
Abstract
Abstract
Background:
The circular stapled (CS) technique with transoral placement of the anvil is commonly used to perform the esophagogastric anastomosis during minimally invasive esophagectomy (MIE). The procedure is safe, efficient, and highly reproducible; however, the intersection between the circular plane of the stapler and the linear staple line of the esophageal stump can expose the anastomosis to the formation of dog-ears and, therefore, increase the risk of anastomotic leak (AL). We describe a simple modification of the CS technique that consists of folding the linear esophageal transection line with a stitch around the anvil shaft, to include the staple line in the resection during the EEA™ firing.
Methods:
We prospectively collected data on a small group of patients who underwent MIE for cancer using our modified CS technique. Feasibility has been evaluated as the percentage of cases in which the modified anastomosis technique has been carried out successfully with the formation of a complete anastomotic ring. Safety has been defined as the absence of procedure-related complications.
Results:
MIE was performed in 10 patients using our modified CS technique. All the procedures were successfully completed with complete resection of the linear esophageal staple line and no intraoperative complications. Only one patient developed a postoperative AL that was only detected by barium swallow and did not cause any symptom or clinical sign.
Conclusion:
Our modified CS technique is feasible and did successfully prevent the occurrence of clinically relevant ALs in this small case series of patients.
Introduction
The past three decades have witnessed an increase in the incidence of esophageal cancer worldwide. 1
Esophagectomy with adequate lymphadenectomy, with or without neoadjuvant chemoradiation, represents the treatment of choice for resectable cancer of the mid-lower esophagus and esophagogastric junction.2,3
Despite the improvements in surgical technique and postoperative care, esophagectomy is still a demanding and technically challenging surgical procedure. The overall incidence of postoperative complications ranges between 20% and 80%,4,5 and the in-hospital mortality reaches an incidence of 20%.4,6,7 Pulmonary complications and anastomotic leak (AL) are the two main sources of postoperative morbidity and mortality, with an incidence up to 67% and 40%, respectively.4,8,9
The first minimally invasive esophagectomy (MIE) was described by Cuschieri et al. in 1992. 10 Since then, several single-institution series11–13 and meta-analyses14–17 have been published, demonstrating the benefits of the minimally invasive approach compared with open esophagectomy, in particular a shorter hospital stay, less blood loss, better quality of life, and less pulmonary complications. These favorable results have been confirmed by three important studies: a multicenter randomized control trial (the TIME trial), 18 a prospective multicenter trial (the ECOG 2202 trial), 19 and a large single-institution case series of >1000 patients. 20
Despite these good results, the aforementioned studies failed to demonstrate a superiority of MIE in the incidence of postoperative AL. 21 The results of the TIME trial showed instead an increased incidence, although not statistically significant, of AL after MIE (12% vs. 7% in the OE group). 18
These findings shed new light on the old debate over which technique would be the preferred to create an intrathoracic esophagogastric anastomosis after esophagectomy. Several articles have been published describing the anastomotic techniques for the intrathoracic reconstruction during MIE 22 ; most of the procedures have been adapted from open surgery and can be summarized into three main categories: the hand-sewn (HS) technique, the circular stapled (CS) technique, and the side-to-side linear stapled (LS) technique. 23
Even if the CS and LS technique seems to be superior in terms of anastomotic leaks to the HS technique, there is great disparity in the published literature comparing the three techniques both in open and minimally invasive surgery, due to variations in technique, patients' condition, cancer stage, preoperative treatment, and so on. 23
These techniques, applied to MIE, are safe, efficient, and highly reproducible; however, we believe there are two main downsides that could potentially explain the increased risk of anastomotic leakage. First, the minimally invasive HS technique is demanding and handling the proximal esophagus during hand sewing may increase tissue damage. Second, in the CS technique, joining the esophageal stump linear staple line to the circular anastomotic plane of the circular stapler creates intersection of staple lines and dog-ears, potentially compromising tissue vascularization and favoring an anastomotic leakage.
This article describes an improvement to the CS technique, which we previously preferred during MIE, which addresses the problem of staple lines intersection. We also provide data on its feasibility and postoperative outcomes.
Materials and Methods
From March 2018 to October 31, 2018, all esophageal cancer patients, planned for totally minimal invasive esophagectomy at our institution, underwent MIE with our modified circular stapling anastomosis technique. The study protocol was approved by the Department of Surgical, Oncological and Gastroenterological Sciences Research Committee—University of Padova, Padova, Italy. All patients were informed about the technical modification and their written consent to the procedure was obtained.
