
Abstract
Background:
Appropriate surgical techniques to control hemorrhage and retain residual liver function are key to treatment success for hepatocellular carcinoma (HCC). This study aimed to evaluate the clinical application of Glissonean pedicle transection with hepatic vein exclusion (HVE).
Materials and Methods:
Between April 2013 and December 2015, 50 patients underwent surgical resection for HCC and were randomly allocated to receive Glissonean pedicle transection with HVE (Glisson group, n = 25) or Pringle maneuver with intermittent clamping (Pringle group, n = 25). Intraoperative blood loss, blood transfusion, operation time, positive surgical margins, complications (bile leakage, hemorrhage, and ascites), and hospital stay were compared between groups, along with the alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (TB) levels at baseline and postoperative days 1, 3, and 7.
Results:
The operation time and range of hepatic resection were comparable between groups. Although both groups had similar preoperative ALT, AST, and TB levels, these levels on postoperative days 1, 3, and 7 were significantly lower in the Glisson group than in the Pringle group (all P < .01). Compared with the Pringle group, the Glisson group had a significantly lower intraoperative blood loss (P < .001), a lower blood transfusion rate (P = .017), lower incidence rates of postoperative hemorrhage (P = .030) and ascites (P = .024), a lower positive surgical margin rate (P = .017), and a shorter length of hospital stay (P < .001).
Conclusions:
Glissonean pedicle transection with HVE is a safe, simple, and effective procedure for hepatic resection.
Introduction
Hepatocellular carcinoma (HCC) is one of the most common malignancies and the second cause of mortality due to cancer in China. 1 The Barcelona clinic liver cancer (BCLC) staging system, which includes health performance status, tumor status, liver function, and treatment-related variables, is a widely accepted staging system for predicting the prognosis of primary liver cancer and has been incorporated into treatment guidelines in many countries. 2
Surgical resection remains the primary treatment of choice and delivers the best outcomes for patients with BCLC stage A HCC, who typically have a solitary lesion or up to three localized lesions <3 cm with preserved liver function. 3
The control of intraoperative and postoperative hemorrhage and retention of residual liver function are major technical concerns in the surgical treatment of patients with early stage HCC. As a classic surgical technique to control bleeding by hepatic pedicle clamping, the Pringle maneuver has received wide acceptance and has been applied in various hepatectomy procedures.4–6 However, vascular inflow occlusion during the standard Pringle maneuver may induce ischemia–reperfusion injury to the liver cells, thereby leading to postoperative liver failure. 7
In the 1990s, Takasaki first described the Glissonean pedicle transection for hepatic resection based on the concept of a new hepatic segmentation refined by the Glissonean pedicle tree anatomy. 8 This Glissonean pedicle approach is simple and has been proven to cause less loss of residual liver function, but backflow bleeding from the hepatic veins poses a possible risk of this approach. The aim of the present study was to present a surgical procedure combining the Glissonean pedicle transection with hepatic vein exclusion (HVE) for safe and effective control of hemorrhage during hepatic resection for HCC.
Materials and Methods
Patients
From April 2013 to December 2015, 50 patients with HCC treated in the First Affiliated Hospital of Jilin University were selected. The protocol was approved by the local ethics committee, and informed consent was obtained from all patients before being enrolled into the study. These patients with surgically resectable lesions were randomly assigned to undergo hepatic resection using the Glissonean pedicle transection combined with HVE (Glisson group, n = 25) or the Pringle maneuver with intermittent clamping (Pringle group, n = 25).
