
Abstract
Abstract
Aim:
There is still no consensus on whether laparoscopic surgery can be routinely recommended as a safe approach for complex Crohn's disease (CD).
Methods:
PubMed, Embase, and Cochrane library databases were searched (up to February 2019). Comparative studies reporting laparoscopic surgery for complex CD (LC group) comparing with simple CD (LS group) were included. The outcomes were blood loss, operative time, conversion rate, length of hospital stay, postoperative complications, and reoperation rate within 30 days after surgery.
Results:
Thirteen retrospective studies with 1120 participants were included. The LC group has significantly more blood loss (weighted mean difference [WMD] 43.64 mL; 95% confidence interval (CI) 8.37–78.91; P = .020), longer operative time (WMD 17.59 minutes; 95% CI 6.38–28.81; P = .002), higher conversion rate (WMD 2.04%; 95% CI 1.43–2.91; P < .001), and longer length of hospital stay (WMD 0.86 day; 95% CI 0.53–1.19; P < .001). Overall postoperative complication rates (WMD 0.98; 95% CI 0.71–1.34; P = .90) did not differ significantly between the 2 groups.
Conclusions:
LC is safe and feasible with comparable postoperative complications, although there is a more blood loss, longer operative time, higher conversion rate, and longer length of hospital stay.
Introduction
Crohn's disease (CD) is an autoimmune disease with skipping lesions throughout the intestine, which can affect the entire digestive tract from the mouth to anus. The incidence and morbidity of CD are increasing in recent decades. 1 It has been shown that the cumulative surgical rate increased year by year, varying from 16.3%, 33.3%, and 46.6%, when the CD patients were diagnosed after 1, 5, and 10 years, respectively. 2
Comparing with the traditional laparotomy, laparoscopic surgery has the advantages of being minimally invasive, less pain, better abdominal integrity, early postoperative recovery, and shorter length of hospital stay.3–6 Previous studies reported that the laparoscopic approach was safe and effective in small bowel and ileocolic CD.7–11 However, there is still no consensus on whether laparoscopic surgery can be routinely recommended as a safe procedure in complex CD, because of extensive intestinal inflammation of the disease. 12
Therefore, we conducted a meta-analysis to evaluate the safety and efficiency of laparoscopic resection for laparoscopic surgery for complex CD (LC) compared with laparoscopic surgery for simple CD (LS).
Methods
This meta-analysis adheres to the preferred reporting items for systematic reviews and meta-analysis guidelines.13,14 This study was approved by the Institutional Review Board (IRB) of The Sixth Affiliated Hospital of Sun Yat-sen University.
Search and selection strategies
PubMed, Embase, and Cochrane library databases were searched up to February 2019 without restriction to languages. The search terms were as follows: “Crohn's disease,” “Inflammatory bowel disease,” “laparoscopy surgery,” “laparoscopy,” “complex,” “complicated,” “recurrent,” “fistula,” “penetrating,” “abscess,” “perforating,” and “abscess.”
Inclusion criteria and exclusion criteria
Randomized controlled trials (RCTs) and retrospective studies comparing laparoscopic resection for complex CD with simple CD were enrolled. Also, all the included studies should have at least one of the relevant outcomes mentioned below. The exclusion criteria were as follows: (a) lack of sufficient data or outcomes of interest; (b) duplicate publication; (c) noncomparative studies, editorials, letters, conference abstracts, review articles, case reports, and animal experimental studies.
Two independent authors extracted and summarized the data from the included studies independently.
In this study, complex CD was defined as CD with fistula formation, intra-abdominal abscess formation, or recurrent CD, and simple CD was defined as primary nonpenetrating CD.15–17
Outcomes of measures
The primary outcomes were conversion rate and postoperative complication rate. Postoperative complication would be divided into wound infection, pneumopathy, anastomotic leakage, intra-abdominal infection, obstruction, and reoperation rate if data were enough. The secondary outcomes were blood loss, operative time, and length of hospital stay.
Statistical analyses
Statistical analyses were performed by RevMan® 5.3 software (Cochrane Collaboration®, Oxford, United Kingdom). For continuous variables (blood loss, operative time, and postoperative length of hospital stay), weighted mean differences (WMDs) were calculated. For dichotomous variables (conversion and complications), odds ratios were calculated.
