
Abstract
Background and Aims:
Laparoscopic sleeve gastrectomy (LSG) among older obese subjects (>60 years of age) has recently gained popularity because of the population aging. We performed a meta-analysis to clarify whether elderly patients undergoing this procedure have an increased complications risk.
Methods:
A literature search aiming at outcomes of LSG in elderly patients throughout Cochrane Library, Embase, Google Scholar, Medline, and Scopus databases was performed from inception until June 2019. Primary endpoints consisted of mortality and overall complications. Secondary endpoints comprised excess weight loss percentage (%EWL), remission, or postoperative improvement of several comorbidities (type-2 diabetes [T2DM], hypertension, dyslipidemia, and obstructive sleep apnea [OSA]). Heterogeneity between the studies was assessed by I2 test and random effects model for the comparative analysis. Mean difference (MD) and relative risk (RR) were used to report the results.
Results:
Eleven studies involving 2259 patients were scrutinized for this study. Overall complications rates did not significantly differ among younger and elderly patients undergoing LSG (RR: 1.71; 95% CI [confidence interval]: 0.76–3.83; P = .19). %EWL was superior among younger patients (MD: −7.63; 95% CI: −13.19 − 2.08; P = .007) while there were no significant differences in remission of T2DM, hypertension, and hyperlipidemia between the age groups (RR: 1.04; 95% CI: 0.83–1.31; P = .72; RR: 1.00; 95% CI: 0.84–1.18; P = .96; RR: 1.05; 95% CI: 0.79–1.38; P = .76). Younger patients exhibited a significantly higher OSA remission/improvement rate (RR: 0.81; 95% CI: 0.69–0.95; P = .001).
Conclusion:
LSG is a reliable bariatric method that is also safe in elderly patients with similar overall morbidity and similar obesity-related comorbidity resolution rates than younger ones, although weight loss outcomes were inferior.
Introduction
As life expectancy has increased leading to global aging, the incidence of obesity continues to rise especially in older adults.1,2 Bariatric surgery has been shown to be the best treatment to achieve and maintain weight loss and to reduce all-cause mortality risk and comorbidities related to obesity. 3
Many studies have compared weight loss outcomes after different bariatric surgery techniques or variations in the same procedure showing controversial results in older patients.4–7
There is still some controversy concerning the safety of this method for older obese subjects. 8 It appears that elderly patients have less tendency to lose weight, to improve obesity-related comorbidities, and they might have a higher risk of mortality after any bariatric surgery.9–13 On the other hand, elderly patients can still benefit from these weight losing procedures because there can be an improvement or even remission of comorbidities.8,11 Laparoscopic sleeve gastrectomy (LSG) appears to have slightly lower mortality and complication rate than laparoscopic Roux-en-Y gastric bypass (LRYGB), 4 with comparable outcomes, effectiveness, and safety in those patients. 13 However, there are few comparative studies on this topic, particularly concerning LSG for the obese elderly subjects with different ages.
The aim of this review and pooled analysis is to assess the current state of LSG for elderly patients in a comparative way, hypothesizing that mortality, overall complications, and outcomes may be similar to younger bariatric patients.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement to carry out this meta-analysis. 14 Any study about sleeve gastrectomy (SG) in elderly patients (older than 60 years) was searched from inception until June 20, 2019 consulting multiple literature databases (Cochrane Library, Embase, Google Scholar, Pubmed, and Scopus). 15 The following terms were applied for this literature research: advanced age; bariatric surgery; elderly; metabolic surgery; morbid obesity; old, sleeve gastrectomy. PICOS inclusion criteria (patients, intervention, comparator, outcomes and study design—Table 1) were used for scrutinizing the articles.
PICOS Criteria for Inclusion and Exclusion of Studies
%EWL, excess weight loss percentage; OSA, obstructive sleep apnea; PICOS, patients, intervention, comparator, outcomes and study design; SG, sleeve gastrectomy.
The indications for SG included patient age over 18 years at the time of surgery, body mass index (BMI) over 40.0 kg/m2 or between 35.0–40.0 kg/m2 including at least one comorbidity associated with obesity (arthrosis, dyslipidemia, gastroesophageal reflux disease, hypertension, obstructive sleep apnea syndrome [OSA], and type-2 diabetes mellitus [T2DM]).
Additionally, the reference lists of the included articles were also checked out aiming to find further relevant study on this topic, which might be included. We considered only comparative studies, therefore studies involving other techniques, or including different bariatric procedures at the same time, and one-arm studies were excluded.
