
Abstract
Purpose:
The aim of this study was to compare the perioperative and postoperative respiratory complications between laryngeal mask (LM) airway and tracheal intubation (TI) in children undergoing percutaneous internal ring suturing (PIRS) for inguinal hernia.
Patients and Methods:
From October 2015 to February 2019, 135 pediatric patients (97 males and 38 females) with median age of 4 years, who underwent PIRS for inguinal hernia, were included in study. Patients were divided in two groups. In group I (n = 94) LM airway was used, and in group II (n = 41) TI was performed. Demographic data, surgical and anesthesia times, American Society of Anesthesiologists (ASA) classification, muscle relaxation, level of pneumoperitoneum, and complications of anesthesia were compared between the groups.
Results:
No significant differences among compared groups regarding age (P = .435), sex (P = .306), body mass index (P = .548), ASA classification (P = .506), level of pneumoperitoneum (P = .968), and duration of surgery (P = .968) were found. Duration of anesthesia was significantly shorter when LM was used compared to TI (25 minutes versus 36 minutes; P < .00001). During recovery from anesthesia, the incidences of desaturation (n = 1 versus n = 5; P = .003), laryngospasm (n = 2 versus n = 5; P = .015), and cough (n = 0 versus n = 4; P = .002) were significantly lower when LM airway was used for securing of the airway. Postoperative incidences of sore throat (P = .543), bronchospasm (P = .128), and aspiration (P = .128) did not differ between LM and TI.
Conclusions:
The use of LM in pediatric anesthesia results in a decrease in a number of common complications and significantly shortened patient anesthesia time. It is therefore a valuable device for the management of the pediatric airway for laparoscopic hernia repair in children.
Introduction
Inguinal hernia repair remains one of the most common surgeries in pediatric patients. 1 All inguinal hernias have to be treated surgically because they can lead to serious complications.1,2 After introduction of percutaneous internal ring suturing (PIRS) for inguinal hernia repair this technique gained popularity among pediatric surgeons. 3 The main goal of this technique is percutaneous closure of the internal inguinal ring using a laparoscope through the umbilical port.2–4
With regard to delivering pediatric anesthesia, appropriate airway management is its most important dimension. The anesthesia for the surgery is usually induced through tracheal intubation (TI) or laryngeal mask (LM) airway. Due to the high frequency of the procedure, it is of utmost importance to manage the airway in a way that would lead to as least number of unwanted effects as possible. Regardless of the patient's age, surgical procedures can be performed with face mask, LM, or endotracheal tube placement. 5 Endotracheal tubes are considered to be more appropriate for premature infants and neonates when maintaining general anesthesia due to a greater difficulty of providing effective face mask ventilation and the danger of air entering the stomach.5,6
There is still debate in the literature regarding the advantages and disadvantages of LM and TI concerning the occurrence of respiratory complications. 7 New evidence suggests that as the LM is not placed in the trachea, its use is associated with a fewer number of bronchospasms, laryngospasms, coughing, and sore throat than a tracheal tube.5–8 Furthermore, the LM is shown as being particularly useful as a temporizing measure in patients with difficult airways due to its ease of insertion and high success rate. 8 In recent years new less-invasive laparoscopic techniques for the inguinal hernia repair in pediatric population have been introduced. Significantly shorter surgical times and very low insufflation pressures and also shorter duration of anesthesia have led to a review of the need for TI and muscle relaxants in pediatric patients.6–9
The aim of this study was to compare the perioperative and postoperative respiratory complications between LM airway and TI in pediatric patients undergoing PIRS for inguinal hernia.
Patients and Methods
Patients
All patients who underwent PIRS for inguinal hernia at the Department of Pediatric Surgery of the University Hospital of Split in the period from October 2015 to February 2019 were enrolled in this prospective cohort study. Study protocol was approved by the ethics committee of our hospital. Inclusion criteria were patients of both genders, up to 17 years of age, with an inguinal hernia treated by the PIRS, and followed up at least 4 weeks after surgery. Exclusion criteria were as follows: patients older than 17 years of age, conversion to open procedure, patients operated in another institution and followed up at our outpatient clinic, history of allergy to anesthetics, terminal or any immunosuppressive illnesses, and patients with incomplete data.
