
Abstract
Abstract
Background and Aim:
In recent years, minimally invasive surgical approaches have gained an increasingly important role in hepatobiliary surgery. The aim of this study was to investigate the safety and potential benefits of laparoscopic liver resection (LLR) compared with open liver resection (OLR) for benign liver tumors and lesions.
Patients and Methods:
Between January 2009 and December 2017, 182 patients underwent liver resection for benign liver tumors and lesions at our center. After exclusion of 15 patients, the remaining 167 patients were divided into LLR group (n = 54) and OLR group (n = 113) and were compared with regard to perioperative outcomes. To overcome selection bias, a 1:1 propensity score matching (PSM) was performed. In addition, patients undergoing major hepatectomy were divided into major-LLR and major-OLR groups and perioperative outcomes evaluated.
Results:
After PSM, 35 patients were included in the OLR group and 35 patients in the LLR group. The LLR group had a significantly shorter median intensive care unit (ICU) stay (LLR: 1 [0–4] days; OLR: 1 [0–3] days; P = .009) and median hospital stay (length of stay [LOS]) (LLR: 7 [4–14] days; OLR: 10 [5–16] days; P < .001). There were no statistically significant differences in postoperative complications graded as Clavien–Dindo ≥III (LLR: 11.4%; OLR: 2.9%; P = .375) in both groups. Postoperative 90-day mortality was 0% in both groups. When comparing major-LLR (n = 8) with major-OLR (n = 59), patients in the major-LLR group had a significantly longer median operation time (major-LLR: 403 [240–501] minutes; major-OLR: 221.5 [111–529] minutes; P < .001), but a significantly shorter median LOS (major-LLR: 7 [5–14] days; major-OLR: 9 [7–129] days; P = .013). The rate of major complications (Dindo Classification ≥III) for major-LLR was 0% and for major-OLR it was 16.9% (P = .207).
Conclusion:
Our case-matched study demonstrates shorter ICU and hospital stay using laparoscopic techniques while maintaining high-quality perioperative outcomes. Based on our findings, we suggest preferring the LLR over OLR for benign liver tumors and lesions regardless of the resection extent.
Introduction
At present, minimal-invasive approaches have gained wide acceptance as the method of choice for a vast variety of abdominal surgeries. They have become the gold standard for common abdominal procedures such as appendectomy, cholecystectomy, colectomy, and bariatric surgery.1–4 The development of laparoscopic liver resection (LLR) remained restricted because of the complexity of the techniques as related to intraoperative safety in case of hemorrhage and oncologic outcomes.
LLR for benign tumors was first reported in 1991 by Reich et al. 5 but has only gained increased consideration in recent years, because of advances in both technology and technical skills. 6 In 2000, Cherqui et al. published a feasibility study, showing that LLR is a safe and feasible approach for left hepatectomy, left lateral resection, segmentectomy, and partial resection of the Segments III–VI. 7 The First International Conference on Laparoscopic Liver Surgery in Louisville in 2008 stipulated the left-lateral LLR as the gold standard, whereas laparoscopic major hepatectomies were considered to be at an explorational stage. 8
Meanwhile, several studies have shown LLR to be feasible and safe, associated with decreased postoperative complication rates, shorter hospital stay, and reduced blood loss (BL) while ascertaining survival rates comparable with liver resection by open approach.9–14
So far only a limited number of studies have been published focusing on the benefits for laparoscopic surgery for benign liver tumors.15–18 Farges et al. published the first prospective study comparing LLR to open liver resection (OLR) for up to two segments for benign liver tumors in 42 patients. 15 Herein, patients in the LLR group had a significantly shorter hospital stay and comparable postoperative outcomes. Another case-matched study investigated left-lateral resections for benign liver tumors and lesions in 92 patients and demonstrated benefits of the laparoscopic approach regarding duration of operation, BL, duration of hospital stay, and total cost of hospitalization. 17
The aim of this study was to compare perioperative outcomes of patients with benign liver tumors and lesions being scheduled for laparoscopic and open surgery, respectively, by performing a propensity score-matched analysis. Furthermore, we aimed to evaluate perioperative outcomes after major hepatectomies by comparing major-LLR with major-OLR.
