
Abstract
Abstract
Purpose:
This study analyzes the effect, long-term survival rate, and complications about preserving the left colonic artery (LCAP) in rectal cancer surgery.
Methods:
Relevant articles were systematically retrieved from multiple electronic databases, for example, EMBASE, BioMed Central, PubMed, Web of Science, and Cochrane. The time for retrieving was from the establishment of the database to December 31, 2018. Evaluated endpoints were effect of LCAP on the curative effect of rectal neoplasms, such as operation time, the amount of bleeding during the operation, root lymph nodes positive number, and the related complications (anastomotic leakage, etc.), postoperative urinary retention, 5-year survival rate, and recurrence differences in rates.
Results:
Totally 12 studies were included in this review. The meta-analysis showed that LCAP has less operation time and lower anastomotic leakage incidence. Intraoperative bleeding, root lymph nodes, and other complications did not show any significant difference.
Conclusions:
LCAP in radical rectal cancer surgery ensures both the radical resection of the tumor and the safety of the operation. So it can provide a new approach to the management of blood vessels and lymph nodes.
Introduction
Rectal cancer surgical technology has been continuously improved, and many consensuses have been reached, such as total mesorectal excision (TME), inferior mesenteric artery (IMA) root lymph node dissection, and pelvic autonomic nerve retention. However, the left colonic artery (LCA) should be retained or does not seem to be a lack of consensus. According to the Consensus Statement of Definitions for Anorectal Physiology and Rectal Cancer of the American Society of Colon and Rectal Surgeons, high tie refers to ligate the IMA root and LCA (left colonic artery ligation [LCAL]); low tie means ligate below the IMA to ensure preserving the left colonic artery (LCAP). 1 Whether LCAP will affect or not the perfusion of anastomotic sites and lymph nodes sweep range is unsure. Therefore, the clinical efficacy of LCAP and LCAL is still controversial. 2
This meta-analysis collected data from clinical controlled studies of preserving or not the LCA and analyzed the two vascular lymph node management methods. The differences in long-term survival rate and tumor radical therapy provide evidence for vascular management during resection of rectal cancer.
Methods
Search strategy
Related documents were systematically retrieved in multiple electronic databases, for example, EMBASE, BioMed Central databases, PubMed, Web of Science, and Cochrane. The deadline is December 31, 2018. Following key words were used: left colonic artery, inferior mesenteric artery, rectal, rectal cancer, rectal tumor, high ligation, low ligation, high tie, low tie, etc. Abstracts of all published documents were retrieved manually. The search terms were combined using logical characters (AND/OR/NOT) to obtain preliminary search results.
Inclusion criteria
(1) The types of studies are randomized controlled studies or case–control studies, (2) the subjects of the study are patients who get diagnosed pathologically, (3) cancer with negative upper and lower circumferential margin, (4) high ligation of IMA (no LCA) or low ligation (LCAP), during operation of rectal cancer, (5) the outcome indicators of the analysis are described in the study.