All cases have been prospectively collected in our esophageal cancer database. Collected data comprise patients and tumor characteristics (age, gender, comorbidities, ASA score, Karnofsky score, tumor histology, tumor location, and clinical tumor staging), chemoradiation treatments, details of surgery (technical details, complete anastomosis ring, surgery duration, blood loss, intraoperative complications), and postoperative outcome (morbidity and mortality).
Technical feasibility has been evaluated as the percentage of cases in which the improved anastomosis technique has been carried out successfully with the formation of a complete anastomotic ring. Safety has been defined as the absence of procedure-related complications.
As this was a safety and feasibility study of a modified surgical technique, no sample size and comparison group analysis were applied. Categorical data are expressed as value and percentage; continuous data are reported as mean and standard deviation. Data were analyzed with RStudio version 1.1.463 (RStudio, Inc.), R version 3.5.2 (The R Foundation for Statistical Computing Platform).
Surgical technique
The laparoscopic and the thoracoscopic phase of the procedure are performed as described by Luketich and colleagues.24,25
Anastomosis technique
Once esophageal dissection is extended 3–4 cm above the Azygos vein, the stomach is retrieved in the thorax; here the conduit is divided from the surgical specimen with a 4.8 mm EndoGIA™ (Medtronic, Minneapolis, MN).
The proximal thoracic esophagus is transected with a linear stapler at the planned level of anastomosis, ∼2 cm above the Azygos vein, and the specimen is extracted in a retrieval bag through a 5 cm thoracotomy performed extending the 10 mm port at the level of the seventh intercostal space. The proximal margin is sent for frozen analysis; if negative the anastomosis is performed.
The OrVil™ EEA Anvil (Medtronic) is, therefore, passed transorally by the anesthesiologist. The OrVil is carefully pushed into the esophageal stump and the shaft is exteriorized through a small hole performed in the middle of the staple line (Fig. 1).
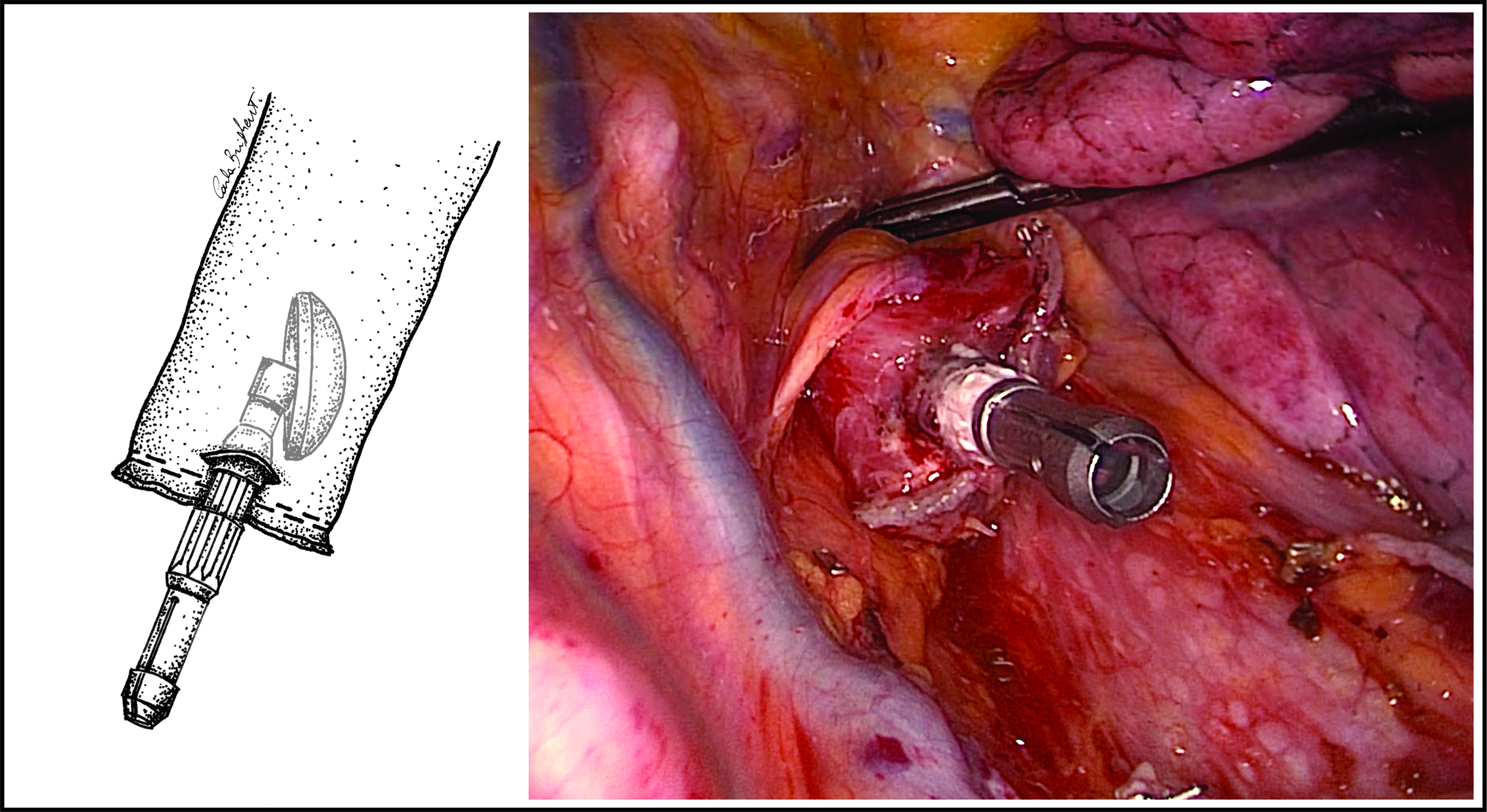
The esophagus is transected with a linear stapler ∼2 cm above the Azygos vein; the OrVil™ is passed through a small hole in the middle of the staple line. Illustration: Carla Brighenti.
To avoid the formation of dog-ears due to circular on linear stapling, we fold the linear esophageal transection line with a stitch around the anvil shaft, to entirely transect the linear staple line with EEA firing (Figs. 2 and 3). A 25 mm EEA is introduced through the small thoracotomy in the fundic portion of the gastric conduit across a small gastrostomy.
