
Abstract
Abstract
Introduction:
Major colorectal surgery procedures are complex operations that can result in significant postoperative pain and complications. More evidence is needed to demonstrate how opioid-related adverse drug events (ORADEs) after colorectal surgery can affect hospital length of stay (LOS), hospital revenue, and what their association is with clinical conditions. By understanding the clinical and economic impact of potential ORADEs within colorectal surgery, we hope to further guide approaches to perioperative pain management in an effort to improve patient care and reduce hospital costs.
Materials and Methods:
We conducted a retrospective study utilizing the Centers for Medicare and Medicaid Services (CMS) Administrative Database to analyze Medicare discharges involving three colorectal surgery diagnosis-related groups (DRGs) to identify potential ORADEs. The impact of potential ORADEs on mean hospital LOS and hospital revenue was analyzed.
Results:
The potential ORADE rate in patients undergoing colorectal surgery was 23.92%. The mean LOS for discharges with a potential ORADE was 5.35 days longer than without an ORADE. The mean hospital revenue per day with a potential ORADE was $418 less than without an ORADE. Any type of open surgery had a statistically significant higher potential ORADE rate than the matched laparoscopic case (P < .001). Clinical conditions most strongly associated with ORADEs in colorectal surgery included septicemia, pneumonia, shock, and fluid and electrolyte disorders.
Conclusion:
The incidence of ORADEs in colorectal surgery is high and is associated with longer hospital stays and reduced hospital revenue. Reducing the use of opioids in the perioperative setting, such as using multimodal analgesia strategies, may lead to positive outcomes with shorter hospital stays, increased hospital revenue, and improved patient care.
Introduction
The dangers of opioid addiction and overdose have reached epidemic proportions in the United States.1,2 However, much less attention has been paid to the harm caused by short-term opioid use in the hospital setting.1–3 With over 73 million patients undergoing inpatient surgical and endoscopic procedures in the United States each year and with more than 95% of those surgical patients receiving opioids during their hospitalization, it is clear that opioid analgesics still remain a foundational part of perioperative surgical pain management.1,4–8 While opioids are effective in pain management, their utility must be balanced against the potential risks of opioid-related adverse drug events (ORADEs) in the perioperative setting, as well as long-term consequences.9–11
ORADEs are a varied group of complications that affect multiple organ systems. 12 In analyses of ORADEs, the logistics of identifying opioid-specific adverse events in administrative data can be challenging as clinicians often do not always utilize the international classification of diseases (ICD) codes specifically related to opioids (e.g., opioid-induced constipation), but rather choose diagnosis codes that generally cover the adverse event itself (e.g., constipation, unspecified). Therefore, to prevent gross underestimation of ORADEs, the methodology of including ICD codes that more broadly cover common ORADEs—such as those listed in Supplementary Table S1—should ideally be utilized.4,6,11
The most common ORADEs broadly range from gastrointestinal effects, central nervous system effects, pruritus/dermatitis, and urinary retention.12,13 More specifically, gastrointestinal effects include nausea, vomiting, and constipation, while central nervous system effects include dizziness, excessive somnolence, decreased psychomotor coordination, and respiratory depression.7,14 National analyses examining ORADE incidence have found that nearly 20% of all patients treated with opioids experience an ORADE, 14 and treatment of ORADEs has been repeatedly shown to increase hospital costs, readmission rates, and lead to longer hospital lengths of stay (LOSs).4,13–15 Although ORADEs have been shown to negatively impact overall patient care and hospital cost, studies have only recently begun examining ORADEs within specific classes of procedures and surgeries.
Major colorectal surgery procedures are complex operations that can result in significant postoperative pain and complications.4,5 Less is known about how ORADEs after colorectal surgery affect hospital LOS, hospital revenue, and their association with clinically relevant diseases during a patient's hospital course. We hypothesized that potential ORADEs are associated with increased LOS, decreased hospital revenue, and have increased associations with specific comorbidities—knowledge of which may allow for more targeted interventions. By understanding the clinical and economic impact of potential ORADEs within colorectal surgery, we hope to further guide both the clinician and hospital administration approach to perioperative pain in an effort to improve patient care and reduce hospital costs.