Exclusion criteria
(1) Abstracts, case reports, single cohort study without a control group; (2) preoperative or postoperative radiotherapy and chemotherapy; (3) duplicate studies or research populations have crossovers; (4) difficult to obtain the complete data of perioperative studies; (5) unable to obtain the full text of the studies.
Data extraction and quality assessment
Two independent researchers collected the available information, in accordance with the inclusion and exclusion criteria, to read the topics and abstracts of the relevant literature, to exclude those that are manifestly inconsistent with the inclusion criteria, to read the full text of the documents that may be included, and to finalize the studies to be included, and then cross-check the extracted data. The main contents are as follows: (1) general data: title, author, nationality, total number of cases, number of cases with different ligation methods of IMA; (2) results: the 5-year mortality rate, retrieved lymph nodes, positive metastatic lymph nodes, recurrence, anastomotic leakage, bowel obstruction, surgical site infection, operation time, intraoperative blood loss, and postoperative exhaust time (Table. 1).
Characteristics of the Studies Included in This Meta-Analysis
AR, anterior resection; LAR, low anterior resection; LCAL, left colonic artery ligation; LCAP, left colonic artery preservation; LN, lymph nodes; RCT, randomized clinical trial; TME, total mesorectal excision.
Statistical analysis
We organized the data according to the requirements of the meta-analysis and set up the datasheet and checked it. Data were analyzed using the RevMan 5.3 analysis software. The measurement data statistics were determined by using the weighted mean difference (WMD) or standard deviation (SD). The odds ratio (OR) was calculated to evaluate the dichotomous variables for the oncological and perioperative outcomes. All statistical values were computed with 95% confidence intervals (CI). In addition, the χ2 statistic was used to evaluate heterogeneity among studies. If there was statistical heterogeneity among the studies (I2 > 50%, P < .05), the random effect model was used for meta-analysis. If there was no statistical heterogeneity (I2 < 50%, P > .05), the fixed response model was used for meta-analysis. All hypothetical tests were bilateral, with a level of α = 0.05.
Results
A total of 595 initial kinds of studies were obtained. After using endnote and manual check to remove duplicate and nonmatch studies, 70 studies were obtained. Reading carefully the full text, 38 articles were excluded for the following reasons: (1) unable to access full text and (2) incompatible endpoint and review. Finally, we excluded 26 studies by details: studies that did not investigate metastasis not grouped according to the preserve or not LCA and studies with no valuable date. So, 12 studies were included in this meta-analysis (Fig. 1).
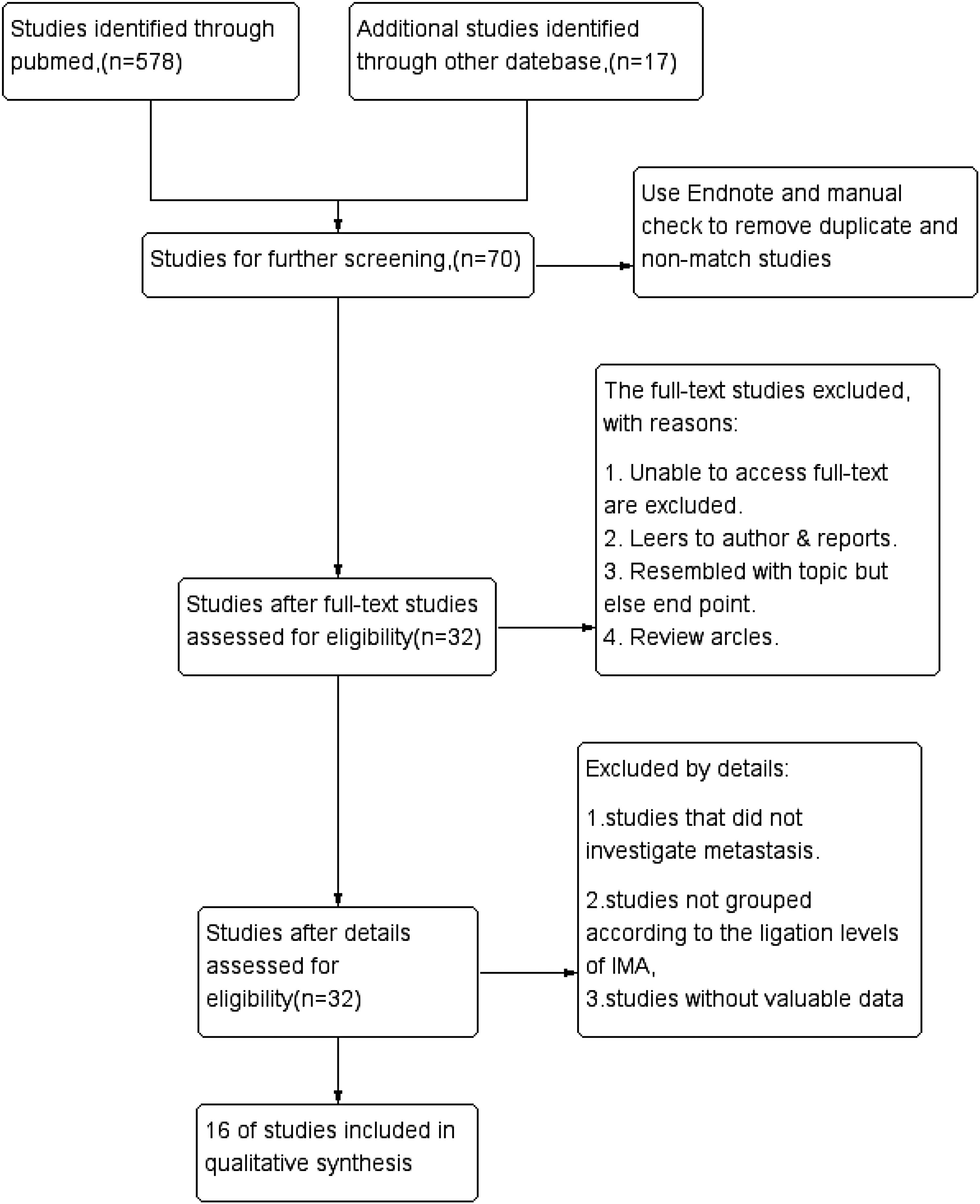
Flow diagram depicting the process of identification and inclusion of selected studies.
Recurrence
The number of postoperative recurrences was recorded in five articles. No heterogeneity was detected in these studies (P = 1.0, I2 = 0%). The fixed-effect models were used for analyses. We failed to find statistical difference (OR = 0.97, 95% CI = 0.81–1.16, P = .74) (Fig. 2).