Patients and Methods
We retrospectively reviewed 182 patients, who underwent a liver resection for benign liver tumors and lesions at the Department of Surgery, Campus Charité Mitte and Campus Charité Virchow-Klinikum from January 2009 to December 2017. The primary aim of this study was to evaluate the safety and feasibility of LLR for benign liver tumors and lesions. Thus, we compared short-term outcomes of patients undergoing liver resection by laparoscopic approach with those by conventional open approach. The study was approved by the local ethics committee (EA2/006/16).
Patients with the diagnosis of an adenoma (hepatocellular adenoma, cystadenoma, and biliary cystadenoma), focal nodular hyperplasia (FNH), hemangioma, and cysts with parenchymal liver resection were included. Exclusion criteria were additional abdominal surgeries, such as multivisceral resections, trisectonectomies, and additional malignant diseases of the liver. A total of 167 patients met the inclusion criteria and were included in the study (Fig. 1). Patients were divided into LLR (n = 54) and OLR (n = 113) groups.

PRISMA 2009 flow chart for inclusion criteria. LLR, laparoscopic liver resection; OLR, open liver resection; PSM, propensity score match.
Operation methods
Three different laparoscopic approaches were undertaken at our department. The multi-incision laparoscopic liver resection (MILL) was performed by a 12 mm trocar, placed in the umbilical region and additional 12 and 5 mm trocars as needed. A supplementary incision is required to retrieve the resected liver.
For the hand-assisted laparoscopic surgery (HALS), a 6–7 cm epigastric incision was required to place a handport additional to 12 and 5 mm trocars that were inserted as needed. The specimen was retrieved at the end of the operations through the handport incision, so no additional incision was needed.
If the lesion was located in segment II or III, a single incision laparoscopic liver resection (SILS) was performed in some cases by a 4–5 cm incision through the umbilicus.
All techniques were performed in French position. A laparoscopic ultrasound was routinely performed intraoperatively.
Indications for surgery
According to the European Association for the Study of the Liver (EASL) guidelines for benign liver tumors, indications for a resection included symptomatic or growing lesions, including pedunculated or large lesions with associated compression of adjacent organs. Additionally, surgery was indicated when malignancies could not be excluded. When hepatocellular adenomas (HCA) were diagnosed, men were operated on if their lesions were persistently >5 cm and woman were operated on when their lesions were increasing in size. 19
Histological examination of all resected liver specimen was performed postoperatively.
Propensity score analysis and statistical methods
To avoid confounding differences because of baseline varieties between the two groups, we performed a propensity score match. Short-term outcomes were compared between LLR and OLR before and after propensity score matching (PSM).
Before matching, categorical variables were expressed as number or frequency (%) and analyzed using chi-square test and continuous variables were expressed as median (range), and differences between groups were explored using Student's t-test or Mann–Whitney U test. In analysis and comparison of preoperative covariates and outcome parameter after PSM, Student's t-test or Wilcoxon signed-rank test for continuous variables and McNemar test for categorical variables were used after matching.
One-to-one matching without replacement was adopted to overcome bias arising from lack of randomization because of the different covariable distribution among patients.
The propensity score was generated with the preoperative characteristics including sex, age at time of surgery, body mass index (BMI), American Society of Anesthesiologists (ASA) score, resection extent, steatosis, and fibrosis grade of the liver. All surgical procedures were classified according to the Brisbane 2000 nomenclature of liver resection. 20 According to the nomenclature, we classified wedge resections, subsegment resections, segment resections, and left-lateral resections as minor resections, whereas right hemihepatectomies, left hemihepatectomies, right extended hemihepatectomies, and left extended hemihepatectomies were classified as major resections. Thus, patients with data record limitations were excluded from the PSM.