Study protocol
All surgeries were performed on a day surgery basis. Medical history and demographic data (age, gender, body mass index [BMI], and lateralization of hernia) were taken and recorded in study protocol. Regarding the type of anesthesia the patients were divided into two distinct groups. In Group I (n = 91) LM was used, and in Group II (n = 34) TI was performed. The type of anesthesia (LM or TI) was based on anesthesiologist's preference. Surgical and anesthesia times, American Society of Anesthesiologists (ASA) classification, muscle relaxation, level of pneumoperitoneum, and complications of anesthesia were recorded and compared between investigated groups.
Postoperative follow-up included pain level, postoperative complications, and length of hospital stay. Surgical time was defined from first incision to last skin suture, and anesthesia time was defined from insertion of peripheral intravenous line to extubation/removal of LM. The patients were followed up at our outpatient clinic at the seventh postoperative day and fourth week after surgery for detection of any complications. Physical examination was performed 6 months after surgery to assess the presence of late complications or recurrence of the hernia.
Outcome measures
The primary outcomes were intraoperative desaturation, postoperative laryngospasm, and cough. Laryngospasm was defined as the sustained closure of the vocal cords resulting in the partial or complete loss of the patient's airway. Cough was considered as complication if its duration was longer than 1 hour after extubation/removal of LM. A value of oxygen saturation of less than 90% was typically considered as significant desaturation. To determine superiority of one airway management technique, consistent and significant differences between the groups in all outcome measures were expected. The secondary outcomes were postoperative bronchospasm, sore throat, and aspiration.
Surgery
A pneumoperitoneum was achieved using Veress needle through 3 mm supraumbilical incision. A level of pneumoperitoneum was set at 6–10 mmHg, depending on patient's age and weight. A 3-mm laparoscope was used in all of the patients. After identification of open internal inguinal ring on the side of hernia, skin incision of 2 mm was performed in optimal position in inguinal region. A 20G spinal needle was used for introduction of a nonabsorbable polypropylene loop (PROLENE™ 3-0, Ethicon®; Johnson & Johnson, Waluj, Aurangabad, India) at one side of the internal ring. After introduction of the loop into the abdominal cavity the needle was pulled out leaving the loop into abdominal cavity.
Through the same skin incision but on the other side of the ring, the same needle was introduced to abdominal cavity passing through the previously introduced loop, and the nonabsorbable monofilament polypropylene 3-0 suture was passed through the needle, taking care not to damage surrounding structures (spermatic blood vessels, deferent duct, epigastric or iliac blood vessels). After removal of the needle the loop was withdrawn and the suture was caught and pulled out through the skin incision. The suture was tied and after tying of the suture the internal ring was completely closed. In case if internal ring was not obliterated completely suture was removed and the same procedure was repeated. Successful repair was defined if complete occlusion of the hernia was performed. Umbilical and inguinal incisions were closed using braided adhesive sterile strips.
Anesthesiology
For all of the patients, general anesthesia was induced through TI or LM. No muscle relaxant was used.
LM introduction
Adequate mask size is critical to a good placement, so the biggest size that can be placed in the oral cavity is used. An intravenous pathway is established after attaining sufficient anesthetic depth before the LM (Solus; Intersurgical Ltd., Berkshire, UK) is inserted because it can precipitate laryngospasm. It is pushed down along the palatopharyngeal curve until the person holding the LM can feel resistance. The next step is to inflate the cuff to the pressure that allows ventilation to 20 cm H2O, forming an effective seal.
