase levels and the time for gastrointestinal function recovery. The average hospital stay in the LLR group was shorter than that in the OLR group.
As mentioned above, laparoscopic surgery was not significantly different from open surgery in terms of bleeding and complications. Moreover, this procedure offers the advantages of faster postoperative recovery, milder pain, and more aesthetic incision compared with laparotomy.20,21 In conclusion, LLR contributes to improved recovery of patients after surgery without increasing the incidence of complication, therefore, LLR is a safe option for liver tumors in children.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
National Natural Science Foundation of China. Grant number 81571473.