Forest plot of the recurrence after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Five-year mortality rate
Two articles had recorded a 5-year mortality rate. We could find heterogeneity through these analyses (P < .00001, I2 = 96%), which was carried out by the random effects model. There was no significant difference in 5-year mortality rate between the two groups (OR = 0.35, 95% CI = 0.03–3.78, P = .39) (Fig. 3).

Forest plot of the 5-year mortality rate after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Total number of lymph nodes removed
Four articles reported the total number of lymph nodes dissected. Heterogeneity was detected in the two groups (P < .00001, I2 = 96%). Thus, a random effects model was used to analyze the articles. No statistical distinction was found between the two groups (WMD = −1.03, 95% CI = −3.48 to 1.42, P = .41) (Fig. 4).

Forest plot of a total number of lymph nodes removed after LCAP compared with those after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Root lymph nodes positive number
Four articles reported the root lymph nodes positive number. No heterogeneity was detected (P < .00001, I2 = 96%). Thus, a random-effects model was used for analyses. No statistical distinction was found between the two groups (OR = 0.9, 95% CI = 0.37–2.20, P = .81) (Fig. 5).

Forest plot of the number of root lymph nodes positive after LCAP compared with those after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Operation time
Six articles reported operation time. Heterogeneity was detected in these studies (P < .00001, I2 = 85%). Thus, a random-effects model was used for analyses. The LCAP operation time was obviously shorter than LCAL (WMD = 15.4, 95% CI = 6.75–24.04, P < .0005), showing that there was statistical difference between the two groups (Fig. 6).

Forest plot of the operation time after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Intraoperative bleeding
Six articles reported intraoperative bleeding. Heterogeneity was found in these studies (P = .04, I2 = 69%), which were analyzed by a random effects model. No statistical distinction was found between the two groups (WMD = 1.36, 95% CI = −4.23 to 6.95, P = .63) (Fig. 7).

Forest plot of the intraoperative bleeding after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Anastomotic leakage
Eleven articles reported the number of patients with anastomotic leakage. No heterogeneity was detected (P = .97, I2 = 0%). Thus, a fixed-effects model was used for analyses. In the LCAP group, anastomotic leakage incidence was 4.88% (72/1475), it was lower than that in LCAL, which was 10.38% (75/722) (OR = 0.53, 95% CI = 0.37–0.76, P = 0.0005) (Fig. 8).

Forest plot of the anastomotic leakage after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Bowel obstruction
Three articles reported the number of patients with ileus. No heterogeneity was detected (P = .96, I2 = 0%). Thus, a fixed-effects model was used for analyses. No statistical distinction was found between the two groups (OR = 1.24, 95% CI = 0.66–2.32, P = .51) (Fig. 9).
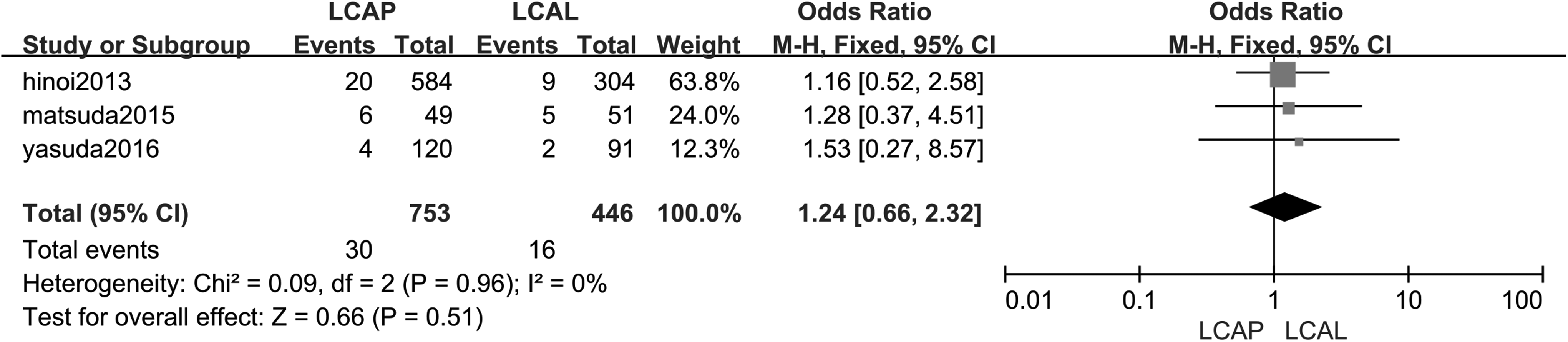
Forest plot of the bowel obstruction after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Surgical site infection
Two articles reported the number of patients with surgical site infection. No heterogeneity was found in these studies (P = .40, I2 = 0%) and the fixed-effects model was used for analyses. No statistical distinction was found in the two groups (OR = 1.10, 95% CI = 0.63–1.92, P = .74) (Fig. 10).