Tracheal intubation
The tracheal tube (Curity; Covidien, Mansfield) is introduced using the laryngoscope in the standard anesthesia method. Choosing the size for children younger than 10 years is governed by the formula: size = age/4 + 4. Tube position is also checked by auscultation of both chest and abdomen to make sure that both lungs are equally ventilated. Endotracheal tube is secured with 2 pieces of 5 to 10 mm long adhesive band placed on the entrance of oral cavity and around the tube.
Statistical analysis
The corresponding data were obtained by revising the study protocols and medical records. The data were analyzed using SPSS 24.0 (IBM Corp., Armonk, NY) software programs. Distributions of quantitative data were described by medians and interquartile ranges (IQRs), whereas absolute rates and percentages were used to describe categorical data. Differences in median values of quantitative variables between the groups of patients were tested with Mann–Whitney U test. The chi-square test was used for the statistical analysis of the categorical data. All values of P < .05 were considered to indicate statistical significance.
Results
During the study period 135 PIRS procedures for inguinal hernia repair were performed in total. LM was used in 94 children (70%), while in the remaining 41 children (30%) TI was used. Both the clinical and demographic data are summarized in Table 1. The median age for patients in LM group was 4 years (IQR 2, 7 years) and for the intubated patients the median age was 3.5 years (IQR 1, 6 