
Abstract
Objective:
The aim of this study was to compare the effectiveness of epidural block (EDB) and paravertebral block (PVB) for minimally invasive pectus repair with the conventional method in terms of pain control during and after pectus operations, patient comfort, and length of stay in hospital.
Materials and Methods:
A retrospective review was made of patients who underwent minimally invasive pectus repair. The patients were allocated into three groups as follows: PVB group (Pre-emptive ultrasound-guided bilateral thoracic single injection PVB, n = 15); EDB group (Pre-emptive landmark-guided single injection thoracic EDB, n = 8); and Control group (Neither PVB nor EPB, n = 9). The intraoperative analgesic requirement was recorded, and a visual analog scale (VAS) for pain evaluation and the Postoperative Patient Satisfaction Scale were applied to all patients.
Results:
The intraoperative analgesic requirement, VAS scores, postoperative satisfaction level, and time to first requirement for postoperative analgesia were different between the control and PVB groups (P < .001) and between the control and EDB groups (P < .001), but not different between the PVB and EDB groups. Although the length of stay in hospital was shorter in the PVB and EDB groups compared to the control group, the difference was not statistically significant (P = .422).
Conclusion:
Epidural and bilateral paravertebral blockades performed in conjunction with general anesthesia decrease the intraoperative and postoperative need for analgesics, and might be beneficial for pain management and contribute to a shorter length of hospital stay for patients undergoing minimally invasive pectus repair operations. Both blockades also significantly improved the patient satisfaction.
Introduction
Pectus excavatum (PE) and pectus carinatum (PC) are the most common congenital chest wall deformities. 1 The Nuss technique for PE and reverse Nuss technique for PC, which can eliminate the need for an extensive anterior chest wall incision and resection of multiple ribs or cartilage and sternal osteotomies, are the most commonly performed minimally invasive surgical techniques. However, forceful bending of the sternum and sternal cartilage may lead to significant postoperative pain and discomfort in patients. 2 Preventing surgical and medical complications and appropriate management of pain during and after the surgery is essential to improve recovery, increase patient satisfaction, decrease patient and family anxiety, help patients regain function, and prevent a prolonged hospital stay. 3 Therefore, this has led anesthetists to use adjunctive analgesic methods such as thoracic paravertebral, epidural, or intercostal anesthetic injections for pain management during and after these operations. 4
Thoracic epidural block (EDB) applied before anesthetic induction is still the most frequently used perioperative interventional analgesic method in most clinics.5,6 Although EDB is generally considered a safe method, recent reports have shown severe and permanent neurological injury after minimally invasive repair of PE using EDB.5,7 The outcome of paravertebral block (PVB) is satisfactory in respect of patient comfort and effective pain control. A previous report of a small series revealed that bilateral PVB and EDB resulted in equivalent pain scores in pediatric patients undergoing a “minimally invasive pectus repair of excavatum (MIRPE)” procedure. 8 However, no consensus has yet been established for a single best anesthetic and analgesic approach to patients undergoing pectus deformity repair.
The aim of this study was to compare the effectiveness of two peripheral and central blockade methods with the conventional method in terms of pain control during and after a Minimally Invasive Pectus Repair procedure, patient comfort, and length of stay in hospital.
Materials and Methods
Study design and participants
Approval for the study was granted by the Local Ethics Committee of the university hospital (Date: 19.12.2018, number: 2018.12.11).
A retrospective review was made of patients who underwent minimally invasive pectus repair in the Thoracic Surgery Department between January 2014 and May 2018. The demographic and clinical data of patients including age at the time of operation, gender, height, weight, intraoperative opioid requirement, and length of stay in hospital were obtained from the hospital network database, anesthesia follow-up charts, and patient records in the Thoracic Surgery Department. The amount and time of intraoperative analgesia requirement was recorded, and a visual analog scale (VAS) pain scale and a Postoperative Patient Satisfaction Scale were applied to all patients. Any patients with incomplete data were excluded from the study.
The patients were divided into three groups as follows:
PVB group: a pre-emptive ultrasound-guided bilateral thoracic single injection PVB was administered after sedation (n = 15).
EDB group: a pre-emptive landmark-guided single injection thoracic epidural blockade was administered after sedation (n = 8).