Forest plot of the surgical site infection after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Time to first flatus
Three articles reported the first flatus time. No heterogeneity was found in these studies (P = .62, I2 = 0%) and the fixed-effects model was used for analyses. No statistical distinction was found in two groups (WMD = −0.30, 95% CI = −0.40 to 0.20, P < .000001) (Fig. 11).

Forest plot of time to first flatus after LCAP compared with that after LCAL. LCAL, left colonic artery ligation; LCAP, left colonic artery preservation.
Discussion
In rectal cancer surgery, the debate on whether the LCA should be preserved or not can be traced back to the operation of Miles and Moynihan in 1908, 14 the main points of contention focus on postoperative complications, tumor radical therapy, long-term survival rate, and difficulty of operation, and so on. 15 Hida and Okuno confirmed that LCAL can reduce the tension of anastomotic site, remove the whole IMA lymph node and rectal tumor, and help determine the stage and prognosis of tumor. Although once lymph nodes are positive metastatic, LCAL does not improve long-term survival, the retention of LCA could provide sufficient blood supply to the intestinal tract, avoid complications such as lower ventral nerve injury, dysfunction, and urinary retention, and improve the quality of life effectively.16,17
Today, TME has changed the way of performing rectal cancer surgery, not only the recurrence rate has decreased significantly but also the 5-year survival rate has improved significantly. However, the debate on the treatment of IMA continues to this day. 13 Simultaneously, the National Comprehensive Cancer Network (NCCN) guidelines also do not explicitly suggest ligation by IMA. 18
Based on this, this meta-analysis focuses on the surgical effects, oncology detection, and surgical complications.
Statistical analysis of surgical effects showed that the LCAP group has less operation time than the LCAL group, but no obvious find in intraoperative bleeding. With development of laparoscopic technology, the operation becomes easier and further reduces operation time. 19 But the individual differences in intestinal blood vessels intraoperative bleeding did not significantly reduce.
In terms of postoperative recovery, the mean time to first flatus of LCAP is faster. Because of the development of technology, the rectum can be loosened, the nerve plexus can be displayed, and the injury of autonomic nerve in the root can be reduced. Moreover, the preservation of LCA can make the intestine have sufficient blood supply and shortens the recovery time of the intestinal function. 14
About complications, bowel obstruction and surgical site infection do not have obvious differences. But the number of patients with anastomotic leakage in the LCAL group is higher than those in the LCAP group. The three diseases affect each other and promote each other. As a common complication, anastomotic leakage can lead to death. Blood supply and tension of anastomotic stoma are the most important factors in its incidence. In addition, preoperative chemotherapy, diabetes mellitus, distance from tumor to anal margin, and intraoperative blood loss are all high-risk factors for anastomotic leakage. So, its incidence is as high as 5–26%.20–23
If the LCA is removed, the mesocolon can be loosened and a larger, freer proximal stump of the colon can be obtained. When anastomosis is performed, the tension-free anastomotic site can be guaranteed and the occurrence of anastomotic leakage can be reduced. However, we should not ignore the reduction of blood perfusion at the proximal stump of the colon caused by high tie.
After removing the LCA, blood supply of the anastomosis site comes from the marginal arterial arch and Riolan arch. But anatomy shows that these arches are sometimes missing. 24 During operation, it is not a concern whether one or two colon arteries are ligated. Intestinal ischemia and necrosis will not occur if the marginal artery arch is not damaged. Integrity, patency, and perfusion of the marginal arterial arch are the keys to the survival of the intestinal canal. 25 At the spleen curve, marginal artery arch at the junction of the descending colon and the transverse colon is called Griffiths. The existence, weakness, and lack of Griffiths in the population percentage are 48%, 9%, and 43%, respectively. If patients are weak or lack Griffiths, the likelihood of a blood vessel disorder in the proximal bowel is increased. 26
The Riolan vascular arch is derived from the middle colon artery, descending to the left along the duodenum and anastomosing with the ascending branch of LCA. It is thinner than the marginal artery and does not send out straight blood vessels to the intestinal wall, but connect the two mesenteric arteries. 27 Riolan vascular arch improves the collateral circulation of colon blood supply, but the rate of existence of this arch is only 7.6%. 28