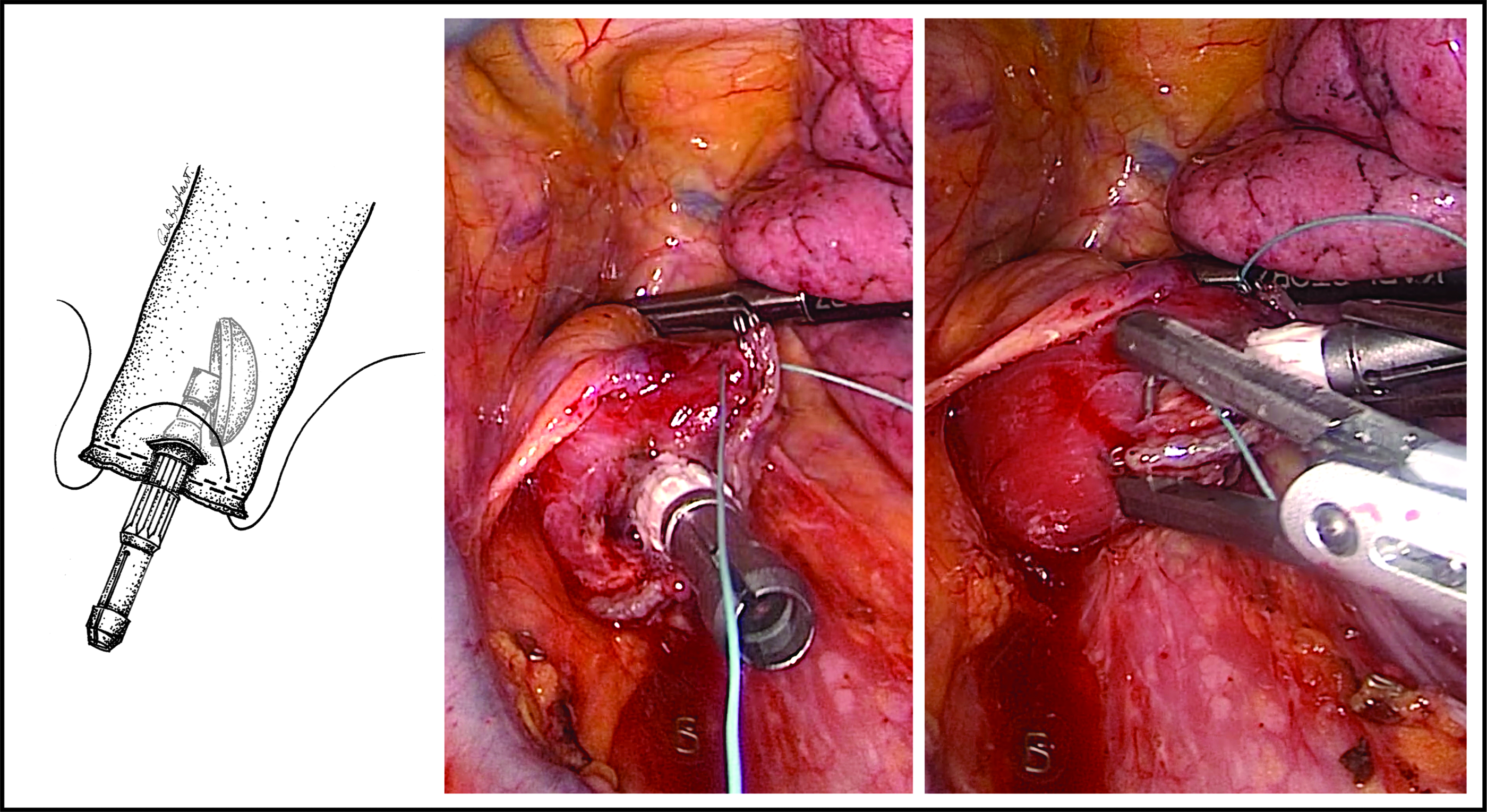
The staple line is wrapped around the anvil shaft with a single stitch. Illustration: Carla Brighenti.
Staple line wrapped around the anvil shaft with the formation of a little pleat. Illustration: Carla Brighenti.
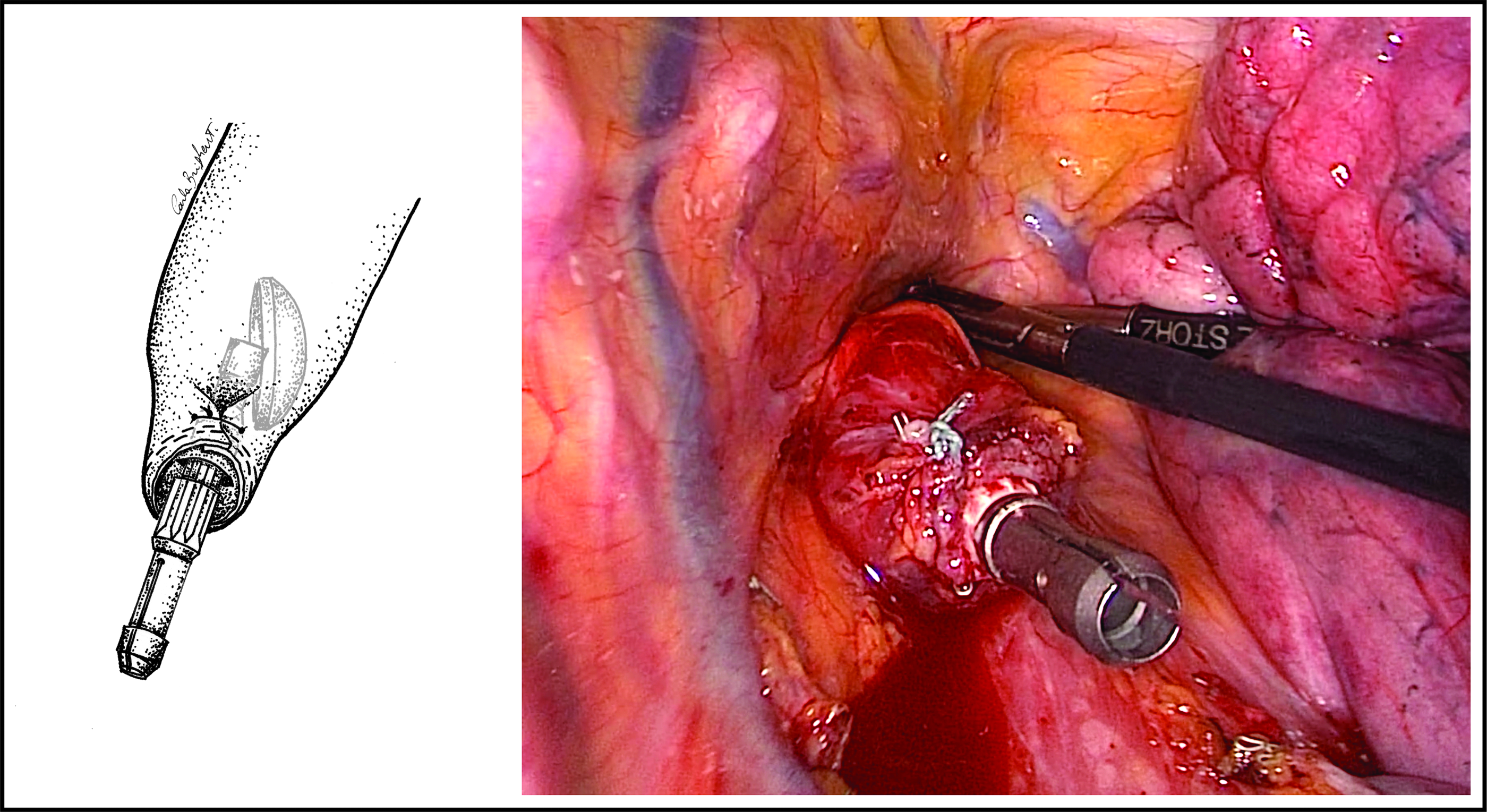
The EEA spike is advanced through the posterior wall of the conduit, the gastric fundi is then gently retracted to ensure the spike complete exteriorization. Care is taken to ensure that the conduit is in the correct position without any twisting. By inserting the spike in the anvil, the latter reaches the firing position smoothing out the pleat created by the stitch on the esophageal stump, allowing an end-to-side anastomosis without dog-ears that are wrapped around the shaft and excised with the anastomotic rings (Figs. 4 and 5).

The stapler and the anvil are engaged. The anvil head tilts, smoothing the esophageal pleat created by the stitch. Illustration: Carla Brighenti.
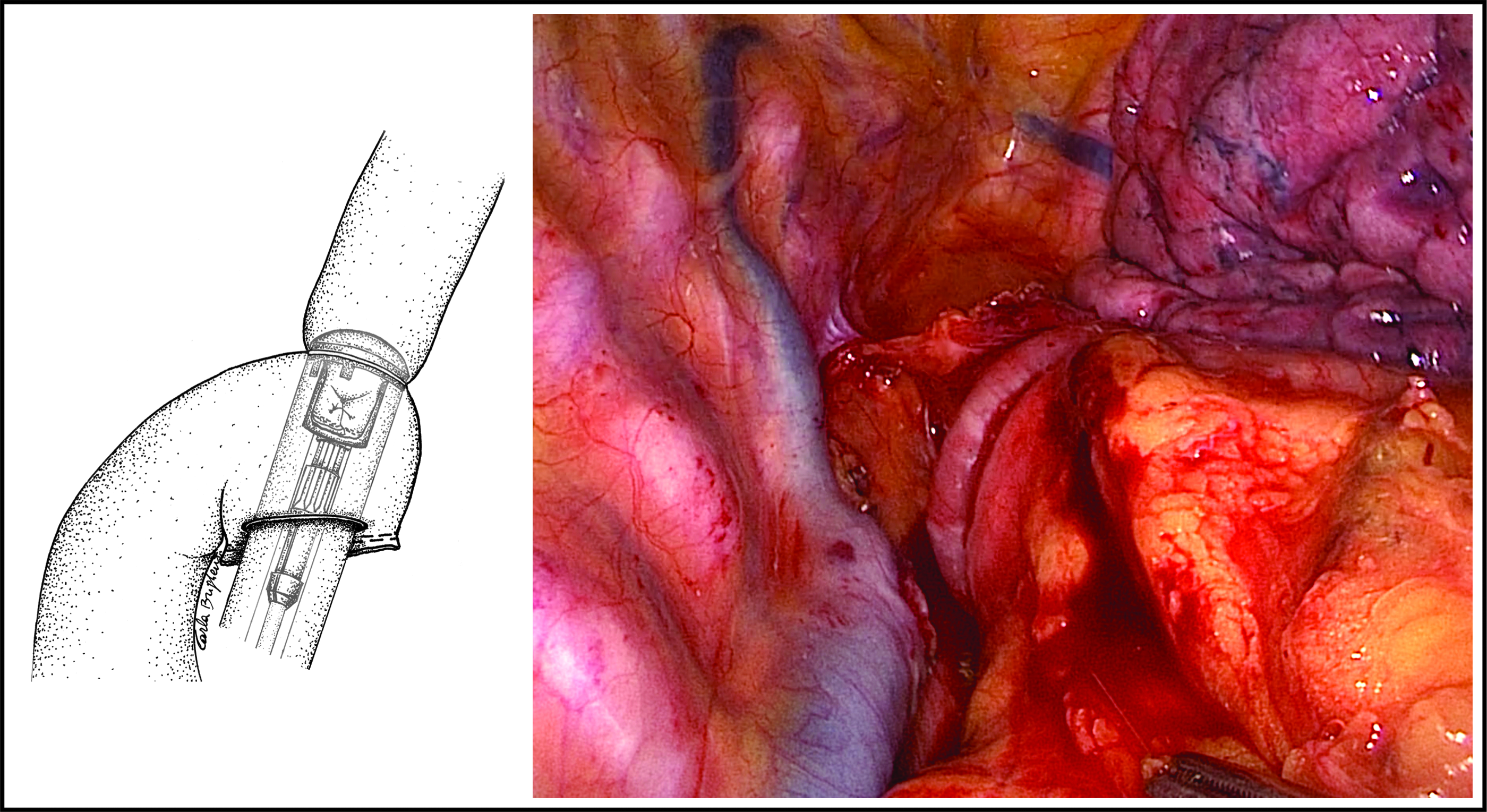
The anastomosis is performed with no dog-ears. Illustration: Carla Brighenti.
The gastrotomy is excised by a single fire of EndoGIA and a nasogastric tube is placed through the anastomosis under direct vision. Finally, the anastomosis is suspended by suturing the upper-medial portion of the conduit to the mediastinal pleura with interrupted absorbable stitches. The upper portion of the gastric conduit's omentum is used to wrap the anastomosis.