We choose cutoff age as 60 years because this is considered the standard numerical criterion for the elderly population by United Nations. 15 However, earlier studies have used an age of over 55 years to define older subjects,8,10 while the World Health Organization define elderly patients as over 65 years of age. 15
Finally, the extracted data from the included articles were entered using predesigned tables. We used some estimations formulas, which have been validated by previous studies, to deal with missing information because we did not attempt to contact the included studies' authors to obtain the missing data. 16
Mortality and 30-days morbidity from surgery were the primary outcome measures. Secondary outcome included %EWL outcomes at 1-year follow-up, length of hospital stay; resolution or improvement of T2DM, hypertension, dyslipidemia, and OSA with all parameters compared with younger patients (<60 years) at follow-up.
The two authors (S.G., P.S.) searched, evaluated the quality of the studies and extracted the data independently. For these purposes the Newcastle-Ottawa Scale was used 17 and any disagreement was dealt by discussion.
Review Manager™ software was utilized to carry out the statistical analysis (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2019, version 5.3). The results were summarized as relative risk (RR) with 95% of confidence interval (CI) for the differences in dichotomous variables, while mean difference (MD) with a 95% CI was used to quantify the differences for continuous variables.
The heterogeneity was controlled with the Higgins I2, where a value over 50% indicated a significant heterogeneity among the studies. 18 However, heterogeneity was already expected to be high because the included studies were observational, a random effect model (DerSimonian–Laird) was used 19 and inverse variance for continuous variables and the method of Mantel–Haenszel in case of dichotomous outcomes. Statistical significance was considered for a P-value <.05 and we evaluated any publication bias inspecting the asymmetry of funnel plot.
Results
A total of 2017 articles were identified though the initial search of the mentioned database and 11 studies20–30 met our inclusion criteria and were selected for data extraction (Table 2). The Figure 1 shows the flow diagram of the search strategy. This pooled analysis included a total of 2259 obese subjects. There was no mortality during postoperative period of 30 days. The overall complication rate was similar between the two groups (RR: 1.71; 95% CI: 0.76–3.83; P = .19, Fig. 2). However, %EWL was significantly higher for patients younger than 60 years (MD: −7.63; 95% CI: −13.19 − 2.08; P = .007, Fig. 3).

Flowchart summarizing literature search results.
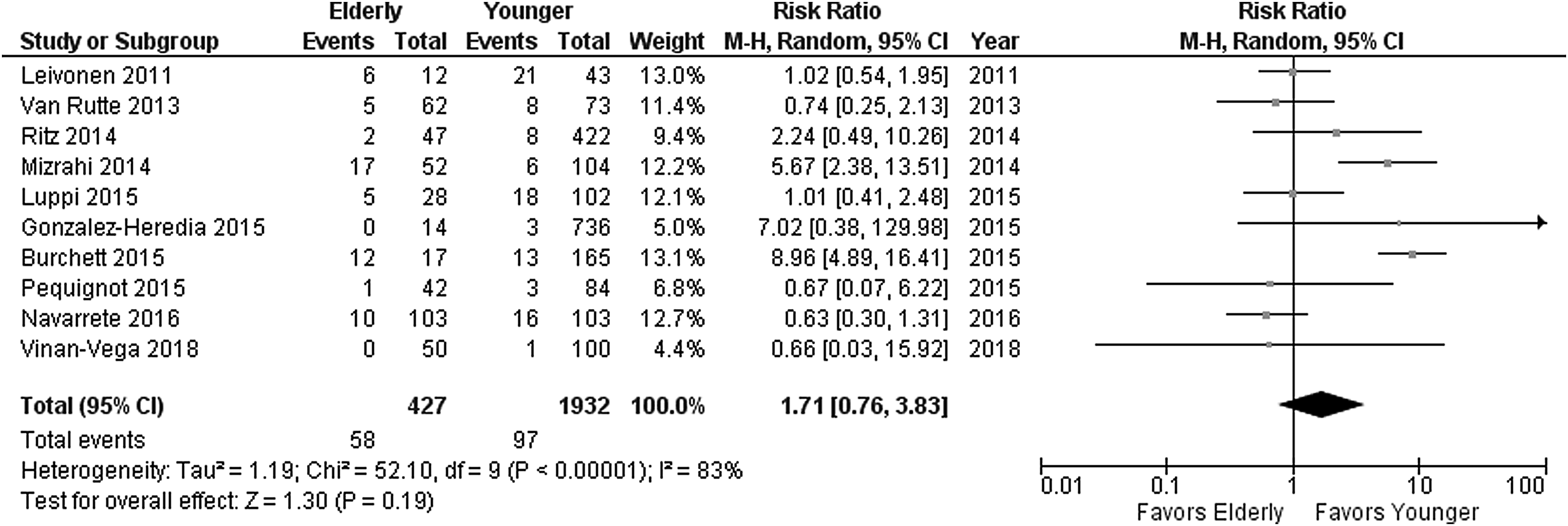
Forest plot showing a lower nonsignificant complication rate in patients younger than 60.