Surgical techniques
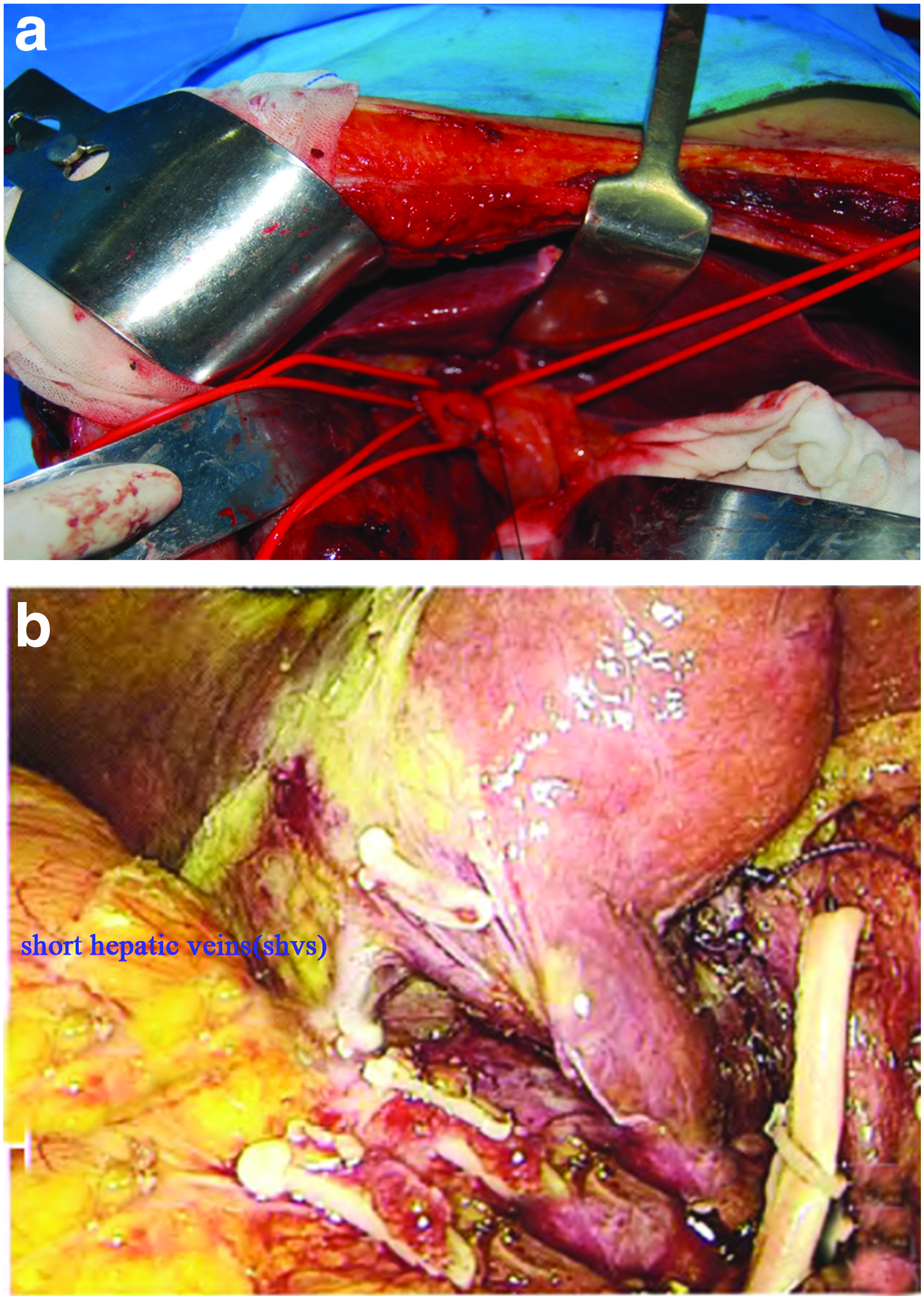
With the patient positioned in the supine position, an L-shaped incision into the abdominal wall was made on the right upper abdomen. In patients allocated to the Glisson group, after selective occlusion of hepatic blood inflow, hepatic resection was performed along the boundary lines of the ischemic regions on the hepatic surface (Fig. 1). In hemihepatectomy, sectionectomy, and segmentectomy, the corresponding left or right lobar, sectional, and segmental portal pedicle were isolated and ligated, respectively (Fig. 2a). During hepatic vein occlusion (Fig. 2b), the superior and inferior vena cava were freed, and with blunt dissection of the loose connective tissue covering the inferior vena cava, the common trunk of middle and left hepatic veins and the right hepatic vein was exposed. The blunt dissection continued toward the lower right to penetrate the ligament of the vena cava, and a precut of the ligament was performed when a ligament appeared to be too thick. The common truck of the middle and left hepatic veins was easily exposed and freed after rotation of the liver to the right side toward the caudate lobe. The hepatic veins were occluded with clamps if it was difficult to isolate the veins due to factors such as tumor invasion. Hepatic resection of the tumor-bearing liver segments was then carried out by the conventional clamp crushing technique, and during the procedure, hemorrhage was controlled with hemostatic electrocoagulation or suture ligation when appropriate. After hemostasis was achieved, a rubber drainage tube was placed. In patients allocated to the Pringle group, portal triad blood inflow was occluded by cross-clamping at the foramen of Winslow using a rubber tube. Fifteen-minute episodes of portal triad occlusion were repeated every 5 minutes when necessary until hepatic section was completed. For patients with severe cirrhosis, each occlusion was controlled to under 10 minutes. The average occlusion time was 10 ± 5 minutes in these patients. Hepatic resection was performed with the clamp crushing technique along with hemorrhage control achieved by hemostatic electrocoagulation or suture ligation. A drainage tube was placed after hemostasis.