Control group: neither PVB nor EPB was administered before general anesthesia (n = 9).
Thoracic paravertebral blockade
In the operation room, patients were sedated with 0.03–0.05 mg/kg midazolam administered intravenously. Then, a 10–18 MHz linear ultrasound probe (EsaoteMyLab 30, Geneva, Italy) was placed in the paramedian plane over/between two transverse processes with the patient in a sitting position. The transverse processes, superior costo-transverse ligament (STCL) and pleura were visualized at the level of T6 and T7 vertebral segments. After the skin and subcutaneous tissue were anesthesized with 3 cc 2% lidocaine HCl (Aritmal, Biosel), an 18 gauge 50 mm needle (Pajunk, Geisingen, Germany) was inserted using the in-plane technique and was advanced until it passed the STCL. After negative aspiration, 8 mL of 0.5% bupivacaine HCl (Marcaine 0.5%, Astra Zeneca) was injected. The spread of the injectate and the collapse of the pleura were confirmed on ultrasound. The procedure was performed bilaterally. Then all patients were positioned supine and intubated with a single lumen endotracheal tube and the general anesthesia protocol was applied.
Thoracic epidural blockade
In the operation room, patients were sedated with 0.03–0.05 mg/kg midazolam administered intravenously. Then, EDB was performed using an epidural kit (Epidural Minipack, Portex, Smiths Medical, ASD, Inc., Keene) comprising an 18 gauge needle and catheter, under sterile conditions. The skin and subcutaneous tissue were anesthetized with 3 cc 2% lidocaine HCl. The epidural space was determined with the loss of resistance method using saline at T6–7 segment. The catheter was advanced in the cephalad direction and was inserted 2 cm beyond the needle tip. Eight milliliters of 0.5% bupivacaine HCl was injected before the anesthesia induction and 8 mL with the surgery incision. Then, the patient was positioned supine and intubated with a single lumen endotracheal tube and the general anesthesia protocol was applied.
Surgical procedure
In PE patients a Nuss procedure was performed through two oblique incisions 8 cm in length on the anterior axillary lines, bilaterally. A 30°, 10 mm thoracoscope was inserted into the thoracic cavity through the lower part of the right incision using a trochar to guide the introducer, which was entered from the upper part of the incision and passed through the substernal space. With the guidance of the introducer, a pectus bar curved according to the deformity was slipped substernally from the left incision to the right incision. The bar was flipped over and emerged from the sternum, then a stabilizer was placed to fix it on the right side. The incisions were closed after suction of the right-side thoracic cavity with a small bore catheter.
In PC patients, unlike the Nuss procedure, the curved bar was placed subcutaneously without entering the thoracic cavity and fixed to the stabilizers that were secured to two consecutive ribs with pericostal steel sutures on both sides.
During the operation, if the anesthesia superficialized as standard (pupil diameter, ventilation, and surgery-related motion) and this condition was reflected in the hemodynamic parameters (blood pressure and heart rate increase), 1 μg/kg remifentanil (Ultiva, Glaxo Smith Kline, India) was administered within 30–60 seconds as IV bolus, and then, 0.5 μg/kg/h remifentanil infusion was administered continuously. At the end of the postoperative first hour, pain was evaluated using a VAS. In the postoperative period, the first analgesic requirement of the patients was noted.
Visual analog scale
This scale is used to evaluate the severity of pain in patients, with the lowest point of 0 indicating no pain and the highest points of 10, intolerable pain. 9
Patient satisfaction scale
Postoperatively, a patient satisfaction scale was applied to evaluate the satisfaction of patients in respect of pain management. The scale was evaluated as 5 points (5: very satisfied, 4: satisfied, 3: not sure, 2: not satisfied, 1: not satisfied at all) and the level of patient satisfaction was considered high when the score was high. 10
Statistical analysis
The chi-square test and Fischer's exact test were used for categorical variables. The Kruskal Wallis test or one-way analysis of variance (ANOVA) test were used for numerical variables. To determine from which group, a difference originated, post hoc analyses were applied using the Mann–Whitney U test or Tukey Multiple Comparisons test. Spearman's rho Correlation test was used to determine correlations between the parameters of the patients.