Methods
Study design
This retrospective study utilized data from the Medicare Limited Data Set (LDS), an administrative claims database from the Centers for Medicare and Medicaid Services (CMS). 16 LDS effectively contains data from all hospitals in the United States that provide care for patients with Medicare, totaling ∼30%–35% of all inpatient hospital discharges.6,11 Three admission diagnosis-related groups (DRGs) were selected to compare the impact of potential ORADEs on specific measures such as hospital revenue, mean LOS, and the associated comorbidities occurring during a patient's hospital course to potential ORADEs within the study population.
Fifty ICD-10 codes were also selected to compare the incidence of potential ORADEs based on laterality of surgery (left versus right), as well as the surgical approach (open versus laparoscopic).
Study population
The study population included all hospitalizations between April 2016 and March 2017 in which patients with Medicare underwent major small and large bowel procedures with major complications or comorbidities (MCC) (DRG 329; 34,884 patients), with complications or comorbidities (CC) (DRG 330; 56,771 patients), or without MCC (DRG 331; 27,450 patients). In total, this comprised a total cohort of 119,045 Medicare discharges who underwent a procedure covered by one of these three DRGs.
ICD-10 codes, representing surgeries with at least 400 cases between April 2016 and March 2017, were also analyzed. In total, this comprised a total of 50 cases who underwent a procedure covered by one of the three DRGs described above.
Measures
The data provided by the LDS database were cataloged by DRGs. Within each DRG, data were further organized by total discharges within each DRG, total CMS payments, potential ORADE rate, mean LOS (total, with potential ORADEs, and without ORADEs), and mean hospital revenue per day (total, with potential ORADEs, and without ORADEs). Using these values, the difference in both hospital revenue and in mean LOS with and without potential ORADEs was determined, thus allowing for the assessment of potential ORADEs on patient care.
Within this data set, hospital revenue is defined as the CMS reimbursement payment and was obtained from the LDS database. More specifically, the hospital revenue per day for each DRG was calculated by totaling the Medicare payments for the DRG cohort and dividing by the total hospitalization days for that specific DRG. Hospital LOS was defined as the total number of days from admission to discharge in both hospitalization with and without potential ORADEs. Due to the LDS database restrictions on the use of specific hospitalization dates, we were not able to calculate specific postsurgical LOS.
Potential ORADEs were determined by analyzing ICD-10 diagnosis codes that were flagged as both not present on admission and are commonly associated with ORADEs. This methodology is consistent with previous research in this area.6,11,12 The included ICD codes are listed in Supplementary Table S1 and include gastrointestinal, central nervous system, respiratory, urinary, as well as other adverse effects potentially related to opioids.
While utilizing the LDS database and ICD codes, further analysis was also conducted to understand the association of specific patient comorbidities present in the study population with potential ORADEs. Using the Agency of Healthcare Research and Quality (AHRQ) Clinical Classification Software (CCS), 17 tens of thousands of ICD codes (over 69,800 diagnosis codes and 71,900 procedure codes) were categorized into groups more suitable for statistical analysis compared to individual ICD-10-Clinical Modification/Procedural Classification System codes. From these groups, 21 categories were selected based on their clinical relevance and statistical significance as related to potential ORADEs within DRGs 329–331 of major small and large bowel procedures.
Analysis of specific procedural ICD-10 codes was also conducted to further understand how the potential ORADE rate may change depending upon the laterality in surgery, as well as the surgical approach (open versus laparoscopic). ICD-10 codes from DRGs 329–331 were obtained and organized by total number of cases. ICD-10 codes with at least 400 cases were included, which comprised a total of 50 ICD-10 codes. Using www.coder.aapc.com, each ICD-10 code's medical classification was obtained. These medical classifications were organized based on the type of surgery (resection, excision, bypass), laterality (left, right, none), anatomical location, and approach (open versus laparoscopic).
In our analysis of laterality, ICD-10 codes were matched by exactly each aspect of their medical classification except for whether the case was performed on the left or right to minimize any confounding variables. For instance, a resection of the right large intestine performed through open approach was matched to a resection of the left large intestine also performed through open approach.
In our analysis of surgical approach, ICD-10 codes were also matched by each aspect of their medical classification except for whether the case was performed as open versus laparoscopic. For instance, a resection of the left large intestines performed through open approach was matched to a resection of the left large intestines performed through laparoscopic approach.