Level of statistical significance was set at P < .05. Funnel plots were used to evaluate publication bias. If there was no significant heterogeneity among the articles, the fixed-effects model was used; otherwise, a random-effects model was used. For continuous data as median and range values, the means and standard deviations were calculated by the formula described by Hozo et al. 18
Results
A total of 13 retrospective studies with 1120 participants (489 participants in LC group, and 631 participants in LS group) were included (Fig. 1).15–17,19–21 The characteristics of studies included in this meta-analysis are shown in Table 1. The Newcastle–Ottawa scale was used to evaluate the methodological quality of all the retrospective studies.
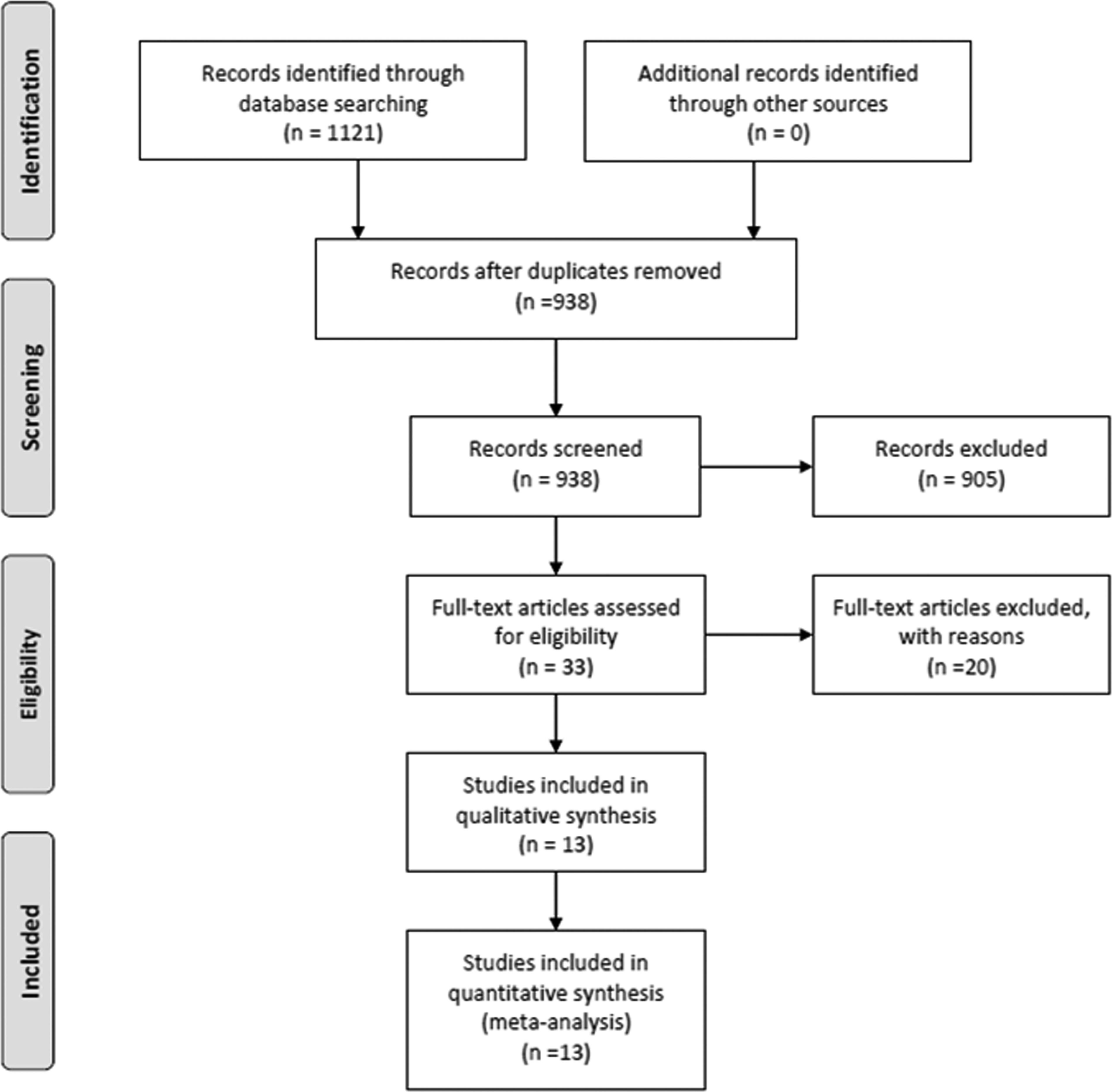
Flow diagram of studies identified, included, and excluded.
