
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) is the most commonly performed bariatric procedure in the world. LSG is a safe and effective primary bariatric procedure with durable weight loss. We believe LSG should not be called “easy” and should be performed only by surgeons trained in bariatric surgery.
Method:
We describe the technique, step by step, we use to perform a sleeve gastrectomy (SG).
Results:
The highlights of a safer SG systematization are based on minimum 36Fr bougie calibration, starting 4–5 cm from the pylorus, keeping ∼1 cm distance from esophagus. We routinely use staple line reinforcement by continuous suture.
Conclusions:
LSG is a safe and effective primary bariatric procedure with durable weight loss. It should be performed only by surgeons trained in bariatric surgery.
Introduction
Laparoscopic sleeve gastrectomy (LSG) is currently the most frequent primary bariatric procedure performed worldwide. 1 This is because, when compared with the laparoscopic adjustable gastric banding, a very popular procedure more than a decade before, the sleeve was a simple, yet a powerful metabolic operation, activating significant hormonal pathways that lead to changes in eating behavior, glycemic control, and gut functions; the procedure does not need a foreign implant. And when compared with Roux-en- Y gastric bypass, LSG is easier regarding its technical aspects and does not need any intestinal anastomosis. The LSG technique is limited to the stomach, avoiding the presence of internal hernias in the postoperative follow-up.1–3
Surgical Technique
The patient is placed in a split leg position with the surgeon located in between the patient's legs.
To enter the abdomen, we use Veress needle at the umbilicus and CO2 is insufflated up to 15 mmHg.4,5
We use five trocars for the LSG technique (Fig. 1). In patients with higher body mass index who have severe visceral obesity, additional trocars can be added for retraction of the omentum or big fatty livers, to optimize the exposure to reach the left crus.6–9
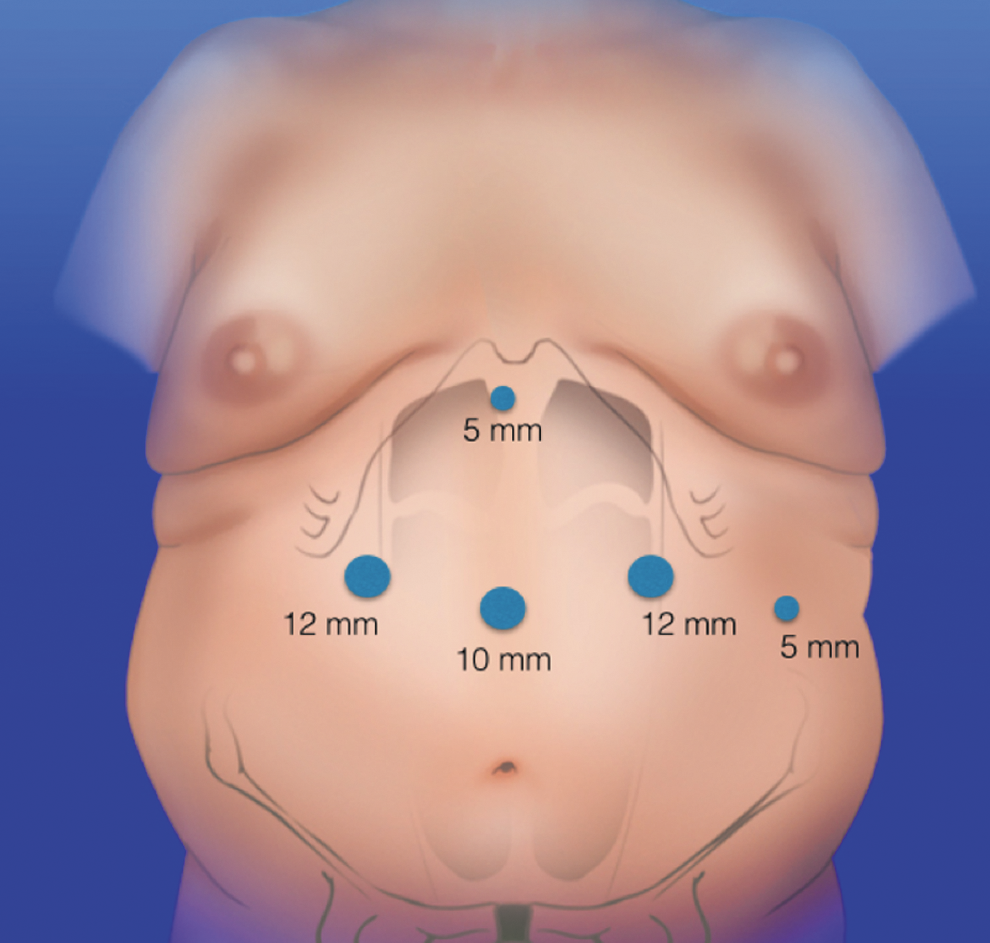
Trocar position when using five trocars.