Statistical analysis
CMS payments are expressed in U.S. dollars as the total sum of all revenue from hospital discharges within each DRG. LOS is expressed as days and is the mean of all hospital discharges within each DRG. A multivariable regression analysis was utilized to determine the odds ratio (OR) of a potential ORADE for each specific CCS category. A P value of <.05 was considered statistically significant for analyses of hospital revenue, LOS, and CCS categories, which were performed using SAS version 9.4 (SAS, Cary, NC). This multivariable regression analysis was compiled into a Forest plot as demonstrated in Figure 1. In this multivariable analysis, the reference CCS categories were “male” and “age <65,” which were thus not included in Table 3 or Figure 1. In the analysis of specific procedural ICD-10 codes, the potential ORADE rate is expressed as a percent. A P value of <.001 was considered statistically significant in our analysis of ICD-10 codes, which was conducted using a t-test on Microsoft Excel (version 16.26).
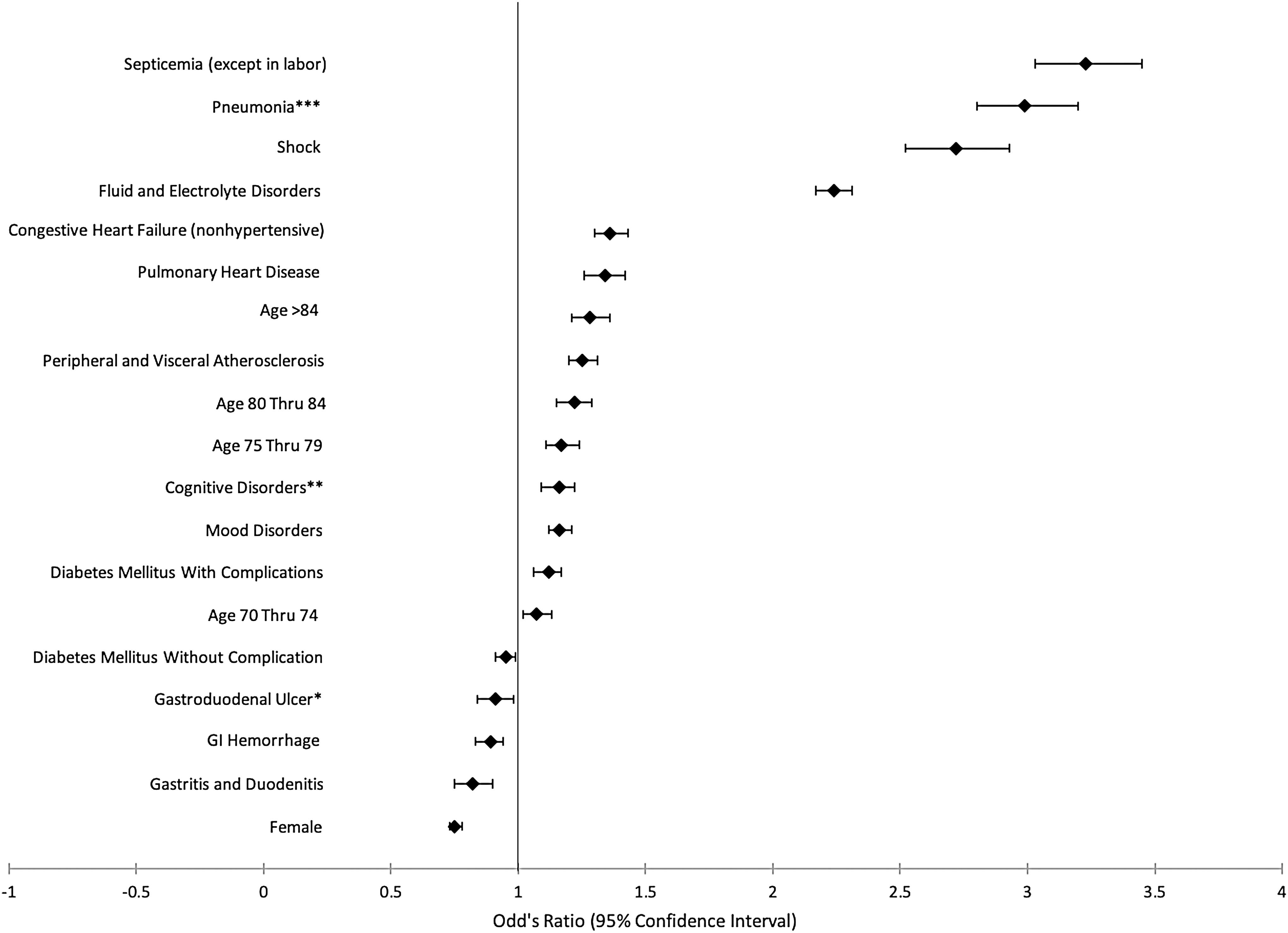
Multivariable association between potential ORADEs and AHRQ CCS categories among colorectal surgery DRGs 329–331. *Except hemorrhage; **cognitive disorders include delirium, dementia, amnestic, and other cognitive disorders; ***except that caused by tuberculosis or sexually transmitted disease. AHRQ, Agency of Healthcare Research and Quality; CCS, Clinical Classification Software; DRG, diagnosis-related group; ORADE, opioid-related adverse drug event.