Characteristics of Studies Included in This Meta-Analysis
Median.
Mean.
BMI, body mass index; CD, Crohn's disease; F, female; LC, laparoscopic surgery for complex CD; LS, laparoscopic surgery for simple CD; M, male; ND, no data; R, retrospective.
Primary outcomes
Conversion rate
All the 13 studies15–17,19–28 reported conversion events. The conversion rate was 18.6% in the LC group and was significant higher (18.6% compared with 10.5%, P < .001) than the LS group (Fig. 2).
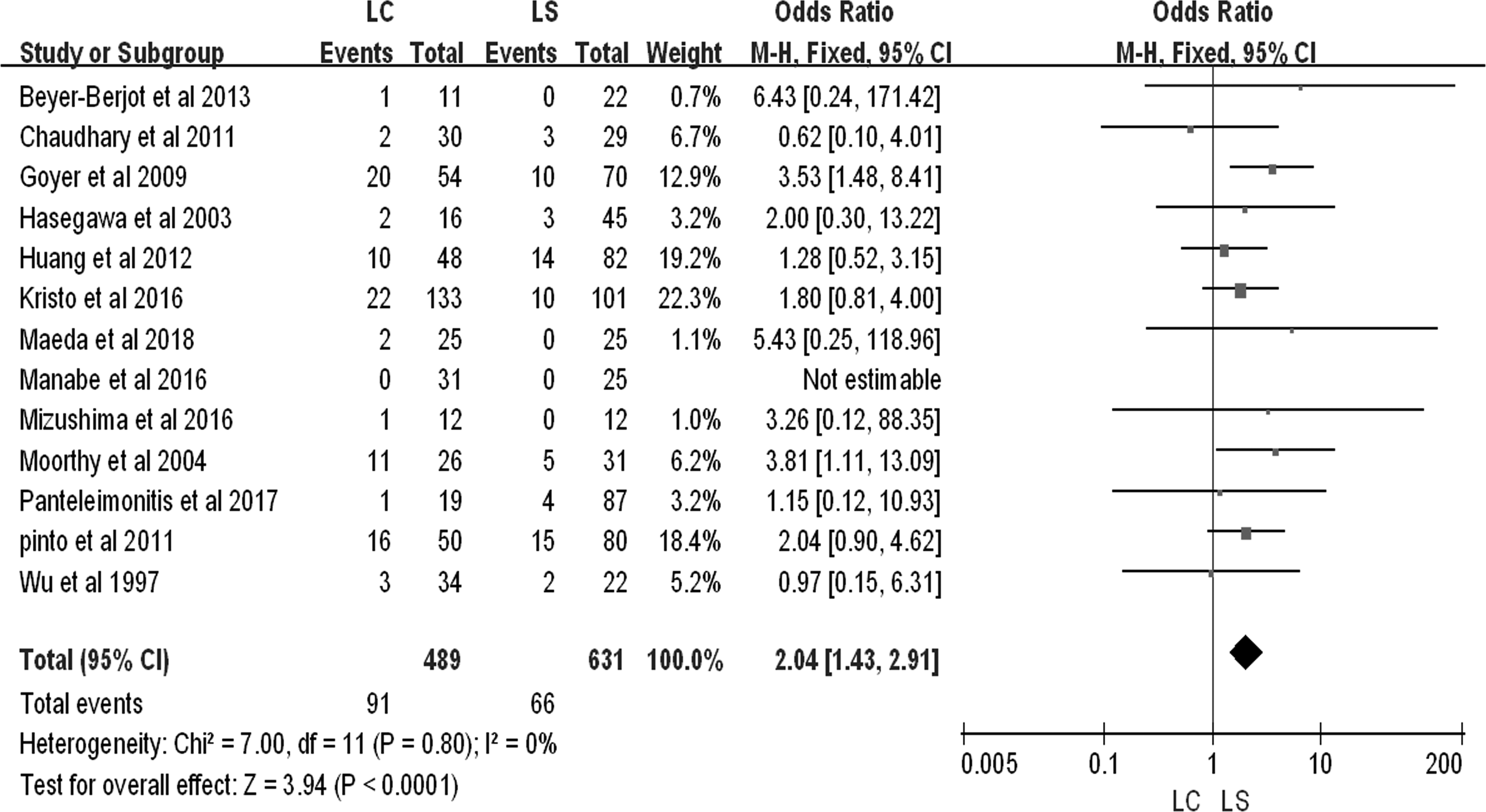
Forest plot describing conversion rate between LC group and LS group. CI, confidence interval; LC, laparoscopic surgery for complex Crohn's disease; LS, laparoscopic surgery for simple Crohn's disease.