Once the left crus is reached, an optimal exposure of the hiatus is mandatory to find incidental hiatal hernias and a complete dissection of the left crus is performed to prevent retained fundus9–13 (Fig. 2).
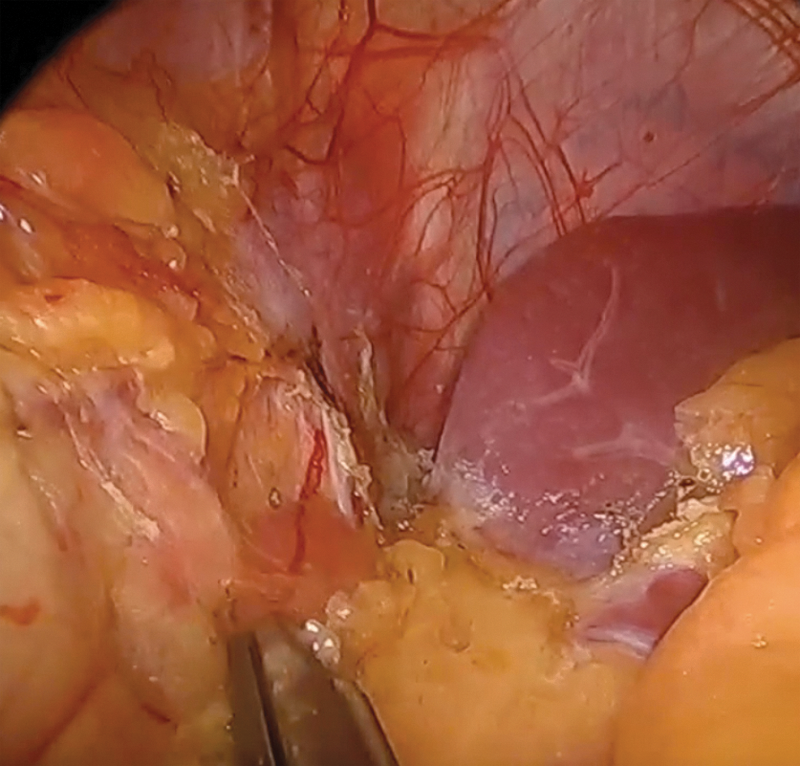
Exposure of the hiatus, this step is mandatory for optimal sleeve construction: inspect the hiatus for hernia and dissect the left crus.
The great omentum should be opened close to the stomach wall in some part in between the fundus and the antrum to have greater curvature completely detached from the stomach, preserving the gastroepiploic vessels; this dissection starts at 3–4 cm proximal to the pylorus and continues along the greater curvature to the left crus5,14–18 (Fig. 3A, B pylorus, white arrow).