Results
Tables 1 and 2 summarize the impact of potential ORADEs on LOS and its effect on hospital revenue in colorectal surgery. The overall potential ORADE rate in the three DRG groups for small and large bowel procedures was 23.92% (28,476 out of 119,045 records analyzed). The mean LOS for discharges with a potential ORADE was 5.35 days longer than without an ORADE (12.34 days with a potential ORADE versus 6.99 days without an ORADE; P < .001). The mean hospital revenue per day with a potential ORADE was $418 less than that without an ORADE ($2,931 with a potential ORADE versus $3,349 without an ORADE; P < .001).
The Impact of Potential ORADEs on Length of Stay in Colorectal Surgery
CC, complications or comorbidities; DRG, diagnosis-related group; LOS, length of stay; MCC, major CC; ORADE, opioid-related adverse drug event.
The Impact of Potential Opioid-Related Adverse Drug Events on Hospital Revenue in Colorectal Surgery
CC, complications or comorbidities; CMS, Centers for Medicare and Medicaid Services; DRG, diagnosis-related group; MCC, major CC; ORADE, opioid-related adverse drug event.
As can be seen in Tables 1 and 2, each DRG group represents a small and large bowel procedure, but they are also characterized by the severity of CC, if any. For instance, DRG 329 are cases with MCC, DRG 330 are cases with CC, and DRG 331 is without any MCC or CC. This allows for analysis of each DRG and the impact of potential ORADEs on hospital revenue and LOS within each DRG. The potential ORADE rate for DRG 329 is the highest at 47.36% compared to DRG 330 at 18.42% and DRG 331 at 5.50%. DRG 329 also demonstrates the largest difference in mean LOS for discharges with a potential ORADE at 3.70 days greater than without an ORADE, compared to DRG 330 and DRG 331, which have a mean LOS for discharges with a potential ORADE at 2.28 and 1.09 days greater than without an ORADE, respectively. The mean hospital revenue per day with a potential ORADE in DRG 329 was $671 less than without an ORADE, compared to DRG 330 and 331, which had a mean hospital revenue per day with a potential ORADE of $843 and $499 less than without an ORADE, respectively.
The multivariable analysis of potential ORADEs with AHRQ CCS categories is listed by similar clinical conditions or age group in Table 3, as well as depicted in a Forest plot in Figure 1, going from strongest to weakest association. As seen in Table 3 and the Forest plot in Figure 1, the adverse postoperative outcomes that were most strongly associated with potential ORADEs included septicemia, pneumonia, shock, and fluid and electrolyte disorders. Older age was associated with adverse postoperative outcomes, with individuals aged 84 and greater having the greatest OR among age groups (OR: 1.28, 95% confidence interval [CI]: 1.21–1.36), followed by individuals aged 80–84 (OR: 1.22, 95% CI: 1.15–1.29), then individuals aged 75–79 (OR: 1.17, 95% CI: 1.11–1.24), and finally, individuals aged 70–74 (OR: 1.07, 95% CI: 1.02–1.13). Patients who had complications secondary to diabetes (OR: 1.12, 95% CI: 1.06–1.17) demonstrated a stronger association with potential ORADEs than patients without diabetic complications (OR: 0.95, 95% CI: 0.91–0.99). Patients with mood (OR: 1.16, 95% CI: 1.12–1.21) and neurologic disorders (OR: 1.16, 95% CI: 1.09–1.22) had nearly equally increased association with potential ORADEs.
Multivariable Association of Potential Opioid-Related Adverse Drug Events with Demographic Factors and Medical Conditions Based on the Clinical Classification Software Disease Categories
CCS, Clinical Classification Software; CI, confidence interval; ORADE, opioid-related adverse drug event.