A value of P < .05 was accepted as statistically significant.
Results
Evaluation was made of a total of 32 patients (PC = 13, PE = 19) eligible for the study. None of the patients required admission to the intensive care unit. After the surgical intervention, no surgical complications (such as hypotension, vascular injury, neurological deficit, and nausea/vomitting) were observed in any patient. The patients were all satisfied regarding the analgesic treatment/intervention for pain in the PVB and EDB groups (P < .001), while none were satisfied in the control group. The VAS scores and intraoperative analgesic requirement were signficantly different between the control and PVB groups (P < .001) and between the control and EDB groups (P < .001) but no significant difference was found between the PVB and EDB groups. The first analgesic requirement of the patients was signficantly different between the control and PVB groups (P < .001) and between the control and EDB groups (P < .001) but no significant difference was found between the PVB and EDB groups. The length of stay in hospital was shorter in the PVB and EDB groups compared to the control group, but the difference was not statistically significant (P = .422) (Table 1, Figs. 1–3).

Error bar comparing VAS at 1 hour postoperatively according to the pain management method for
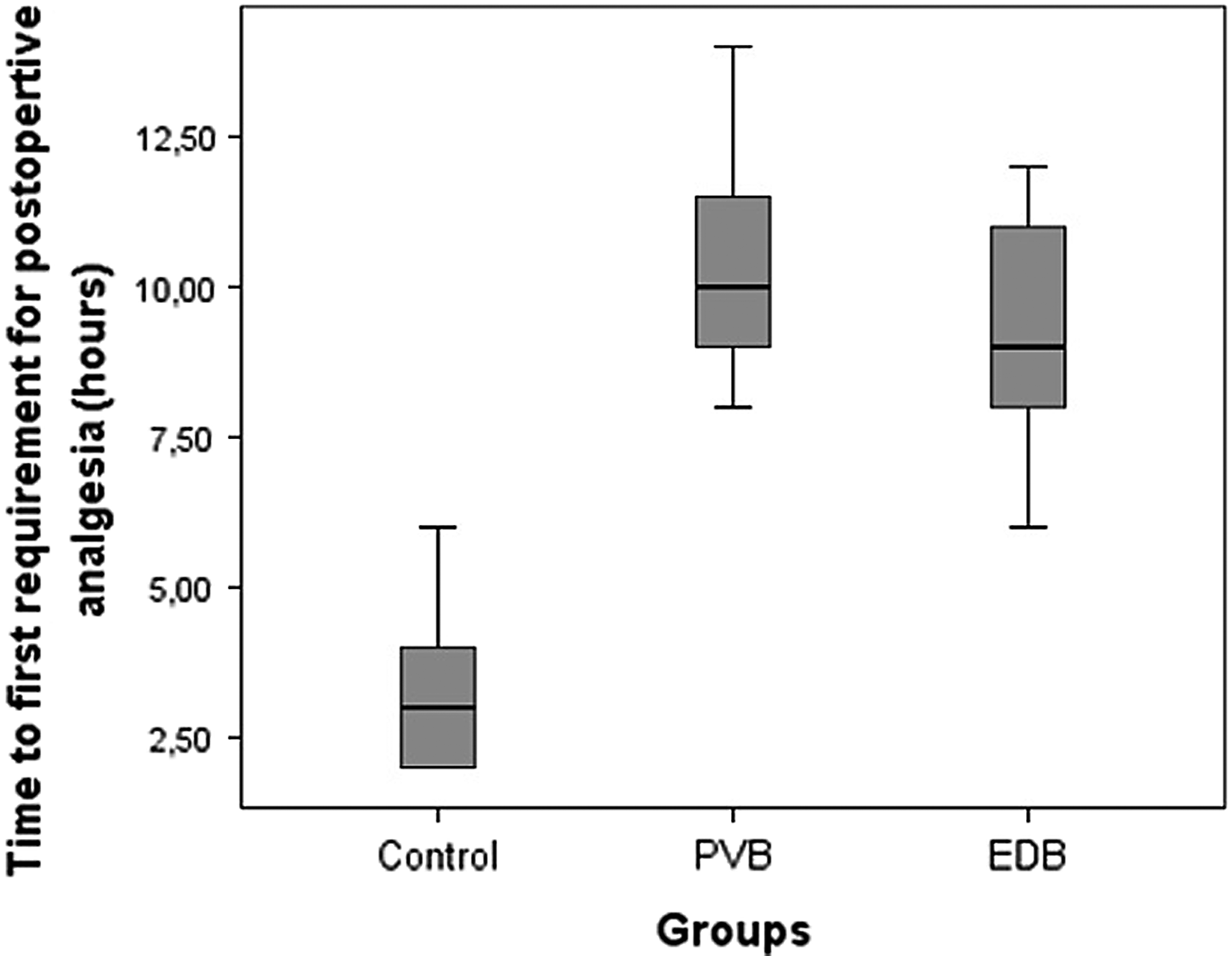
Box plot comparing time to first requirement for postoperative analgesia according to the pain management method for

Box plot comparing length of hospital stay according to the pain management method for
The Demographic Data of the Patients and the Significance of Differences Between the Three Groups
Data are shown as mean ± SD or median (25%–75%) values or number of patients.