Postoperative complications within 30 days were evaluated according to the Clavien–Dindo Classification ≥III. 21 In addition, intraoperative BL was calculated according to a hemoglobin (Hb)-based formula 22 :
where BV is the patients' blood volume before surgery in mL; Hbt, total amount of Hb of the transfusion in g; H, height in m; W, weight in kg; for men k1 = 0.3669, k2 = 0.03219, and k3 = 0.604; for women k1 = 0.3561, k2 = 0.03308, and k3 = 0.1833. A unit of banked blood was considered to contain 52 g Hb.
To predict the surgical difficulty of liver resection, a novel model for prediction of pure LLR by Hasegawa et al. was adopted before and after PSM. 23 Hereby, four factors were taken into account: extent of resection (scored 0, 2, or 3), location of tumor (scored 0, 1, or 2), obesity (scored 0 or 1), and platelet count (scored 0 or 1). The scores were summed to classify surgical difficulty into three levels: low (total score ≤1), medium (total score 2–3), and high (total score ≥4). Major hepatectomies were defined as resection of ≥3 segments.
The 1:1 nearest neighbor matching without replacement was carried out using the Match package in software R. Statistical analyses were carried out using IBM SPSS Statistics 23 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.). Statistical significance was set at P < .050.
Results
During the study period, 167 patients underwent liver resection for benign liver tumors and lesions and met the inclusion criteria.
The most common indication for liver resection constituted adenomas with 50% (n = 27) in the LLR group and 34.5% (n = 39) in the OLR group. Other indications were hemangioma (LLR: 13%, n = 7; OLR: 22.1%; n = 25), FNH (LLR: 29.6%, n = 16; OLR: 23.0%, n = 26), hydatid cysts (LLR: 5.6%, n = 3; OLR: 15.9%, n = 18), and liver cysts (LLR: 1.9%, n = 1; OLR: 4.4%, n = 5; Fig. 2).
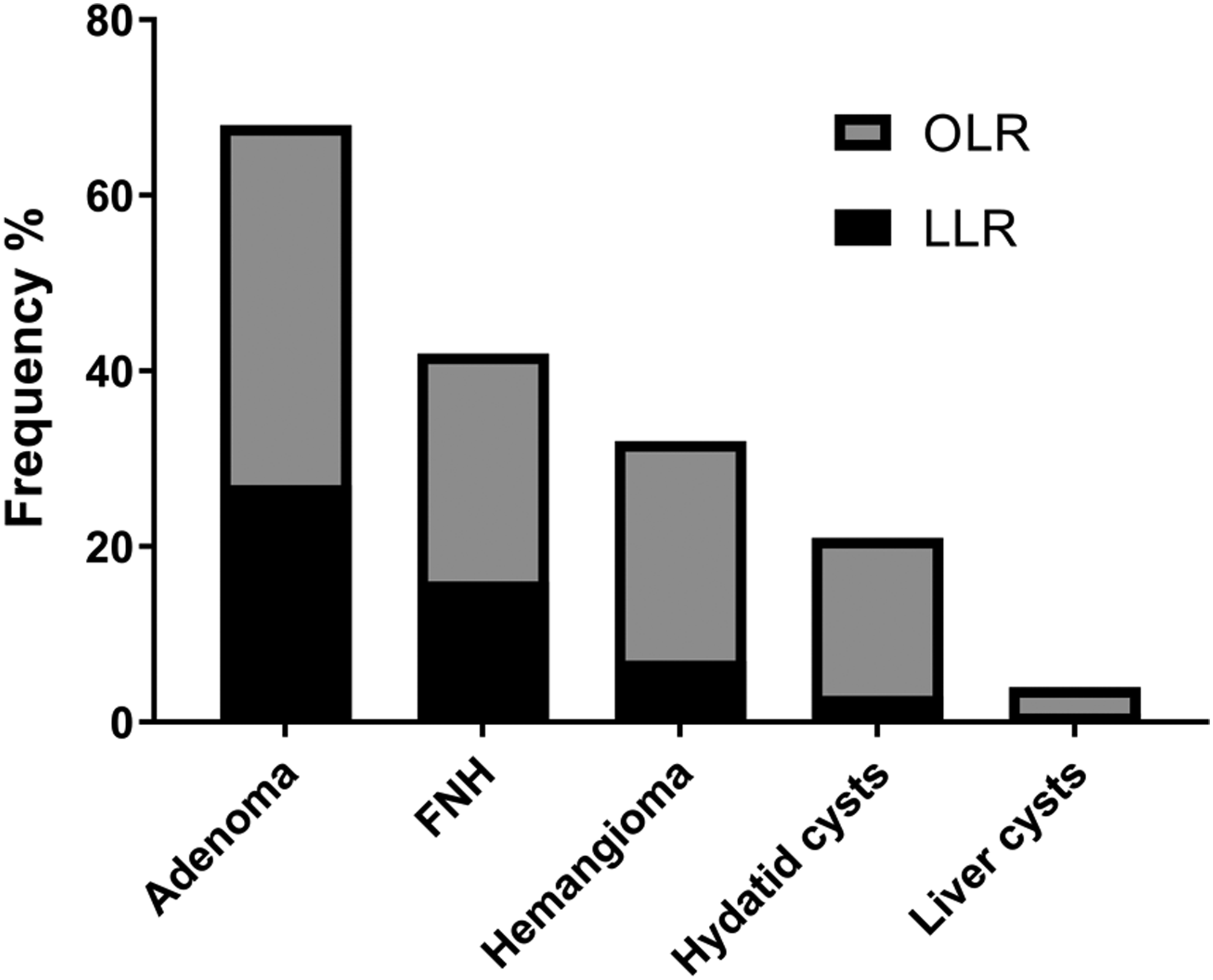