Analysis of ICD-10 codes based on laterality was focused on four ICD-10 codes, which were organized into two pairs, one being resection of the right versus left large intestines (open approach) and the other being resection of the right versus left large intestines (laparoscopic approach). The potential ORADE rate for resection of right large intestines (open approach) and for resection of left large intestines (open approach) were 27.63% and 30.94%, respectively. The potential ORADE rate for resection of right large intestines (laparoscopic approach) and for resection of left large intestines (laparoscopic approach) was 17.11% and 16.54%, respectively.
Analysis of ICD-10 codes defining the surgical approach was focused on 32 ICD-10 codes, which were organized into 16 pairs. As can be seen on Figure 2, patients undergoing any type of open surgery (bars in black) had a statistically significant higher potential ORADE rate than their matched laparoscopic case (bars in gray) with a P value <.001.
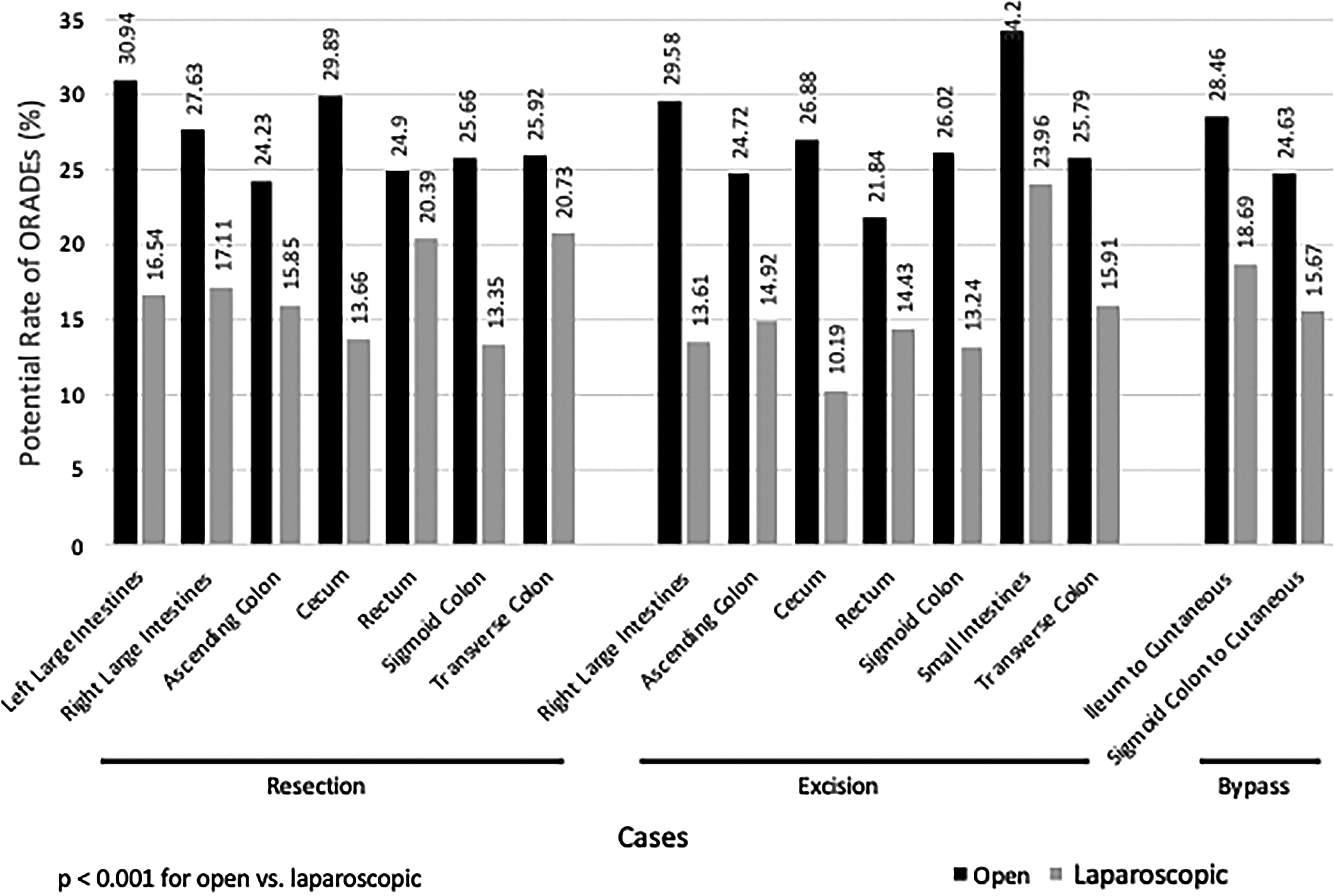
The incidence of potential ORADEs in open versus laparoscopic cases. Patients undergoing any type of open surgery (bars in black) had a statistically significant higher potential ORADE rate than their matched laparoscopic case (bars in gray) with a P value <.001. ORADE, opioid-related adverse drug event.