Postoperative complications
There was no significant difference between the 2 groups in overall postoperative complication rates (WMD 0.98; 95% confidence interval [CI] 0.71–1.34; P = .90) (Fig. 3). No publication bias between the 2 groups was observed (Fig. 4). Similarly, when postoperative complications were further divided into wound infection, pneumopathy, anastomotic leakage, intra-abdominal infection, obstruction, and reoperation rate, there were still no significances between the 2 groups (Table 2).

Forest plot describing overall postoperative complication rates between LC group and LS group. CI, confidence interval; LC, laparoscopic surgery for complex Crohn's disease; LS, laparoscopic surgery for simple Crohn's disease.
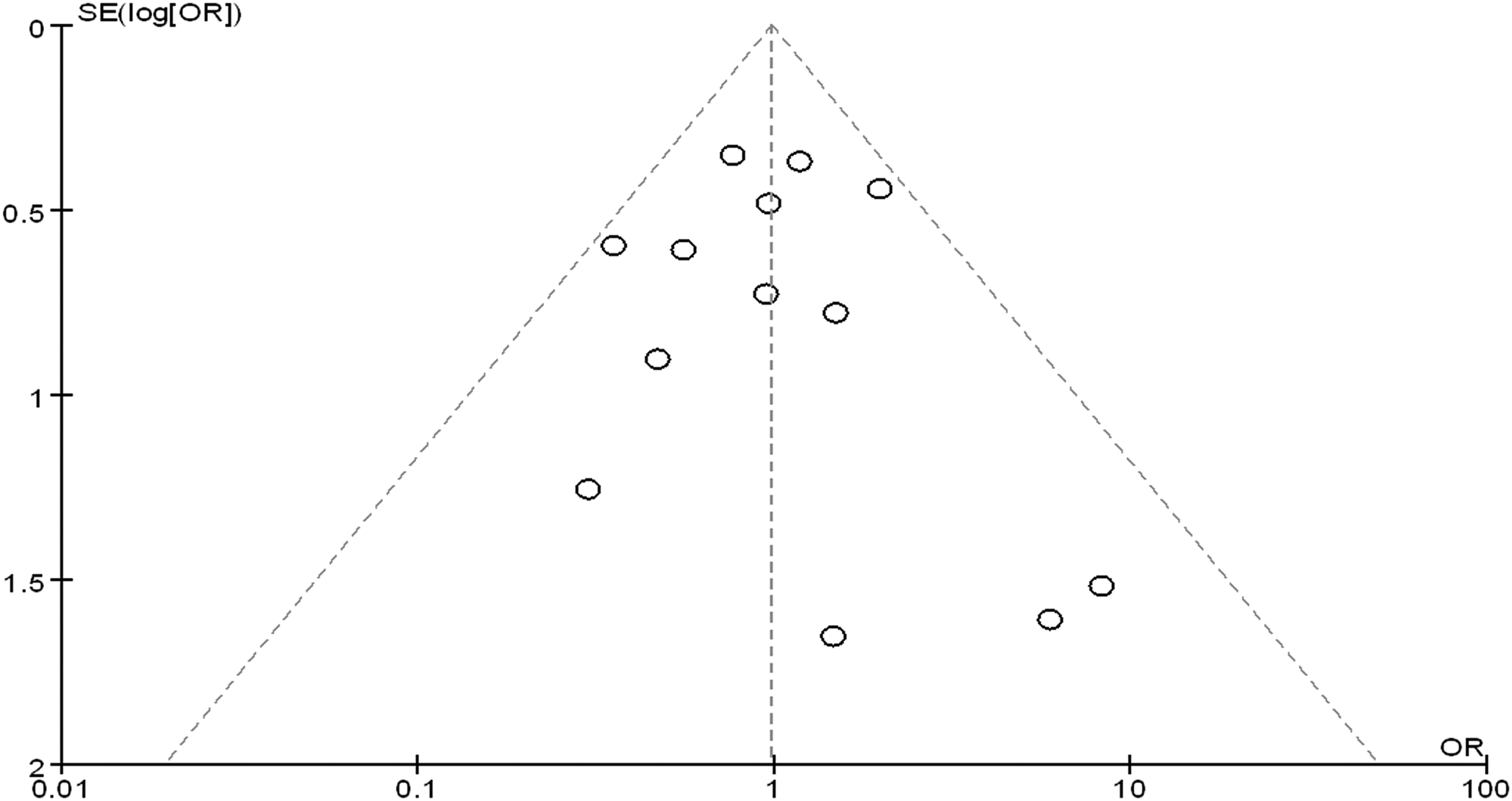
Funnel plot showing no significant publication bias of overall postoperative complication rates.