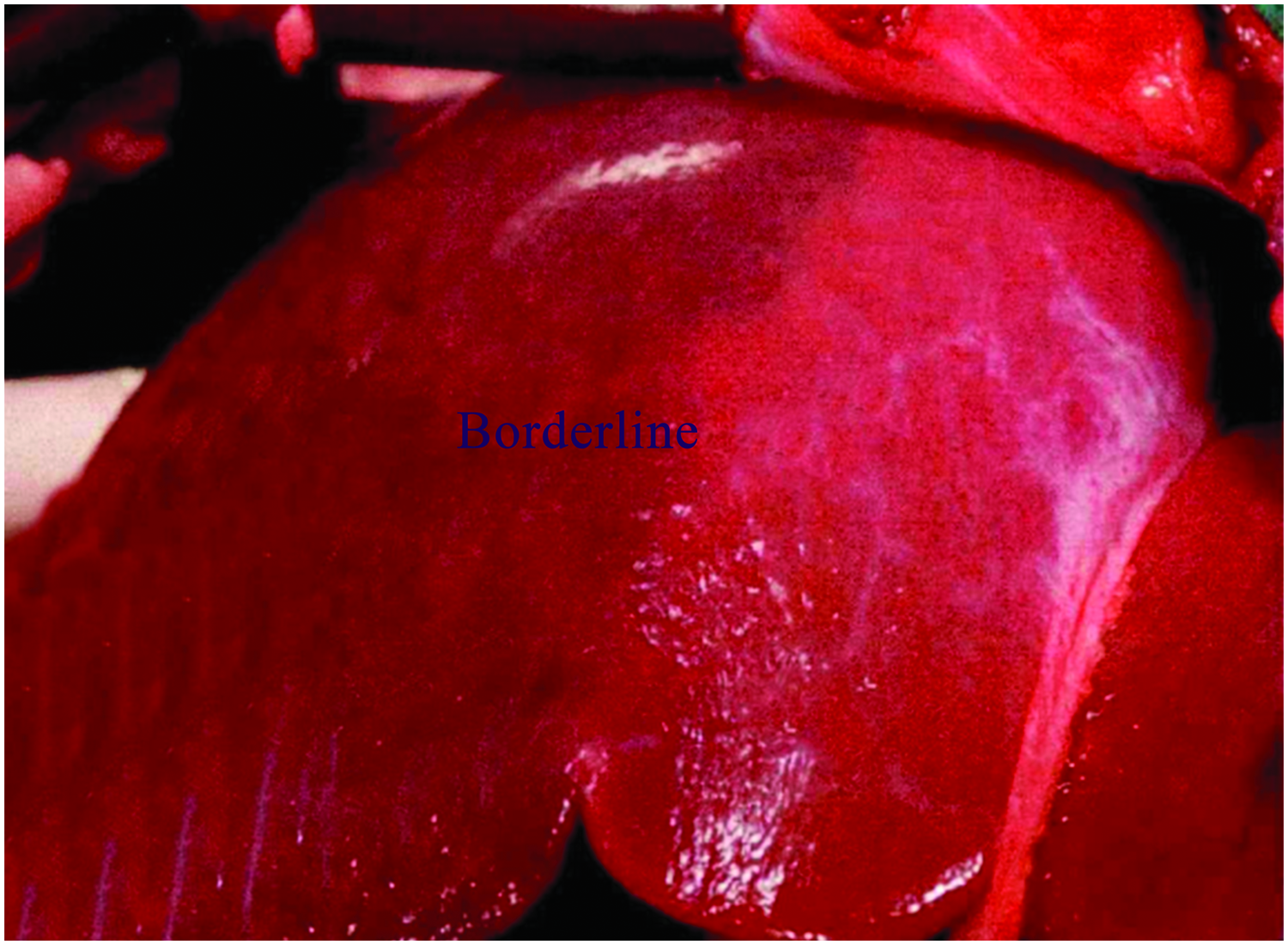
The boundary lines of the ischemic regions on the hepatic surface.