Incidences of benign liver tumors and lesions compared between OLR and LLR groups. FNH, focal nodular hyperplasia; LLR, laparoscopic liver resection; OLR, open liver resection.
A total of 113 patients (67.7%) underwent OLR and 54 (32.3%) underwent LLR. MILL resection was performed in 44 cases (81.5%) followed by SILS (n = 6, 11.1%) and HALS (n = 4, 7.4%). In 1 patient conversion from laparoscopic approach to open approach was required (1.9%).
We observed a shift toward LLR over the years. In the past 2 years we consistently performed more than twice as many LLR than OLR (2016: 73.1%, 2017: 88.9%). After PSM, 35 patients remained in the OLR and 35 patients in the LLR group.
Baseline characteristics of PSM
The patient groups did not differ regarding sex, age at time of operation, BMI, ASA score, liver steatosis, and fibrosis level. The median age was 40 years (12–76 years) for patients operated by laparoscopic approach and 41 years (9–70 years) for patients operated by open approach. The majority of patients were women (LLR: n = 42, 77.8%; OLR: n = 94, 83.2%; P = .400). Before matching, one significant difference between both groups was found for the resection extend (P < .001). Major hepatectomies were performed in 14.8% (n = 8) of the cases in the LLR group and in 52.2% (n = 59) of the cases in the OLR group.
After PSM, no significant differences of baseline characteristics between both groups were observed. Baseline characteristics of patients in both groups are given in Table 1.
Patients Baseline Characteristics Before and After Propensity Score Matching
ASA, American Society of Anesthesiologists; BMI, body mass index; LLR, laparoscopic liver resection; OLR, open liver resection.
Surgical difficulty
Before PSM the surgical difficulty score in the LLR group was significantly lower compared with the OLR group (LLR: 1 [0–5]; OLR: 3 [0–6]; P < .001). After PSM we observed no significant differences between the groups (LLR: 2 [0–5]; OLR: 1 [1–3], P = .293, Table 2).