Results of Meta-Analysis Comparison of Laparoscopic Surgery for Complex Crohn's Disease and Laparoscopic Surgery for Simple Crohn's Disease
CD, Crohn's disease; CI, confidence interval; LC, laparoscopic surgery for complex CD; LS, laparoscopic surgery for simple CD; OR, odds ratio; WMD, weighted mean difference.
Secondary outcomes
Blood loss
Eight studies15,21,23–28 encompassing 714 patients reported blood loss, and there was significant heterogeneity among the studies (I2 = 66%, P = .005). So, in random-effects models, pooled data indicated a significant difference favoring the LS group (WMD 43.64 mL; 95% CI 8.37–78.91; P = .020) (Fig. 5).
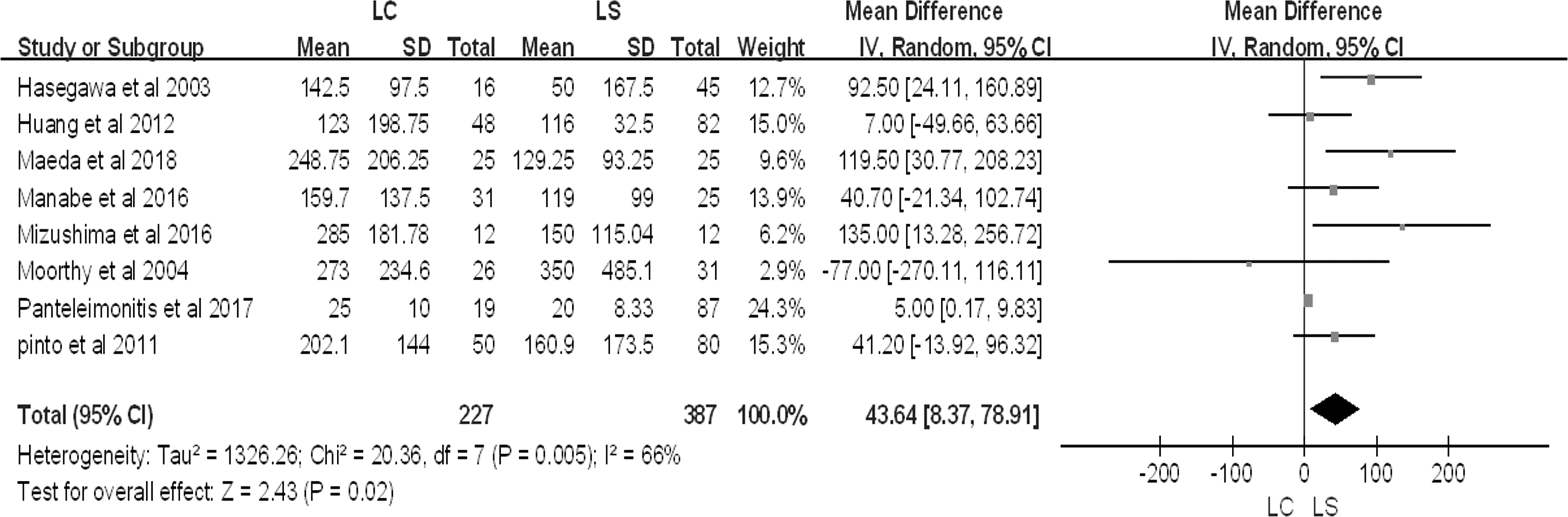
Forest plot describing blood loss between LC group and LS group. LC, laparoscopic surgery for complex Crohn's disease; LS, laparoscopic surgery for simple Crohn's disease.