Results
We performed our modified anastomosis during MIE in 10 consecutive patients (mean age 60.4 ± 11.5 years). Mean total operative time was 342 minutes (St. Dev. 55.2). The modified CS anastomoses were all successfully performed without intersecting staple lines and with 100% complete anastomotic ring formation (100% feasibility). All patients underwent postoperative oral contrast swallow, and one (10%) minimal anastomosis leakage was registered (Type 1 according to ECCG—Esophagectomy Complications Consensus Group 26 ). Oral feeding was re-established in all patients.
No complications due to the technique have been registered. See Table 1 for further results.
Results of the Study Series
TNM tumor staging according to AJCC seventh edition.
Leakage and conduit necrosis classified according to ECCG. 26
ADC, adenocarcinoma; CTRT, chemoradiotherapy; Distal thor., distal thoracic esophagus; ECCG, Esophagectomy Complications Consensus Group; Middle thor., Middle thoracic esophagus; No compl., no complications; SCC, squamous cell carcinoma.
Discussion
This article describes a simple modification of the CS technique for esophagogastric intrathoracic anastomosis during MIE.
Despite the simplicity of the technical modification, our technique proved to be feasible and easy to perform: no significant increase in the operatory time and in intraoperative complications was noted in this preliminary case series compared with patients undergoing MIE with the conventional CS anastomosis at our center.
Since the introduction of MIE in 1992, 10 the main case series, randomized control trials, and meta-analyses18–21 failed to demonstrate a superiority of the minimally invasive approach in preventing AL. Although we recognize that there are several limitations in evaluating this complication given the variability in tumor location, tumor stage, anastomotic location, and anastomotic technique, this finding prompted us to examine the potential flaws of the CS anastomotic technique used at our center during MIE.
Since the introduction of circular staplers in the 1970s, 27 the CS technique has been increasingly used during open esophagectomies. 28 The main advantages of the CS anastomosis include a shorter operative time and the requirement of less surgical expertise compared with the HS technique, with no increase in the risk of anastomotic leakage.29–31 Since the beginning of our experience in 1987, we have adopted circular stapling as the standard technique to perform the esophagogastric anastomosis during Ivor Lewis procedures.