Measurements
All demographic and clinical data were retrieved from medical records. Preoperative clinical parameters that were evaluated included age, sex, and severity of cirrhosis defined by the Child–Pugh classification. Liver function was monitored by serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin (TB) at preoperative baseline and postoperative days 1, 3, and 7. Intraoperative parameters, including range of hepatic resection, blood loss volume, rate of blood transfusion, and operation time, as well as postoperative parameters, including major complications (bile leakage, ascites, and hemorrhage) and length of hospital stay, were analyzed.
Statistical analyses
Numerical data were expressed as mean ± standard deviation if normally distributed and as median (interquartile range) if not normally distributed. Group differences were compared using Student's t-test or analysis of variance (ANOVA) for numerical data following a normal distribution as appropriate and using Wilcoxon signed-rank test for numerical data not normally distributed. Categorical data were compared with Pearson's chi-square test. A two-sided P value <.05 was taken as statistically significant. SPSS version 18.0 (SPSS, Inc., Chicago, IL) was used for statistical analyses.
Definitions
Operative time was calculated as the time from skin incision to the entire skin closure. Blood loss was recorded carefully by the anesthetist through a Postoperative Complications vacuum system. Length of stay was defined as the days from admissions to discharge. Bile leakage 9 was defined by international study group of Liver surgery as bilirubin concentration in the drain fluid at least thrice the serum bilirubin concentration on or after postoperative day 3 or as the need for radiologic or operative intervention resulting from biliary collections or bile peritonitis. Posthepatectomy hemorrhage 10 is defined as a drop of hemoglobin level >3 g/dL after the end of surgery compared to postoperative baseline level and/or any postoperative transfusion of packed red blood cells for a falling hemoglobin and/or the need for invasive reintervention (e.g., embolization or relaparotomy) to stop bleeding; Postoperative ascites 11 was defined as daily ascite fluid drainage exceeding 500 mL and/or grade 2 ascites in ultrasonography, computed tomography, or clinical assessment showing a moderately symmetrical distension of the abdomen.
Results
No significant differences in age, sex, and tumor size were observed between the Glisson and Pringle groups (Table 1). Cirrhosis was observed in 80% and 60% of patients allocated to the Pringle and Glisson groups, respectively, and this difference also was not statistically significant. Hemihepatectomy was performed in 72% of patients in both groups. As shown in Table 1, the average operation time for the Pringle maneuver approach was comparable to that for the Glissonean pedicle approach, but the blood loss volume in the Pringle group (median, 600 mL) was significantly greater than that in the Glisson group (median, 50 mL, P < .001). Intraoperative transfusion was required in 35% of patients in the Pringle group, and this was significantly higher than the rate of 8% of patients in the Glisson group (P < .05).
Clinical and Operative Characteristics of Patients Allocated to the Pringle Maneuver Group or Glissonean Pedicle Transection Group for Hepatic Resection
SD, standard deviation.