Operative time
Eleven studies15–17,20–28 reported operative time for 830 patients, and there was significant heterogeneity among the studies (I2 = 62%, P = .003). So, in random-effects models, pooled data indicated that the operative time was significant longer in LC group than the LS group, with a WMD of 17.59 minutes (95% CI 6.38–28.81; P = .002) (Fig. 6).
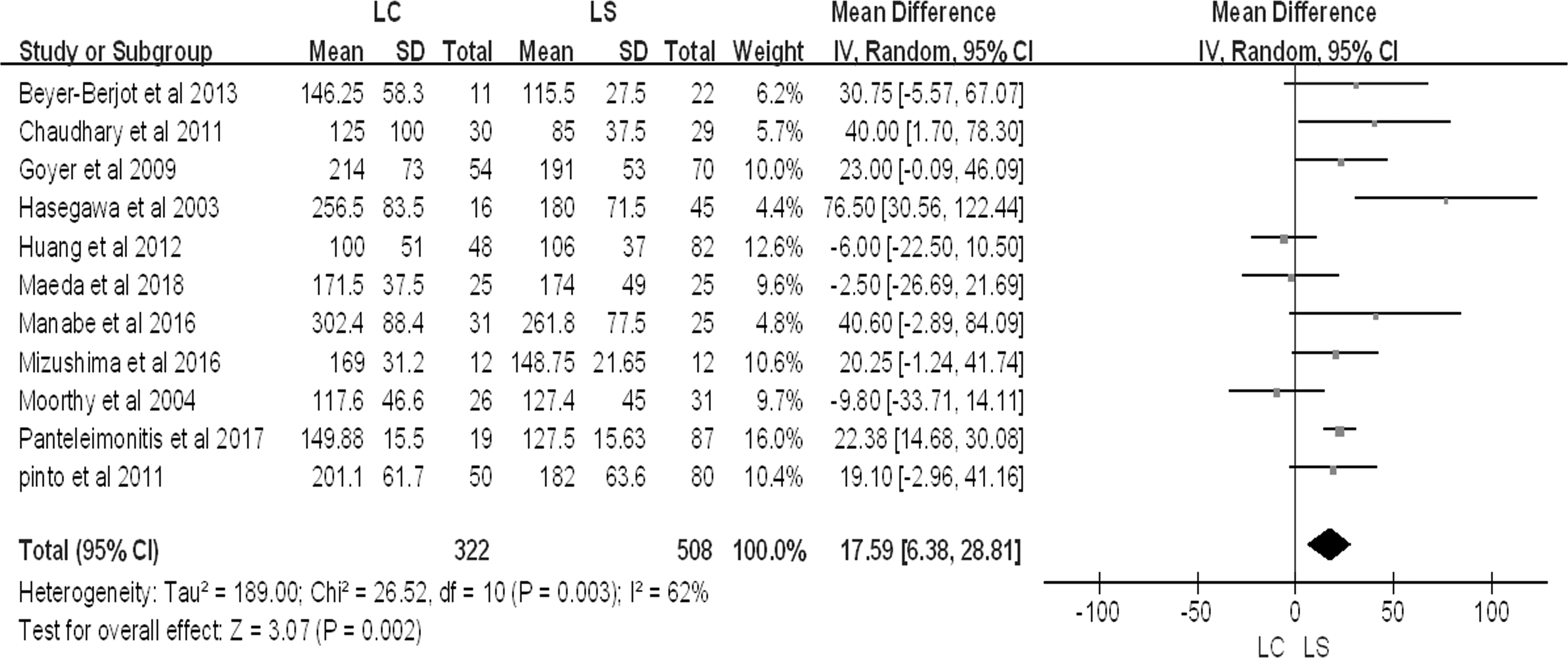
Forest plot describing operative time between LC group and LS group. LC, laparoscopic surgery for complex Crohn's disease; LS, laparoscopic surgery for simple Crohn's disease.