Discussion
In this study, we analyzed the impact of potential ORADEs on patients undergoing colorectal surgery and found that cases with potential ORADEs were associated with overall increased mean hospital LOS by 5.35 days and decreased hospital revenue by $418 per day. In addition, potential ORADEs were found to be most strongly associated with certain postoperative outcomes such as septicemia, pneumonia, shock, and fluid/electrolyte disorders.
Opioid analgesics are currently a fundamental part of perioperative surgical pain management. However, while they are effective in the postsurgical setting, their activity at peripheral receptors throughout the body can lead to the negative consequences of ORADEs. 7 Thus, the benefits of opioids in postsurgical pain management must be carefully weighed against their adverse effects, which can result in patient harm as well as increased costs.9–11
We hypothesized that the findings in this analysis of an association between potential ORADEs and longer LOS are most likely a result of the subsequent time needed to treat a broad range of adverse effects. These would include minor and major ORADE types listed in Supplementary Table S1, such as pruritus, nausea, vomiting, constipation, paralytic ileus, altered mental status, somnolence, disorientation, falls, acute respiratory failure, hypoxemia, aspiration pneumonia, and urinary retention. A large retrospective study by Suh et al. focused on all hospitalized patients—not simply those undergoing colorectal surgery—and essentially had similar findings whereby in their study out of 434,034 hospitalized patients, 55% required treatment for nausea, vomiting, or constipation after administration of opioids. 18 A recent study by Urman et al. analyzed the prevalence, risk factors, and outcomes of ORADEs in previously opioid-naive patients who underwent surgery. The authors found that 91% of patients received postoperative opioids, and of those patients, 9.1% had a potential ORADE. 19 In addition, the authors found that presence of a potential ORADE was associated with 32% higher costs of hospitalization, 45% longer postoperative LOS, 36% lower odds of discharge home, and 2.2 times the odds of death. Thus, costs will increase without the commensurate increase in reimbursement from Medicare.
In addition, our finding of an association of potential ORADEs with decreased hospital revenue per day is likely connected to treatment of the adverse effects of opioids. A prolonged hospital course most likely would require continued monitoring by medical staff and various treatment regimens and interventions depending on the type of ORADE encountered. 7 A prolonged hospitalization can result in subsequent hospital-acquired infections such as hospital-acquired pneumonia (in cases of respiratory depression or prolonged time on the ventilator) or a urinary tract infection (in cases of urinary retention or instances requiring urinary catheter placement).20,21 Our data agree with other studies in surgical and laparoscopic procedures, which have shown an association between potential ORADEs and worse patient outcomes, higher likelihood of discharge to a care facility rather than home, increased inpatient mortality, and a higher rate of 30-day readmission.1,4,6,11,22,23
As shown in Table 3 and Figure 1, CCS disease categories that most associated with potential ORADEs during a patient's hospital course included septicemia, pneumonia, shock, and fluid/electrolyte disorders. Since opioids have the ability to cause respiratory depression and decrease a patient's mental status, it is not surprising that pneumonia is a strongly associated CCS condition with potential ORADEs. The association of sepsis and shock with potential ORADEs is consistent with findings in previous studies that demonstrated the potential of opioids to suppress the immune response and increase the patient's vulnerability to infections. 24 Similarly, previous epidemiological studies have found that high doses and the initiation of opioid therapy for nonmalignant pain have been correlated with a higher risk of infection such as pneumonia. 25 The specific immunomodulatory effects of opioids are likely due to their inhibitory effects on cellular and humoral immune responses—such as antibody production, cytokine expression, phagocytic activity, and natural killer cell activity 24 —thus placing patients at higher risk for septicemia and shock, both of which were strongly associated with potential ORADEs in our study.