The CS technique was adapted to the minimally invasive approach by placing the anvil of the circular stapler in the proximal esophagus through a transthoracic or a transoral route. 22 Nguyen et al. 32 first described the transoral technique to perform an intrathoracic CS anastomosis after MIE. The procedure involved the transection of the esophagus by linear stapling and the use of a commercially available tilted anvil, with the anvil's shaft attached to an orogastric tube passed transorally. Campos et al. 33 reported the good results of this technique on a small case series of 37 patients, with only one anastomotic leak (2.7%).
The transoral CS technique is highly reproducible and effective in reducing operative times. Moreover, compared with the transthoracic placement of the anvil, it avoids performing a purse string suture, thus significantly reducing the technical demand of the procedure and reducing the traumatic handling of the proximal esophagus. 22
In our opinion, the main downside of the transoral CS anastomosis lies on the intersection between the horizontal staple line of the proximal esophageal stump and the circular plane of EEA stapler, making the anastomosis prone to the formation of lateral intersecting staple lines (dog-ears). Although this issue is poorly addressed in esophageal surgery, several studies conducted in colorectal surgery demonstrated both in the experimental animal model34,35 and in the clinical setting 36 that dog-ears represent weak points in the anastomosis and that the lateral intersection of staple lines is associated with anastomotic leakage.
The modification introduced in our technique consists of placing a stitch that includes both the extremities of the esophageal staple line. When the stitch is closed the staple line is folded around the anvil's shaft: this conformation allows the staple line to be included in the resected specimen when the circular stapler is fired, thus avoiding the formation of staple line intersections.
We were able to implement this technique successfully in 10 patients without the formation of dog-ears and only one asymptomatic anastomotic leakage was registered. Moreover, the procedure resulted to be easily reproducible and easy to perform, as it required the application of a single stitch instead of a purse string suture.
This technique has limitations. First, the exteriorization of the anvil shaft through the horizontal staple line could require some manipulation of the esophageal stump, potentially leading to tissue tearing, damage that can occur easier with the purse string. Second, even though poor consensus exists in the literature, several studies report a higher risk of stricture formation with the CS anastomosis.29,37
The LS anastomosis could represent a valid alternative to avoid the intersection of staple lines during MIE. Collard et al. and Orringer et al. first proposed the use of a linear staple to create the posterior portion of the cervical esophagogastric anastomosis during transhiatal esophagectomy.38,39 Subsequently, Ben-David et al. and Gorenstein et al. reported the use of the technique in the thoracoscopic phase of MIE.40,41 The LS technique provides a larger anastomotic orifice diameter compared with the CS technique and it is less dependent on the size of the esophageal lumen: this corresponds to a significantly lower incidence of stricture compared with both the HS and the CS techniques. 37
In our experience, however, the development of clinically significant strictures is usually related to the occurrence of anastomotic leakage, rather than the site of the anastomosis or the anastomotic technique. Most of the strictures are successfully treated by a single or two sessions of endoscopic dilation. Moreover, the LS technique has several main downsides that limit its use in MIE: it requires a longer esophageal remnant to guarantee an adequate extension of the staple line on the esophageal side; it is more technically demanding compared with the CS technique: more space is required to properly maneuver the linear staple, especially in the high intrathoracic area and, lastly, the manual application of running or interrupted sutures is required to close the entry site of the linear stapler.
The main limitation of this report is the small number of patients. Moreover, the mean follow-up is relatively short since most of the minimally invasive procedures were performed in the past 2 years; therefore, we have limited data on long-term complications. However, we believe that this case series proves the feasibility and the safety of our technique.
Anastomotic leak is the Achilles heel of esophageal cancer surgery. It occurs even with optimally perfused conduits in low-risk patients, because surgical technique plays a critical role. In this context every effort should be taken to address all the possible weak spots of the anastomotic techniques. The ideal anastomosis should be easy to perform, reproducible, and should prevent the occurrence of leaks and stenosis. Although we might be far from achieving these goals, in this small case series our simple modification to the CS anastomosis for MIE proved to be safe, feasible, and efficient in preventing AL. Further randomized studies with bigger patients' samples will be required to assess its efficacy in reducing the incidence of anastomosis leakage.
Footnotes
Acknowledgment
The authors thank Carla Brighenti, AA, for the original drawings.
Disclosure Statement
No competing financial interests exist.
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship.
Funding Information
No funding to declare.