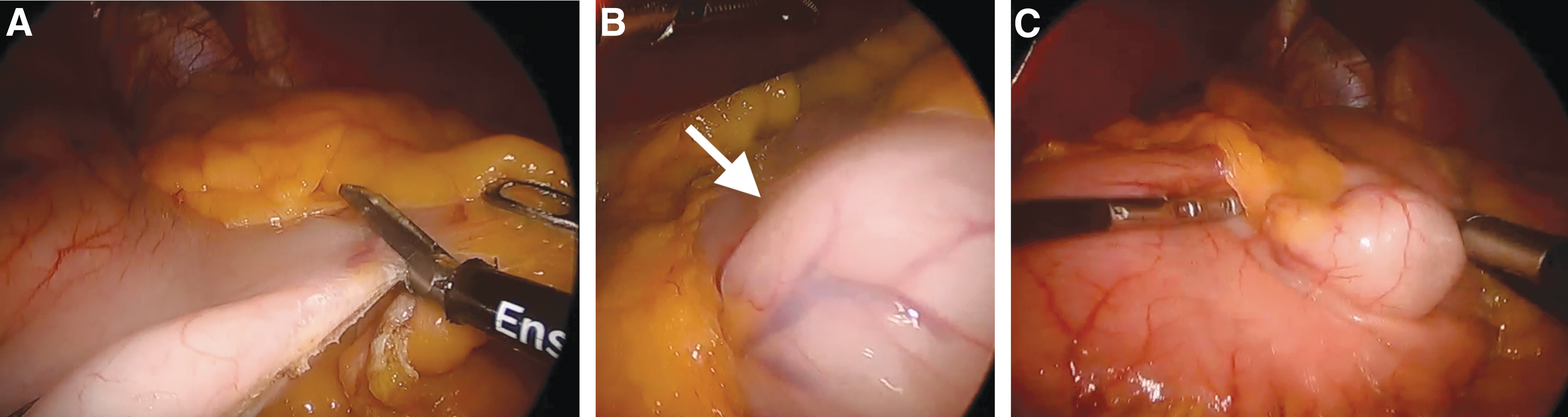
Posterior adhesions are carefully divided.6,19 When clearing the top of the fundus and the angle of His, it is recommended to be careful and slow down in this part of the operation, because short gastric vessels could be covered with a large amount of fat making them difficult to identify, 7,8,10–12 and a lesion can cause severe bleeding.9,13,20,21 The left gastrophrenic ligament should be divided to expose the angle of His to identify the complete hiatus and fundus, this is because an undiagnosed hiatal hernia or unresected fundus could be a cause of severe reflux and regurgitation postoperatively.7,8,21
A bougie is mandatory before starting resection of the stomach. Always before firing the stapler, it is important to ask the anesthesiologist to move the bougie to be sure that the tube is free. We use a 36Fr bougie.3,9,21 (Fig. 3C). The stapler should never be placed abutting the bougie, it should be used only for guidance of the resection of the stomach. Other surgeons use the endoscope as a bougie, we think an advantage could be the tracking of the resection from the inside, but some disadvantages are that they have to dessufflate the stomach before firing and also that the endoscopic tube's diameter is smaller.
The starting point from the pylorus to begin the gastrectomy is still controversial. Most surgeons begin the division of the antrum from 2 to 5 cm from the pylorus to avoid large antrums4,15 (Fig. 4A). We mostly fire the stapler 5 cm away from the pylorus.
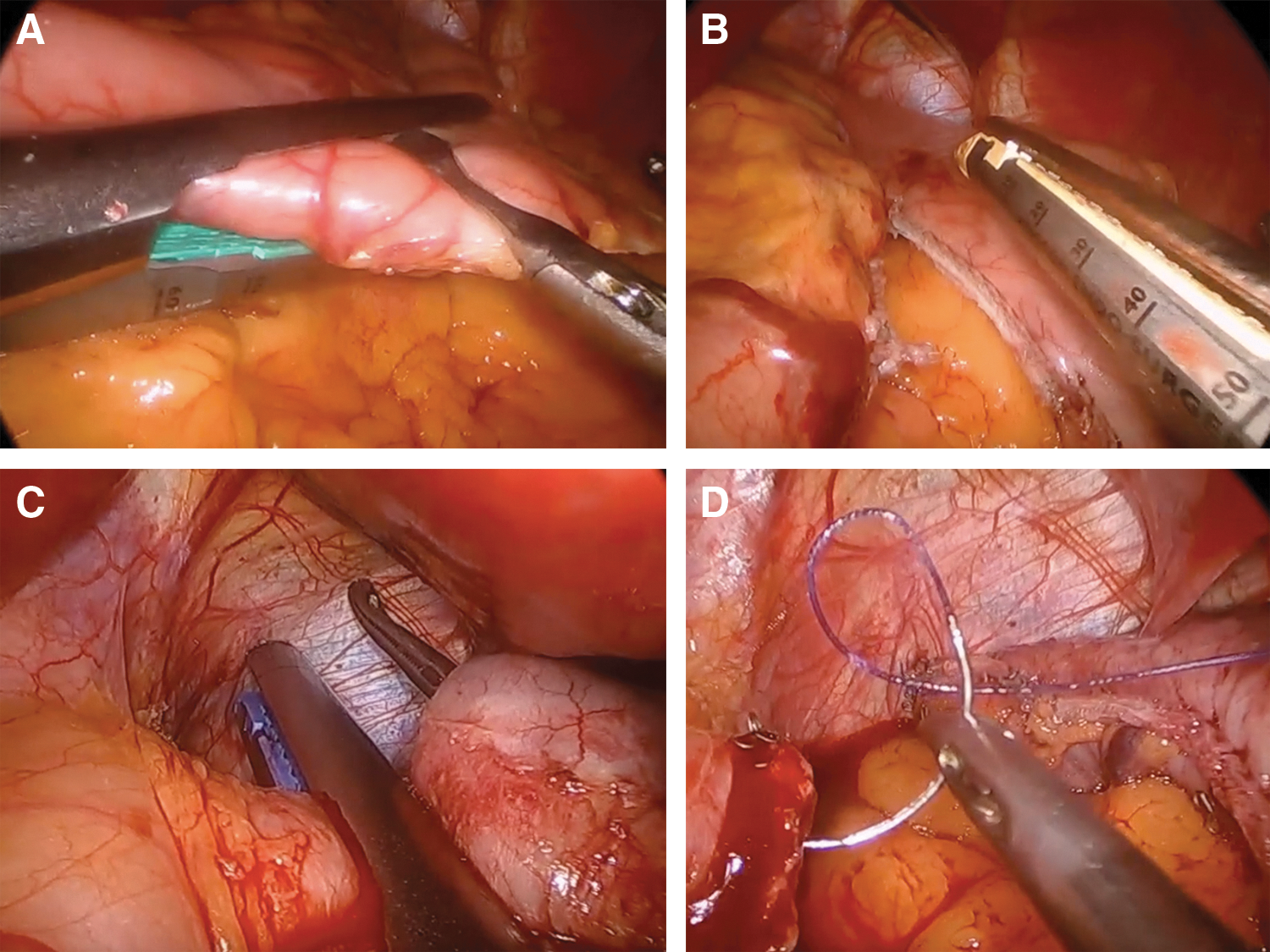