Difficulty Score of Liver Resection
BMI, body mass index; LLR, laparoscopic liver resection; OLR, open liver resection; S, segment.
Perioperative outcomes after PSM
The median operation time was 215 minutes (45–501 minutes) for the LLR group and 183 minutes (114–361 minutes) for the OLR group (P = .059). No differences were seen regarding intraoperative BL between the LLR (median = 643 mL, range = 0–2255 mL) and OLR (median = 718 mL, range = 0–1799 mL) approach (P = .9163). Patients undergoing liver resection by laparoscopic approach had a significantly shorter intensive care unit (ICU) stay (LLR: 1 [0–4] days; OLR: 1 [0–3] days; P = .009) and significantly shorter median hospital stay (length of stay [LOS]) (LLR: 7 [4–14] days; OLR: 10 [5–16] days; P < .001) than patients with the open approach (Table 3). The 30-day complication rate Clavien–Dindo ≥III was 11.4% (n = 4) in the LLR group and 2.9% (n = 1) in the OLR group (P = .375). Two patients suffered from bile leaks (LLR: n = 1, 2.9%; OLR: n = 1, 2.9%), 1 patient had a pneumothorax (LLR: n = 1, 2.9%), and 2 needed relaparoscopy because of trocar hernia with a subileus (LLR: n = 1, 2.9%) and wound-healing impairment (LLR: n = 1, 2.9%).
Perioperative Clinical After Propensity Score Matching
BL, blood loss; Hb, hemoglobin; ICU, intensive care unit; LLR, laparoscopic liver resection; LOS, length of stay; OLR, open liver resection.
The postoperative 90-day mortality rate was 0% in both groups.
Major hepatectomy
Of 167 patients, major hepatectomy was performed in 8 patients (14.8%) in the LLR group and in 59 patients (52.2%) in OLR group. The median age at operation for patients undergoing major-LLR was 25 years compared with 42 years in the major-OLR group (major-LLR: range = 13–48 years; major-OLR: range = 14–70 years; P = .004). There were no significant differences when comparing baseline characteristics, such as gender, BMI, and ASA score (Table 4). Patients in the major-LLR group had a significantly longer median operation time (major-LLR: 403 [240–501] minutes; major-OLR: 221.5 [111–529] minutes; P < .001) but no statistically significant differences regarding BL were shown between groups (P = .843); however, there was a significantly shorter overall median LOS of 2 days (major-LLR: 7 [5–14] days; major-OLR: 9 [7–129] days; P = .013). The median ICU stay was 1 day in both groups (major-LLR: 1 [1–4] days; major-OLR: 1 [0–15] days; P = .655). There was a trend toward a lower complication rate after major-LLR compared with major-OLR; however, because of the low number of patients in the LLR group this did not reach statistical significance (major-LLR: n = 0 (0%); major-OLR: n = 10 (16.9%); P = .207). Complications were biliary leak (n = 6, 10.2%), liver abscess (n = 2, 3.4%), acute renal failure (n = 1, 1.7%), and impairment of wound healing (n = 1, 1.7%). The 90-day mortality rate was 0% in both groups.
Comparison Between Baseline Characteristic and Perioperative Outcomes of Major-LLR and Major-OLR Groups
ASA, American Society of Anesthesiologists; BL, blood loss; BMI, body mass index; Hb, hemoglobin; ICU, intensive care unit; LLR, laparoscopic liver resection; LOS, length of stay; OLR, open liver resection.