So, it is suggested that if LCA is removed in the operation, blood perfusion of the peripheral colon stump mainly comes from the marginal artery from the middle colon artery and Riolan arch.
It is obvious that the blood supply of anastomotic mouth is an independent risk factor and can increase the occurrence of anastomotic leakage. 29 According to the results of Color Doppler Flow Imaging (CDFI), Seike et al. believed if LCA was resected during surgery that the blood supply fraction at the cut end of the colon would decrease significantly and that it is also age related. The older the age, the more decline is obvious.16,31 However, Cirocchi et al. think that although high ligation of IMA may reduce the blood supply of the distal intestinal tube, compared with LCAP, high ligation of IMA can satisfy the minimum blood supply of anastomotic healing, and if the simple marginal vascular supply of the anastomosis meets the minimum blood supply of anastomotic healing, high ligation does not cause more anastomotic leakage. 16
On the contrary, low tie can direct supply of blood to the marginal artery of the colon by LCAP and reduce the adverse effects due to lack of Griffiths and Riolan arterial arch. At the same time, with the development of surgical techniques, it is not difficult to release spleen flexure technically, and tension-free anastomosis can also be achieved.
Komen et al. used laser Doppler blood flow meter and Sung et al. used near-range infrared fluorescence imaging technology to measure the blood supply of anastomotic stoma after operation. It was proved that the blood supply of the marginal artery in LCAP was much fuller. So, it was suggested that LCAP could provide more sufficient blood supply for anastomosis. 5 Hinoi et al., in a retrospective study of 28 Japanese hospitals and randomized clinical trial study of Guo et al., also found that LCAP could guarantee a lower incidence of anastomotic leakage.
This meta-analysis also confirmed that retaining LCA can effectively reduce the occurrence of anastomotic leakage.6,7 Therefore, it is reasonable to think that good blood perfusion can promote the rapid healing of anastomotic sites to a certain extent. Preserving the IMA and LCA can ensure a good blood supply, prevent the occurrence of anastomotic leakage, or promote the healing of anastomotic leakage.
Statistical analysis of oncological outcomes show no significant difference between the number of lymph nodes removed or the number of positive lymph nodes. The root lymph node is between the beginning of IMA and the beginning of LCA. As the third lymph node drainage station, it is the main avenue for metastasis of rectal cancer.
For rectal malignant tumors, the metastatic rate of IMA root lymph nodes has great significance for histological classification, differentiation, and prognosis. In addition, the lymph node invasion range directly influenced the cancer metastasis and patient survival time. It is reported that the lymph node metastasis rate of IMA root was 0.7%–11.6% and for the root lymph nodes positive patients, the postoperative recurrence rate can be 67.4%. Therefore, lymph node dissection can receive more accurate postoperative staging in oncology and guide postoperative treatment. It is the key to radical resection of rectal cancer. The statistical results show that LCA-preserving surgery can completely meet the requirements of IMA root lymphadenectomy and obtain a satisfactory prognosis and survival rate.32,33
The most important postoperative observation index is the 5-year survival rate. In the past, it was thought that resection of LCA could effectively improve.34 However, the results of meta-analysis give the opposite conclusion. At the same time, Cirocchi et al. believe that high tie cannot reduce tumor invasion. 16 For rectal malignant tumors, the degree of lymph node involvement directly influences the survival time. No significant difference was detected in the number of positive lymph nodes because of the same scope of lymph node dissection in LCAL and LCAP. Although they were positive lymph nodes, after radiotherapy and chemotherapy, some lymph nodes had little effect on patient survival.
Conclusion
This meta-analysis believed that retaining LCA can provide both root lymph node dissection and fuller blood supply to the intestines. It can not only meet the requirements of radical resection of the tumor but also reduce the occurrence of complications such as anastomotic leakage.
Footnotes
Disclosure Statement
The authors declare that there is no conflict of interest. No competing financial interests exist.