EDB, epidural block; F, female; IO, intraoperative; M, male; n, number of patients; PC, pectus carinatum; PE, pectus excavatum; PVB, paravertebral block; SD, standard deviation; VAS, visual analog scale for pain in postoperative period.
Correlation analysis results demonstrated a significant positive correlation between the satisfaction scores and the anesthetic blockade method (r = 0.840, P < .001), between the satisfaction scores and time to first requirement for postopertive analgesia (r = 0.782, P < .001), between intraoperative analgesic requirement and VAS scores (r = 0.673, P < .001), and between the time to first requirement for postoperative analgesia and anesthetic blockade method (r = 0.580, P < .001). A negative correlation was found between the VAS scores and satisfaction scores (r = −0.800, P < .001), between the VAS scores and anesthetic blockade method (r = −0.672, P < .001), between the VAS scores and time to first requirement for postoperative analgesia (r = −0.770, P < .001), between intraoperative analgesic requirement and time to first requirement for postoperative analgesia (r = −0.584, P < .001), between intraoperative analgesic requirement and anesthetic blockade method (r = −0.669, P < .001), and between intraoperative analgesic requirement and satisfaction scores (r = −0.756, P < .001) (Table 2).
The Correlations Between the Dependent Variables of the Patients
IO, intraoperative; VAS, visual analog scale for pain in postoperative period.
Discussion
The minimally invasive pectus repair procedure is a common pediatric procedure with significant postoperative pain. EDB is the procedure performed most often, which provides good to excellent analgesic results for thoracic and abdominal surgeries in children.5,11,12 In a previous systematic review and meta-analysis by Stroud et al., the authors compared epidural analgesia with intravenous patient controlled analgesia (PCA) in patients undergoing MIRPE. 13 It was emphasized that pain scores immediately after, and at 24 and 48 hours after the surgery were significantly lower in patients treated with EDB than in patients treated with PVB, whereas the secondary outcomes (e.g., cost, length of stay in hospital, operation time, and rescue analgesics) were not different. However, it has been suggested that the addition of EDB to thoracotomy may be an independent risk factor for nerve injury. 14 It has been assumed that surgically induced changes to the configuration of the spinal canal in combination with factors affecting spinal cord perfusion secondary to thoracic EDB may lead to spinal cord hypoperfusion in patients undergoing the Nuss procedure. 7 As a result of these concerns, alternative methods for pain control in patients undergoing the Nuss procedure have been sought. With the increasing use of ultrasound-guided regional anesthesia, paravertebral nerve blockade serves as a non-neuraxial peripheral nerve block, which has been used effectively for more than two decades in children and adults for pain control after thoracic and abdominal surgeries. 15 In addition to providing a dense sensory block, the thoracic sympathetic chain may be blocked after PVB, 16 which may prevent hemodynamic fluctuations during the operation. Ultrasound-guided needle placement decreases the risk of pneumothorax and other complications such as vascular puncture, epidural spread, hypotension, and technique failure. 17 There are no reports in literature of permanent neurological injury after PVB. A meta-analysis of randomized trials comparing PVB and EDB revealed similar analgesic efficacy with a better side effect profile of PVB in adult thoracotomy patients. 18 Bilateral PVB in comparison with thoracic EDB in pediatric patients undergoing the Nuss procedure has been found to have equivalent results in postoperative pain management. 8 In a study by Qi et al., the effectiveness of bilateral PVB was compared with a control group, and it was concluded that ultrasound-guided bilateral PVB provides improved postoperative analgesia for children undergoing the Nuss procedure compared with intravenous PCA. 19