Forest plot showing significant difference in excess weight loss percentage at follow-up favoring patients younger than 60.
Characteristics of the Elderly Group Included in the Studies
%EWL, excess weight loss percentage; BMI, body mass index; nr, not reported; OSA, obstructive sleep apnea.
Remission or improvement of T2DM, hypertension, and dyslipidemia were also similar in the two study groups of age (RR: 1.04; 95% CI: 0.83–1.31; P = .72; RR: 1.00; 95% CI: 0.84–1.18; P = .96, and RR: 1.05; 95% CI: 0.79–1.38; P = .76 respectively). Significant difference was detected among OSA remission/improvement percentages (RR: 0.81; 95% CI: 0.69–0.95; P = .001). Lastly, the sensitivity analysis that we performed did not change the summary outcomes with the exclusion from the analysis of any of the included studies and we did not note a significant asymmetry of the funnel plot.
Discussion
The results of our pooled analysis of comparative studies showed that LSG provides a low overall complications rate independently than the age group (Fig. 2). However, these findings revealed that weight loss outcomes and OSA remissions were significantly better among younger patients (Figs. 3, 4).
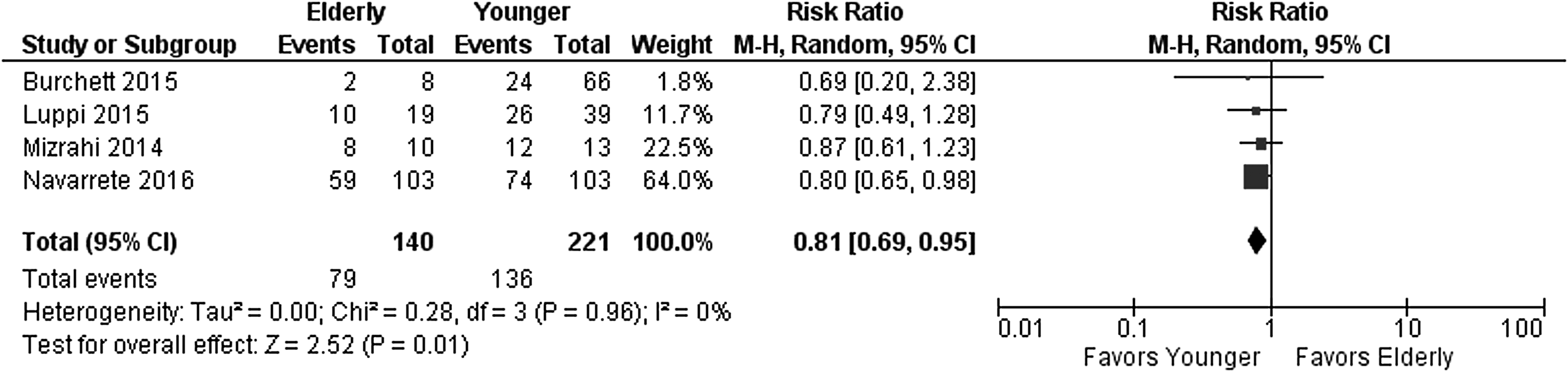
Forest plot showing significant difference in obstructive sleep apnea remissions at follow-up.
On the light of these results, LSG can be considered a safe procedure for elderly patients (over 60 years) contrary to laparoscopic gastric bypass that has been shown to be a procedure with higher complication rate and resulting in less optimal outcomes in elderly population from our previous meta-analysis on this topic. 12
During the last decade, bariatric surgery has been performed more regularly with better outcomes, in both perioperative morbidity and mortality.5,7
Considering that life expectancy has increased, as expected also obesity prevalence has increased in elderly subjects, regardless of gender and ethnicity, therefore, there will be a continuous increment of request for bariatric surgery among elderly patients.1–3
There has been a pooled analysis on the topic of LSG in elderly 13 that has revealed similar results including also patients between 55 and 60 years.
There appear to be a correlation between the risk of mortality and increasing age and BMI. In particular, BMI and age have shown to be important risk factors for 30-day mortality after LRYGB.31–33 This fact is consistent with our previous studies,8,10 where we have demonstrated that bariatric surgery can accomplish a satisfactory weight loss also for older subjects without too much higher risks, independently of which kind of bariatric surgery was used. In contrast, when directly compared available data on LRYGB for older versus younger obese patients, there might be a significantly higher morbidity for the first ones. 12 We attempted to clarify through this meta-analysis whether LSG is a safer bariatric surgery procedure in obese individuals over 60 years, using a direct comparative methodology. We detected an acceptable amount of %EWL, remission or improvement of several obesity-related comorbidities, with comparable rates of complications, consistently with the other previous studies.13,20–30 Although a greater %EWL during the follow-up was detected in younger patients after LSG, the difference in comorbidity resolution was significant only for OSA.