years). No statistically significant differences between the investigated groups in regards to age (P = .435), gender (P = .306), BMI (P = .548), ASA classification (P = .506), level of pneumoperitoneum (P = .968), and duration of surgery (P = .968) were found. Duration of anesthesia was significantly shorter in LM group with the median time of 25 minutes (IQR 20, 30) compared to 36 minutes (IQR 28, 45) in TI group (P < .00001) (Fig. 1).
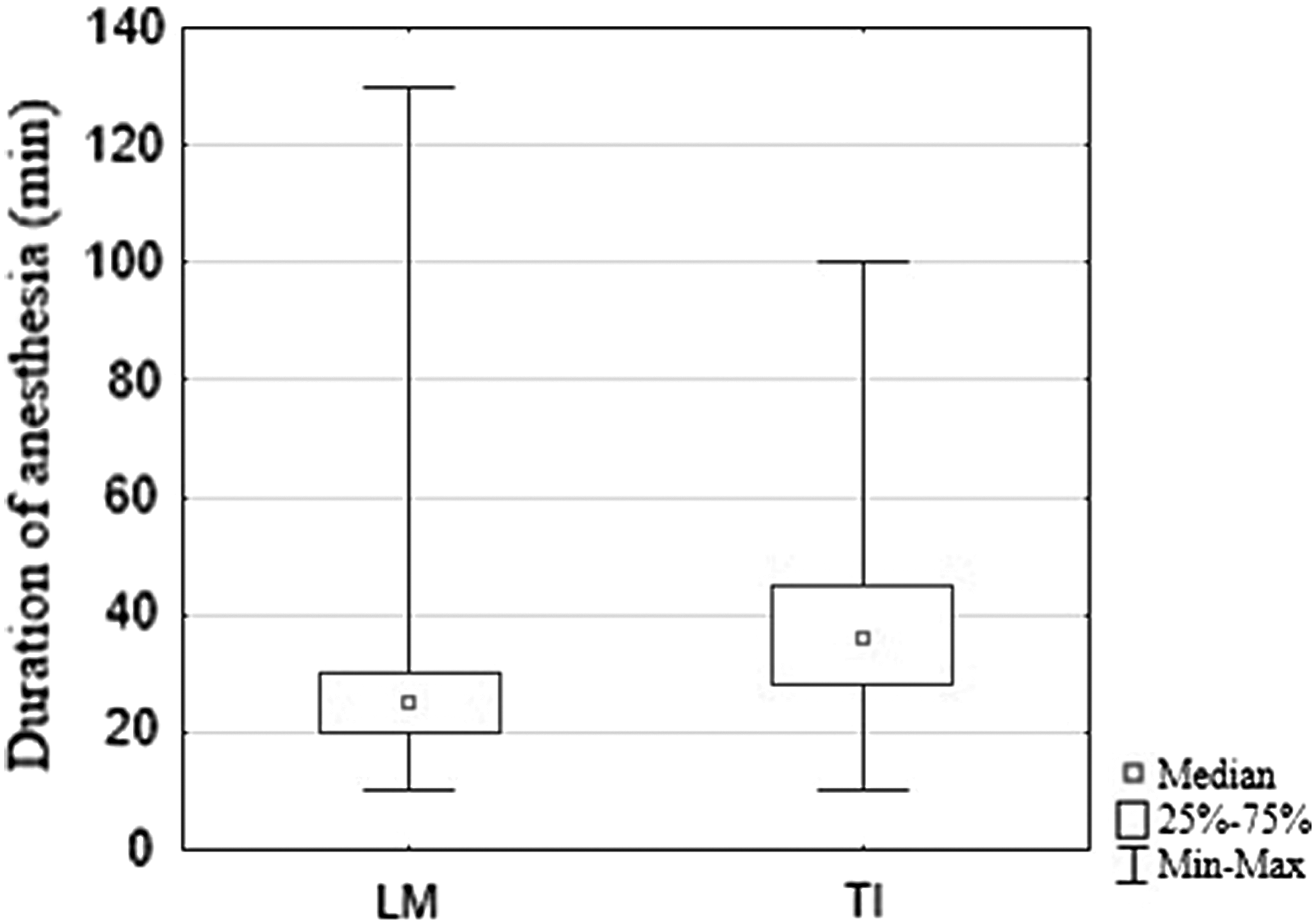
Comparison of duration of anesthesia between LM (n = 94) and TI (n = 41) groups. LM, laryngeal mask; TI, tracheal intubation.
Demographic and Clinical Data of the Patients
Mann–Whitney test.
Chi-square test.
ASA, American Society of Anesthesiologists; BMI, body mass index; IQR, interquartile range; LM, laryngeal mask; TI, tracheal intubation.
Overall, the type of airway management significantly affected the frequency of certain complications. The incidence of postoperative laryngospasm was significantly lower in group where LM was used, compared to intubated patients (n = 2 versus n = 5; P = .015). Furthermore, there was a significantly smaller frequency of desaturation (n = 1 versus n = 5; P = .003) and cough (n = 0 versus n = 4; P = .002) in patients using LM. There were no statistically significant differences in groups regarding complications such as sore throat (n = 1 versus n = 1; P = .543), bronchospasm (n = 0 versus n = 1; P = .128), and aspiration (n = 0 versus n = 1; P = .128) (Table 2, Fig. 2).
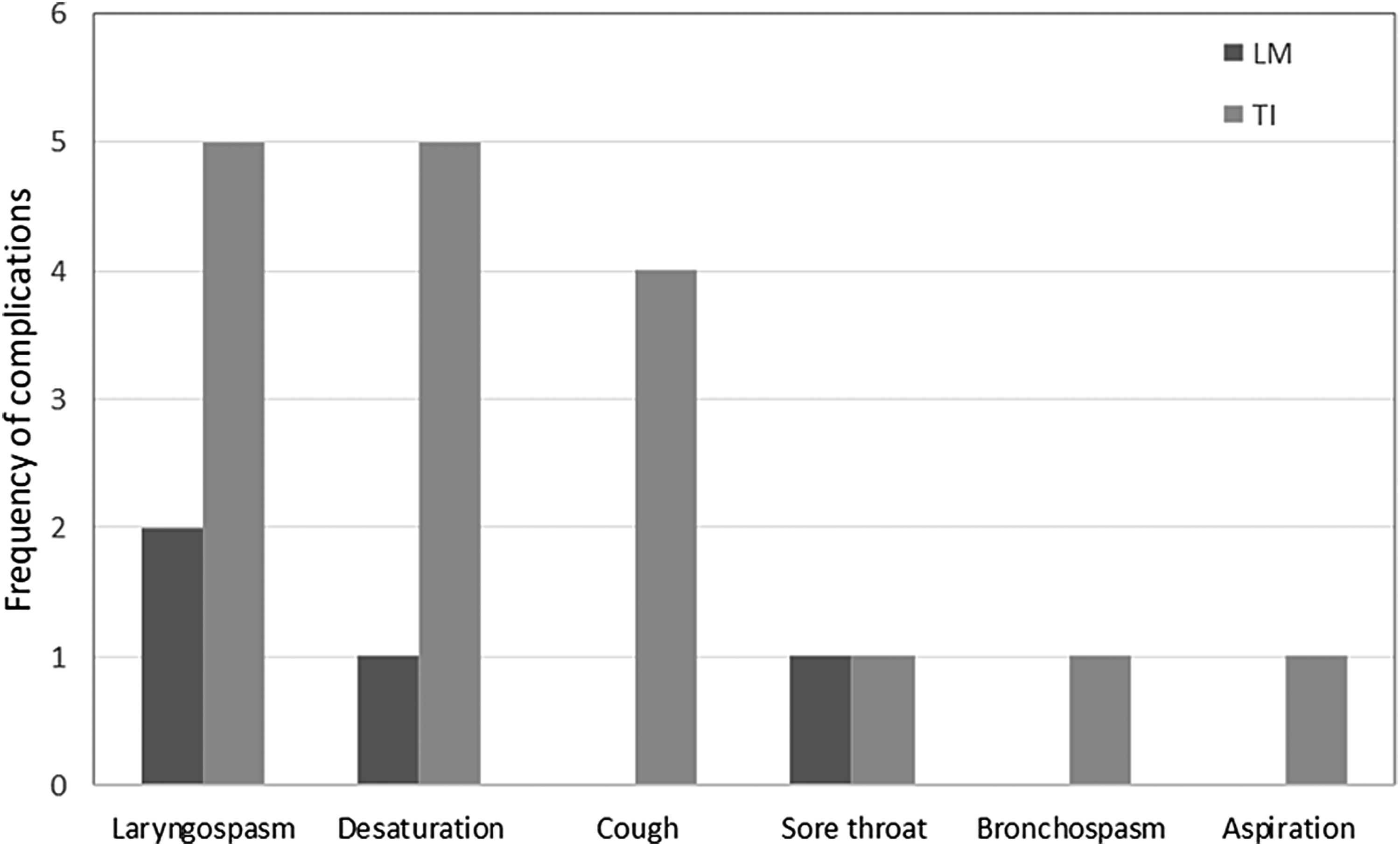
A comparison of the complications between LM (n = 94) and TI (n = 41) groups.
A Comparison of the Respiratory Complications Between Two Groups
Some patients had two or more complications.
Chi-square test.
LM, laryngeal mask; TI, tracheal intubation.
Discussion
In this comparative study, PIRS using LM airway in children was found to be safe and successful surgical procedure with shorter duration of anesthesia and lesser frequency of both intraoperative and postoperative respiratory complications. In children undergoing short surgeries with low insufflation pressures, safe anesthesia can be achieved using LM airway with no muscle relaxant. Our results are in agreement with few other studies and meta-analyses.5,7,9
This study used a nonrandomized comparison, which might be its biggest limitation. A larger number of patients might have also revealed a different frequency of complications in regards to different methods of anesthetic conduction. Nowadays two main airway management techniques are used. LM is easier to administer and generally used in shorter surgical procedures, while TI provides easier airway control and is more commonly used in everyday practice. TI is usually preferred over LM when carrying out inguinal hernia repair. A few studies have confirmed the safety of using LM in inguinal hernia repair, but nonetheless it has gained no significant traction in today's use.10–13 LM airway has been the treatment of choice for many years in short-duration pediatric surgical procedures where the patient is in the supine position.