To perform gastrectomy, we chose the tallest stapler cartridges (green) at the antrum level and gradually chose shorter staplers as the resection continues proximally.5,16 The thickness of the stomach decreases from antrum to fundus and from greater curvature to the smaller curvature. Based on the use of Ethicon Echelon stapler, we should start with black or green cartridge and continue with a golden cartridge and finish with a blue cartridge. (Fig. 4B, C) But with Medtronic®, we should start with one or two black cartridges and finish with a purple cartridge. We should always check the posterior wall before firing. Once we have reached the proximal stomach, the stapler has to be positioned 1 cm lateral to the left of the angle of His to avoid inclusion of esophageal tissue.9,15,21
We always perform staple line reinforcement by using over-sewing with absorbable suture (Fig. 4D). Methylene blue test is performed routinely. 21
Conclusions
We can conclude that LSG is a safe and effective primary procedure with adequate weight loss. The concept of a “simple” operation, without the need of intestinal anastomosis, is what made this procedure popular and reproducible. Therefore, we believe that this procedure should not be called “easy operation” and it should be performed by surgeons trained in bariatric surgery and with a multidisciplinary group. The highlights of a safer LSG systematization are based on minimum 36Fr bougie calibration, starting 4–5 cm from the pylorus, keeping 1 cm distance from the esophagus, and reinforcing the staple line routinely.
Footnotes
Disclosure Statement
No competing financial interests exist.