To the best of our knowledge, no previous study has evaluated the effectiveness of PVB and EDB in comparison with the conventional method for the management of pain during and after minimally invasive pectus repair. The results of this study showed that all patients in the control group had an increased need for analgesic medication during the operation and the postoperative VAS scores of these patients were higher than those of the patients in the PVB and EDB groups. In addition, it was seen that the need for analgesic drugs in these patients developed very early after surgery. From these findings, it was concluded that PVB and/or EDB methods decreased the need for analgesic medication both during and after surgery. At the end of this study, it was observed that application of single bilateral PVB and EDB could both decrease the intraoperative opioid need and increase the postoperative pain-free time. The patient-rated VAS pain scores were lower and overall patient satisfaction was higher in both the PVB and EDB groups. The length of hospital stay was shorter in the PVB and EDB groups than in the control group but not at a statistically significant level. However, no statistically significant difference was determined between the two interventional (PVB and EDB) groups in respect of any of these parameters. Furthermore, no significant complications or side effects were observed in either the EDB group or the PVB group. From the correlation analysis findings it was predicted that there could be an increase in the satisfaction score after the block application, a decrease in VAS score, and a decreased need for intraoperative analgesia and postoperative analgesia. It was observed that in patients with high patient satisfaction, the time to postoperative analgesia was prolonged and the need for intraoperative analgesia was lower, and in patients with low VAS scores, the time to postoperative analgesia was prolonged. However, for patients with intraoperative analgesic requirement, VAS scores were higher and the time to postoperative analgesia was shorter. Thus, from the correlation analysis findings it could be predicted that with the application of PVB or EDB to patients before surgery, the need for analgesic medication would be significantly reduced during the operation and VAS scores would be lower in the postoperative period, with a later postoperative need for analgesia and increased satisfaction levels of the patients in the postoperative period. Finally, it could be said that the findings of this study were consistent with those of previous studies demonstrating similar results in postoperative pain scores and intraoperative opioid requirements for both the EDB and PVB groups.
Appropriate postoperative pain management has been reported to affect the capacity for deep breathing, early mobilization, independent ambulation, and the length of hospital stay. 6 In a study by Loftus et al., a retrospective review was made of 137 patients who underwent PE repair using the Nuss and Ravitch methods with pain management via EDB, intercostal block, or PVB. The length of stay in hospital was significantly shorter in the PVB group and intercostal group compared with the EDB group. 20 In the present study, the length of stay in hospital was shorter in both the PVB and EDB groups compared with the control group but the difference was not statistically significant.
Limitations
This study had several limitations due to the retrospective nature. First, the numbers of patients enrolled in the study groups were not equal and were relatively low. No sample size calculation and posthoc power analysis were performed. The postoperative pain assessed with VAS was performed only once, and thus the levels of pain during subsequent postoperative hours could not be compared. Although there was no superiority between the two interventional groups, the PVB was performed under ultrasound guidance, while EDB was not. The length of hospital stay of the patients was recorded, but there were no data available concerning pain after discharge, recovery from surgery, or participation in physical therapy.
Conclusion
In conclusion, epidural and bilateral paravertebral blockades performed in conjunction with general anesthesia, decrease the intraoperative and postoperative analgesia requirement and might be beneficial for pain management and contribute to a shorter length of hospital stay for patients undergoing minimally invasive pectus repair operations. In addition, both blockades significantly improved the patient satisfaction. However, there was no difference between the two interventional pain management (PVB versus EDB) procedures in respect of intraoperative opioid requirement, postoperative pain, and patient comfort. Although the results of this study are promising, the comparison of the safety profile and the effectiveness of these interventions require larger studies in this patient population.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.