New LM models have been developed and their use has been increasing. In comparison to TI, the advantages of using an LM airway include faster insertion without the use of laryngoscope and a higher rate of successful first attempts, even among novice providers. Successful TI requires more complicated training, and evidence suggests that today's practitioners are having a hard time at mastering this procedure. Resuscitation might be delayed and unfavorable outcomes might happen if endotracheal intubation cannot be conducted on time or if the tube is not properly set. Following modern trends, less invasive laparoscopic techniques for pediatric inguinal hernia repair with the duration of surgery from 15 to 20 minutes have been reported.1–4 The actual need for muscle relaxants and TI had to be reviewed due to lower insufflation pressures and shorter anesthesia times.
This led to LM airway being accepted as a valuable device for airway management during pediatric anesthesia, while TI is still considered to result in less complications compared to LM in conduction of general anesthesia. At a recent time, LM has gained vast popularity in pediatric anesthesia and is reported to be safe in all age groups for various surgeries.14,15 The most common complications of aforementioned airway conduction are laryngospasm, bronchospasm, cough, desaturation, aspiration, and a sore throat. With regards to the high rate of inguinal hernia it is of utmost importance to clarify which airway management technique results in fewer complications. Meta-analysis indicates that the rates of postoperative desaturation, laryngospasm, and cough are parallelly decreased when LM airway is used instead of TI. 5
Laryngospasm, very common in pediatric patients, usually occurs when vocal cords are irritated by respiratory secretions or blood. Comparing postoperative laryngospasm incidence during LM airway and TI revealed significantly lower incidence of laryngospasm when using LM airway. This finding is in agreement with a meta-analysis conducted by Luce et al. which also showed a number of other complications, like desaturation and sore throat, being less frequent when using LM, further confirming our results. 5
Aspiration, also a quite common complication, was proven not to differ in frequency when using LM or TI. Several studies have also shown no dissimilarity in frequency when using LM. Aspiration is usually caused by increased intraabdominal pressure, which leads to increased intragastric pressure.5,9 Our study did not follow the intragastric pressure values during surgeries but a study by Ozdamar et al., which recorded the pressures both when using LM airway and TI, advocates LM application as a feasible anesthetic device in pediatric laparoscopic surgery. 10 We have noted that the duration of anesthesia was significantly shorter when using LM. This was unanimous with a study conducted by İnce et al. 9 The part of the reason for this lies in the fact that it takes less time to position a LM than it takes to intubate a patient. The abovementioned study showed no significant difference between the duration of surgery confirming our results that also showed no difference in duration no matter LM or TT was used. It is worth mentioning that no muscular relaxant was used when LM was administered, which probably shortened duration of anesthesia. The use of muscle relaxation in laparoscopic surgery offers increased visibility of the surgical field and decreased the risk of complications because of patient movement while trocars or laparoscopic instruments are in place, although nowadays many laparoscopic procedures may be successfully performed without use of muscle relaxation. In contrast, the use of muscle relaxants may be related to increased anesthesia-related complications. 16
Recently studies have been reporting the safety of LM use in both adults and children.16,17 A study by Chen et al. asserts that no muscle relaxant is necessary in general anesthesia when using LM airway. 18 It is very important to emphasize that our study population is a very specific group of patients, with median age of 4 years using low insufflation pressure of 6–8 mmH2O in surgeries lasting 10–12 minutes. Although we have satisfactory sample size, anesthesia related complications are rare and would require a larger sample size to accurately determine.
Conclusion
The use of LM airway with no muscle relaxant is a safe alternative to TI in short lasting lower abdominal procedures, although this may not be generalizable for all pediatric age groups or procedures. LM airway use during pediatric anesthesia results in a significant reduced incidence of postoperative complications such as desaturation, laryngospasm, and cough. Duration of anesthesia is significantly shorter when using LM in comparison to TI.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.