Liver function, as indicated by the ALT, AST, and TB levels, was compared between the groups before and after surgery (Table 2). The preoperative serum levels of ALT, AST, and TB did not differ significantly between the Glisson and Pringle groups. However, the postoperative serum levels of ALT, AST, and TB were significantly lower in the Glisson group than in the Pringle group at 1, 3, and 7 days after surgery. In the Glisson group, the ALT, AST, and TB levels temporarily increased dramatically after surgery and then gradually returned to close to preoperative levels by postoperative day 7. A similar trend was observed for patients in the Pringle group, but by postoperative day 7, the ALT, AST, and TB levels remained obviously higher than the preoperative levels.
Preoperative and Postoperative Serum Levels of Alanine Aminotransferase, Aspartate Aminotransferase, and Total Bilirubin in Patients Allocated to Pringle Maneuver or Glissonean Pedicle Transection for Hepatic Resection
Post-op, postoperative.
One patient (4%) in each group developed bile leakage, with no difference in the incidence of this complication between groups (Table 3). Significantly more patients in the Pringle group developed postoperative ascites compared with the Glisson group (40% versus 6%, P = .024). Six patients (24%) in the Pringle group had hemorrhagic complications, while no hemorrhage was observed in the Glisson group, resulting in a significant between-group difference (P = .030). Specimens resected in the Glisson group had a significantly lower percentage of positive margins than those resected in the Pringle group (8% versus 36%, P = .017). Patients in the Pringle group had a significantly longer length of hospital stay compared with patients in the Glisson group (17.64 ± 3.83 days versus 13.72 ± 2.97 days, P < .001).
Complications and Outcomes in Patients Allocated to the Pringle Maneuver Group or Glissonean Pedicle Transection Group for Hepatic Resection
SD, standard deviation.
Discussion
Viral hepatitis and hepatic cirrhosis are common diseases that pose a great health burden to China. 12 More than half of all primary liver cancer cases diagnosed annually worldwide occur in China. 1 Despite recent advances in radiotherapy and systemic therapies, surgery remains the primary treatment for most liver cancer cases. Of note, patients with HCC frequently present with cirrhosis, and cirrhotic liver is commonly considered to be sensitive to ischemia. Kajikawa et al. found that the increased risk of mortality and delayed postoperative hospital stay for hepatectomy were associated with intraoperative blood loss aggravated by portal hypertension, hypersplenism, and abnormal coagulation accompanying cirrhosis. 13 Therefore, factors crucial to the success of surgical treatment and outcomes for patients with HCC are effective control of intraoperative and postoperative hemorrhage, shortening of operation time, and preventing damage to residual liver function. In this regard, various types of vascular occlusion techniques have been introduced, and the Pringle maneuver is a classical surgical technique for vascular inflow occlusion.
First described by Pringle in 1908, 4 the Pringle maneuver clamps the hepatoduodenal ligament to occlude the blood flow through the hepatic artery and portal vein and thus decrease hemorrhage during hepatic resection. Normal liver is capable of tolerating continuous warm ischemia for about 60 minutes, while cirrhosis in the liver lowers the safe threshold for ischemia to 15–20 minutes. Much remains to be elucidated about factors that influence hepatic ischemia and reperfusion and can accurately predict tolerable ischemia time. Chen et al. found that the average warm ischemia time was 31.4 minutes using the Pringle maneuver, and the threshold for continuous ischemia could even exceed 60 minutes. 14 The liver seems more tolerant to intermittent blood flow occlusion, which typically consists of clamping of the portal triad for 15–30 minutes and reperfusion for 5 minutes. Ishizaki et al. revealed that the cumulative time could exceed 120 minutes when using intermittent clamping with no notable increase of hemorrhage or major complications. 15 Ischemic preconditioning, typically comprising 5–10 minutes of ischemia and 5–10 minutes of reperfusion, has proven to be effective in prolonging the tolerable ischemia time and protecting liver function during hepatic resection.16–18 Petrowsky et al. found that although a similar liver function protective effect was observed for noncirrhotic patients receiving major hepatic resection, ischemic preconditioning with continuous clamping resulted in lower intraoperative hemorrhage and shorter transection time compared with intermittent clamping. 19