Discussion
In this study, we report on our experiences in 167 patients undergoing surgery for benign liver tumors and lesions. Among all benign tumors and lesions, the most common indication for liver resection was HCA, followed by FNH and hemangioma. Although, HCA is considered rare, there is a strong association of malignant transformation and subtype-dependent notable risk of rupture. Therefore guidelines recommend resection in all HCAs found in men and HCAs persistently greater than 5 cm or increasing in size in women.24–26 In contrast, most other benign tumors and lesions in the liver do not warrant therapy or surgical intervention.27–29 Exemplary in hemangioma and FNH, being considered the most common solid benign liver tumors,30,31 therapeutic consequences are limited to symptomatic tumors,32,33 rupture, intratumoral bleedings, Kasabach–Merritt syndrome, and organ or vessels compression. 33
Several studies have reported the advantages of LLRs for malignant liver tumors regarding BL, time of hospitalization, and complication rate.34–36 All available studies focusing on laparoscopic approaches for benign liver tumors and lesions are limited by patient heterogeneity and less extended resections. 14 Indeed, this is the first study comparing LLR and OLR for benign liver tumors and lesions with PSM of >150 patients. Our analysis is of importance, as aspects of perioperative morbidity and mortality are of particular interest in patients with benign liver tumors and indication for resection is to a high degree dependent upon clinical presentation.
Because of the favorable outcomes, we have expanded our minimal invasive liver program over time. Almost 50% of this patient cohort was treated within the past 2 years. Depending on the difficulty of the resection and experience of the surgeon, we individually decided which method is feasible for the patient. By rigorously selecting the right approach, we were able to minimize the rate of conversions to 1.7%. As previously reported, we have seen no differences between the minimal invasive operation methods MILL, HALS, and SILS. 37 Thus, we consider these methods equally beneficial for patients.
The complication rate after resections of benign liver tumors is reported to be low independent of the operation method. In line with others, we have not seen a decreasing complication rate with the laparoscopic approach.17,18,38 After adopting the surgical difficulty score by Hasegawa et al. there was a trend toward higher surgical difficulty in the LLR group, leading to slightly higher morbidity rates. 23
As others already have reported, Hb-based calculation of intraoperative BL showed no differences between matched groups and major groups.39,40 However, a significantly shorter ICU and LOS was indeed observed. Despite longer operations times, our results suggest overall advantages of laparoscopic surgery for benign liver tumors and lesions. Given the positive results of this study and prudent patient selection, surgical indication should be given liberal.
Certainly, benign tumors and lesions pose an interesting challenge, as indications are based on either increase of size or symptoms, which are likely because of a larger tumor size. Focusing on whether patients with extensive tumors and lesions are particularly amenable to the laparoscopic approach, we also compared laparoscopic major hepatectomies with open major hepatectomies. To date, laparoscopic major hepatectomies are still critical because of the complexity of the procedure, the fear of venous gas embolism, and uncontrolled bleeding.8,41 Nevertheless, we observed no major complications in the LLR compared with a complication rate of 16.9% in OLR. In addition, the results of this study showed a significantly shorter LOS in the LLR group. The small number of patients that underwent a major liver resection in the LLR cohort is a limitation of this study and further investigations are needed to confirm these data. However, this finding indicates the feasibility of major liver resection for benign liver tumor in experienced centers. 42
Achieving favorable results after LLR for benign tumors in this study consequently highlights the benefits of this approach. The retrospective nature of this study is an obvious limitation. However, in the absence of large randomized controlled trial we believe this report to be a valuable contribution that allows clinicians to ascertain whether laparoscopy is feasible for patients with benign liver tumors or lesions. Based on our findings, we suggest preferring the LLR over OLR for benign liver tumors and lesions regardless of the resection extent.
Footnotes
Authors' Contributions
S.W.: conception and design, analysis and interpretation, and writing the article; A.K.: writing the article, statistical analysis, and data collection; P.K.H.: conception and design and critical revision of the article; C.B.: analysis and interpretation and critical revision of the article; F.K.: conception and design and critical revision of the article; A.A.: critical revision of the article; K.L.: statistical analysis; J.P.: critical revision of the article; M.S.: conception and design, analysis and interpretation, and critical revision of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.