Elderly patients may present obesity-associated comorbidities longer than the younger and this fact may play a role in the remission outcomes in bariatric surgery and specifically in LSG. In addition to the comorbidities, with aging there is a reduction in the metabolic capacity. 34 This fact might be a result of the aging process, which affects their baseline physical condition, the presence of decreased muscle metabolic activity, and a higher prevalence of sarcopenia that can be aggravated by the loss of lean body mass after bariatric surgery (described in patients undergoing any bariatric surgery and ranging from 10% to 25%), all of which have been negatively correlated with weight loss. 35
There might be some hormonal changes due to aging affecting metabolism. Obese postmenopausal women have shown a reduced lipolytic activity when subjected to a hypocaloric diet.35,36 These subjects also showed an impaired capacity to mobilize lipids from fat storages to use energy, leading to a larger caloric intake after the surgical procedure. These facts have been showed determining the weight loss amount in female subjects between 20 and 45 years versus 55 to 65 years of age after bariatric surgery, where younger women exhibited a significantly higher amount of weight loss, but there results were not found in male patients, indicating the role not only of aging but also of some hormonal effect. 33 Conversely, in our pooled analysis, the majority of the included studies' patients were female, and this can explain our results consistently with the literature (Table 2).
It is well known that there is a decline of body basal calories expenditure starting from the age of 40, probably due to hormonal changes and a decrease in physical activity. For these reasons, one possible reason for the reduced weight loss outcomes in older subjects can be a less active life style in elderly population. Younger patients are usually more active physically, with improved exercise tolerance, which are important factors for successful long-term weight maintenance. 37
Patient's age negatively impacts the healing of all body tissues. 38 Macroscopically, aging affects the skin with atrophy, higher susceptibility to the external environment, diminished homeostatic capability, and loss of tension. 39 Furthermore, cell proliferation and migration are reduced, while also the levels of growth factors are decreased. 39 All these factors added to the comorbidities present in the elderly patient and affect the complication rates particularly after major surgeries.
We believe that elderly patients can be good candidates for LSG, as the morbidity rate did not differ from the younger patients on the contrary to similar comparison in patients undergoing LRYGB and even considering the prevalence of comorbidities, by which older subjects are often affected. We believe that the age alone cannot be used to exclude obese patients from bariatric surgery. However, a careful preoperative counseling should be performed to identify the proper indications for each bariatric surgery procedure considering that elderly patients may have higher procedural risks and inferior outcomes in weight loss and resolution/improvement of the preoperative comorbidities. Further active research is needed to tailor the optimal bariatric procedure in the older patient population.
The findings of our systematic review and meta-analysis are limited by several potential sources of bias that may have influenced the outcomes. This pooled analysis is limited to the LSG and it seems to be safe also in the elderly population providing sustainable good outcomes also at long-term follow-up. 7 We pooled outcomes of 11 studies, all retrospective, with differences in patients' population, study design, methods, and settings (Table 2). Some factors might affect the pooled outcomes although the same type of procedure was performed, with possible differences in the surgical technique and perioperative patient management: differences in the mean age of the patients for both elderly and younger groups, the gender prevalence percentage, and the overall number of subjects was relatively small. We have found that there were differences in age in patients considered as older adults, which varied from 60 to 70 years. We decided to exclude two studies included in a previous meta-analysis,40,41 because their age cutoff between groups was less than 60 years (55 years). Indeed, in most of the studies included, the subjects enrolled were mainly women, there was an imbalance in comorbidities in the control groups, and nutritional status reports were poor, all of which make it more challenging to achieve a favorable balance between benefit and risk for LSG in elderly patients. Moreover, it is not mentioned for how long any comorbidity was diagnosed because this can negatively affect the chance of resolution. Similarly, frequency and duration of follow-up was not always elucidated. Therefore, we pooled together all weight outcomes and complications. There is a need of original studies comparing different bariatric procedures for the older obese population patients with long-term outcomes to further improve the procedure choice process and we can confirm that LSG is feasible and safe procedure for obese subjects of over 60 years of age.
Conclusions
This meta-analysis of comparative studies demonstrates LSG to be a reliable bariatric procedure in older obese subjects with no difference in overall morbidity rate compared to patients under 60 years. LSG was also associated with similar obesity-related comorbidity resolution rates regarding T2DM, hypertension, and dyslipidemia in patients over and under 60 years, but LSG associated OSA resolution rates were superior for subjects less than 60 years. The associated %EWL was inferior in patients over 60 years of age undergoing LSG compared to patients under 60 years. In general, elderly patients assessed for bariatric surgery require multidisciplinary individual risk-based assessment regardless of the planned type of bariatric procedure. Further studies are needed to verify these outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.