Interestingly, Table 3 and Figure 1 also illustrate the increasing association of potential ORADEs with age, showing a stepwise increase in OR from ages 70 to >84, although at times with crossing CIs between consecutive age groups. Nevertheless, this demonstrates the particular vulnerability of the elderly population to the development of ORADEs, some of which can be explained by altered pharmacokinetics and pharmacodynamics such as lower volume of drug distribution, as well as reduced renal and hepatic metabolism.26,27
To further understand the rate of potential ORADEs, we analyzed the laterality of 50 ICD-10 codes within the DRGs 329–331. However, given the limited abdominal procedures that have laterality, there were only four ICD-10 codes which would allow for left versus right analysis. The potential ORADE rate for resection of the right versus large intestines in the open approach was 27.63% and 30.94%, respectively. Similarly, the potential ORADE rate for resection of the right versus large intestines in the laparoscopic approach was 17.11% and 16.54%, respectively. Therefore, this analysis shows that there is no significant difference between the same surgery performed on the right versus the left side, suggesting that the rate of ORADEs is not associated with the laterality of an abdominal surgical procedure.
However, Figure 2 illustrates how the potential rate of ORADEs is consistently associated with a statistically significant higher rate in all cases using the open surgical approach compared to the same surgery undergoing a laparoscopic approach (P < .001). This is repeatedly demonstrated in each abdominal surgery regardless of its anatomical location in the abdomen and whether it was a resection, excision, or bypass. This analysis demonstrates an association of a higher rate of potential ORADEs in more invasive surgical cases compared to laparoscopic cases, most likely due to the increased use of opioids during the surgery, as well as within postoperative recovery. These findings are congruent with a previous study that found open thoracic procedures were associated with a higher risk of prolonged opioid use compared to minimally invasive thoracic procedures. 28 With prolonged opioid use, patients are exposed to a greater potential for ORADEs and their subsequent complications. By demonstrating an association between a higher rate of ORADEs in more invasive surgical cases, this analysis further aims to establish an increasing association between the inherited complexity of a surgical procedure and the potential rate of ORADEs.
To improve health care quality and reduce complications, the Department of Health and Human Services in 2014 called for better systems to monitor ORADEs. 29 As a response, Stone et al. developed a framework using the data from the CMS National Administrative Database that identifies potential ORADEs that can be used for internal institutional use, benchmarking, and research. Our current work builds on this study as we focus on the impact of potential ORADEs in specific surgical subspecialties such as colorectal surgery. 12 The study of potential ORADEs in our study provides additional insight into how health care providers can improve their practices to prevent future ORADEs. On the institutional level, quality improvement projects designed to evaluate inpatient and outpatient opioid prescription and administration practices are one major way that hospitals are tackling the negative consequences of opioids. 30 With the findings of this study, hospital-based programs can utilize this information to further develop their curriculum and educate providers on the safe use of opioids. Practical clinical recommendations that focus on creating specific opioid order sets and maintaining updated guidelines on opioid use in acute, as well as chronic pain are some important quality measures that may also further prevent ORADEs and their consequences on the health care system.
An essential quality measure continually being developed is the use of multimodal analgesia. The purpose of multimodal analgesia is to recognize that pain is multifactorial and then to use multiple agents or interventions to treat a patient's pain, using an individualized approach based on patient- and surgery-related factors.4,31 This allows for the clinician to reduce the total dosage of opioid required and thus decrease the patient's risk for an ORADE. Past studies have illustrated both the negative effects of opioids and their poor ability to alone properly control pain, given that up to 75% of patients still report continued pain after surgery.4,32,33 This indicates that not only is the use of opioids harmful, it is also not necessarily effective for postsurgical pain. For this reason, it is critical to avoid utilizing only a single agent (i.e., opioids) but rather use multimodal analgesia in perioperative pain management.
The American Pain Society and American Society of Anesthesiologists guidelines recommend the use of at least two modalities in a stepwise approach, starting with nonopioid analgesics or methods to the use of opioids.34,35 Nonopioid options may include oral or intravenous nonsteroidal anti-inflammatory drugs, acetaminophen, short-acting local anesthetics, and regional blocks. Patient-controlled analgesia also serves as an appropriate modality to managing pain, as well as an effective use of opioids. While these options are certainly known to provide pain relief, it is important to recognize that more research is needed to understand the most effective combinations of nonopioid and opioid agents for perioperative pain management.