Postoperative length of hospital stay
Nine studies15–17,20–23,27,28 reported postoperative length of hospital stay for 853 patients. The length of hospital stay was significant longer in LC group than the LS group, with a WMD of 0.86 day (95% CI 0.53–1.19; P < .001) (Fig. 7).

Forest plot describing postoperative length of hospital stay between LC group and LS group. LC, laparoscopic surgery for complex Crohn's disease; LS, laparoscopic surgery for simple Crohn's disease.
Discussion
This meta-analysis of 13 studies, encompassing 1120 patients comparing the efficacy of LC with LS, was the first meta-analysis comparing LC with LS. The results confirm that the postoperative complication was similar between the 2 groups. We hope that our meta-analysis could illustrate the safety and feasibility of laparoscopic surgery, as well as promote its application in complex CD.
Many studies had demonstrated that comparing with laparotomy, laparoscopic resection for small bowel and ileocolic CD was safe, efficient, was associated with shorter length of hospital stay and time to bowel movement, and fewer operative complications.7–11 Laparoscopic surgery was a contraindicant for complex CD in the traditional view. Comparing with open surgery, Ren et al. found that laparoscopic surgery was safe with less systemic stress responses, fewer postoperative complications, shorter length of hospital stay, and lower postoperative mortality for fistulizing CD. 29 To date, there was only 1 meta-analysis performed by Shigeta et al. encompassing 627 patients, comparing recurrent CD with primary CD in 2013. 30 They found similarities in postoperative complications and concluded that laparoscopic resection for recurrent CD was safe and feasible. However, the safety of laparoscopic surgery for complex CD is still unknown.
Although laparoscopic surgery for complex CD has more technical limitations than open surgery, this procedure is thought to have several potential benefits, especially the reduced number of intra-abdominal adhesions from laparoscopic surgery may be a benefit for the repeated operations of CD patients. Being different from the meta-analysis above, this meta-analysis not only involved recurrent disease but also included perforating disease. To investigate the safety and efficiency of laparoscopic resection for LC, the variates of blood loss, operative time, length of hospital stay, and reoperation rate were compared. To our knowledge, this is the first meta-analysis that focuses on evaluating the safety of laparoscopic surgery for complex CD with a large volume of CD patients. Our results found that the postoperative complications were similar between 2 groups. We hope that our meta-analysis could illustrate the safety and feasibility of laparoscopic surgery, as well as promote its application in complex CD.
This meta-analysis has several limitations that must be taken into account. First, all the included studies were observational with no RCTs. Without adequate random sequence generation and blinding, the risk of bias might increase. Second, the heterogeneity of blood loss, operative time, length of hospital stay, and reoperation rate has been shown to be significant. This heterogeneity might be due to the calculation from median and range values to means and standard deviations. Finally, the outcomes might be confounded by the quality of the articles of publication, section, and reporting bias.
Conclusions
The results of the current meta-analysis suggest that LC is safe and feasible with equivalent postoperative complications, although there is more blood loss, longer operative time, higher conversion rate, and longer length of hospital stay. Future large-sample RCTs and long-term outcomes are awaited to assess the association with LC.
Footnotes
Authors' Contributions
Z.L.Y., D.Z.L., P.L., and X.J.W. contributed to study concept and design, acquisition, analysis, and interpretation of data, and drafting of the article. J.C.H., Y.F.C., Z.R.C., Y.F.Z., J.K., and X.F.G. contributed to data collection and article review. D.Z.L., Z.L.Y., and X.J.W. contributed to study concept and design, analysis and interpretation of data, and critical revision of the article for important intellectual content. X.J.W. and P.L. supervised the study. All authors read and approved the final article.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) of The Sixth Affiliated Hospital of Sun Yat-sen University.
Informed Consent Statement
This is a meta-analysis study and we petition for waiver of informed consent.
Data Sharing Statement
No additional data are available.
Disclosure Statement
No competing financial interests exist.