While minimizing opioid use and maximizing the diversity of nonopioid analgesics is a reasonable goal, it is important to recognize the production pressure on clinicians that may also be contributing to opioid overuse. For instance, postsurgical pain relief is often considered a fundamental right for patients, and hospitals providing inadequate pain relief may face low scores on public patient satisfaction surveys and, consequently, lower reimbursement rates.36,37 In addition to patient pain relief and patient satisfaction, there is also the concern of acute postoperative pain leading to chronic pain, which occurs in 10%–50% of patients. 38 Inadequate postsurgical pain has also been shown to increase morbidity and suffering in patients.38,39 These are all likely contributing factors to the clinician's pressure to utilize opioids, but with the use of multimodal analgesia, clinicians can provide their patients with adequate pain control, while simultaneously decreasing their risk for ORADEs.
While optimizing pain regimens and improving patient care is a high priority, the economics involved in ORADEs must also be considered. While there can be ambiguity regarding the cost to a hospital for a minor extension in a patient's hospital course, there is no doubt that an increased LOS of 5.35 days is economically damaging to hospital revenue. Thus, to improve both economic yield and patient care, it is essential to consider institution-wide implementation of enhanced recovery pathways (ERPs) that focus on—among other recommendations—reduced opioid consumption and improved utilization of multimodal analgesia. 13 Recent guidelines for perioperative care in elective colorectal surgery from the Enhanced Recovery After Surgery (ERAS) Society and American Society for Enhanced Recovery (ASER) specifically advocate for multimodal analgesia and minimization of opioids.40,41 ERPs were initially described in open colorectal surgery, but have since been implemented in a broad range of surgical subspecialties. 42 While ERPs were designed to reduce the medical and economical burdens of surgical complications, they may also have the potential to avoid ORADEs, thus further reducing LOS and improving hospital revenue. In recent studies, ERPs have been shown to reduce complications, decrease hospital stays, and allow for earlier resumption of normal activities such as bowel function and mobilization.43,44 Taking into account the findings of this analysis, we believe that utilization of ERPs will likely reduce ORADEs while simultaneously decreasing hospital LOSs, improving hospital revenue, and reducing surgical complications.
Within this study, there are several limitations that warrant discussion. It is a retrospective study utilizing an administrative database. In addition, while an association between potential ORADEs and certain outcomes, as well as diagnoses, was made, this does not establish a causal relationship from opioid use in pain management, just a possible association. Since adverse events were determined by ICD codes, this may have resulted in an overestimation of ORADEs and their association to LOS and hospital revenue. Further contributing to this inflation is that the Medicare database does not specifically describe the medications administered during each hospitalization or the timing of each medication administration to an adverse event. In contrast, the incidence of ORADEs may also be underestimated as hospitals can only submit a limited number of ICD codes and often only link the most severe complications to claims data, thus possibly underreporting common adverse events such as nausea, vomiting, constipation, delirium, and pruritus. Nevertheless, the large number of hospitals included in the Medicare database, the methodology for identifying potential ORADEs, and the associations formed using the AHRQ CCS categories provided insight into potential ORADEs and their impact on patients undergoing colorectal surgery.
Future research efforts should focus on conducting prospective cohort studies that specify the medications given during every hospitalization and the timing of adverse events in relation to drug administration to establish a more definitive cause–effect relationship between opioids and adverse events in colorectal surgery. Additional research into various types of multimodal analgesia regimens to determine which is most effective would also be beneficial in understanding optimal pain management strategies.
Conclusions
The incidence of minor and major ORADEs in colorectal surgery is high and is associated with longer hospital stays and reduced hospital revenue. Clinical conditions that most strongly associated with ORADEs in colorectal surgery include septicemia, pneumonia, shock, and fluid and electrolyte disorders. Reducing the use of opioids in the perioperative setting using strategies such as multimodal analgesia may lead to positive outcomes with shorter hospital stays, increased hospital revenue, and improved patient care.
Footnotes
Disclosure Statement
N.R.: Employed by Dexur Research and Analytics; R.D.U.: Received funding for unrelated work from Mallinckrodt Pharmaceuticals, Medtronic, and Merck; and J.H., E.Y.B., E.E.W.: no competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. However, the data were provided by Dexur Research and Analytics, New York, NY.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.