The advantages of the Pringle maneuver are that it is simple to execute and widely indicated, except in cases with tumors invading the portal and caval veins. 20 However, clamping of the hepatoduodenal ligament does not restrict backflow bleeding from hepatic veins and induces stasis of the portal vein, superior mesenteric vein, and inferior mesenteric vein, which lead to gut barrier disruption and thus increased risks of bacterial infection and leakage of endotoxins. 21 Moreover, ischemia–reperfusion injury remains a potential problem for patients undergoing the Pringle maneuver, because ischemia–reperfusion injury makes patients more prone to developing liver failure, especially those with cirrhosis, 7 and has been associated with recurrent growth of liver neoplasms. 22 To overcome the detrimental effects of the Pringle maneuver, the Glissonean pedicle transection method adopted a classification based on the ramification of the secondary Glissonean pedicle and divided the liver into three segments, which are further divided into 6–8 cone units with tertiary branches for selective transection. 8 This Glissonean pedicle approach is suitable for anatomical hepatectomy with effective control of bleeding and complete perfusion of residual normal liver, but may be limited by backflow bleeding and air embolism from the hepatic veins. In our study, the Glissonean pedicle transection combined with HVE led to much less intraoperative hemorrhage compared with the Pringle maneuver, and only 2 patients needed intraoperative blood transfusions during major hepatic resection. This is consistent with the findings of Giuliante et al., who reported preliminary exclusion of the hepatic veins as an effective way to reduce the need for intraoperative blood transfusions from 44.4% in a non-HVE group to 11.1% in a HVE group. 23 Moreover, liver function evaluation by serum ALT, AST, and TB levels revealed better reserved residual liver function in patients undergoing the Glissonean pedicle transection, supporting that less ischemia–reperfusion injury occurred with this surgical procedure. Less postoperative hemorrhage and ascites were identified in the Glisson group, along with a shorter length of hospital stay. This is in line with the results of Tsujita et al., who reported a correlation of severe postoperative complications with intraoperative hemorrhage and blood transfusion after hepatic resection. 24
Hepatic resection and subsequent regeneration provide a local microenvironment in favor of microscopic residual tumor growth, partly mediated by Kupffer cell-dependent mechanisms. 25 This tumor growth effect may be deteriorated by immunosuppression induced by allogeneic blood transfusion, which has been shown to impair immune surveillance of cancer cells in blood recipients and increase HCC recurrence after resection.26,27 Intrahepatic metastasis is a major cause of HCC recurrence. The Glissonean pedicle transection is an anatomic resection, which removes the tumor together with the corresponding portal veins and hepatic territory. This anatomic resection approach prevents cancer cells from spreading through the hepatic portal system, which is considered to be the primary mechanism of intrahepatic metastasis.28,29 Wakai et al. observed significantly improved survival with anatomic resection compared with nonanatomic resection for T1–T2 stage HCC. 29 Our study did not include a follow-up assessment, and thus, the long-term survival and recurrence outcomes could not be compared between the groups treated with the Glissonean pedicle transection and Pringle maneuver. However, the Glissonean pedicle transection was associated with a lower rate of positive margins, suggesting a reduced risk for postoperative recurrence. 30 Nakai et al. reported an increased risk of bile leakage with Glissonean pedicle transection, 31 but in our study, the rate of bile leakage after Glissonean pedicle transection was much lower than previously reported (4% versus 23.4% in Nakai et al.'s study) and was not different from that after the Pringle maneuver. More studies are needed to evaluate the potential adverse effects of this surgical approach.
The Glissonean pedicle transection with HVE requires an experienced surgeon who can identify the Glissonean system and recognize surgical structures of the Glisson pedicle trees. In our study, the operation time was comparable to that for the Pringle maneuver, likely due to less bleeding, improved surgical field visualization, and no need for intermittent clamping with a reperfusion period in the Glissonean pedicle transection procedure.
In conclusion, the Glissonean pedicle transection with HVE is a safe and effective approach to controlling hemorrhage and protecting residual liver function compared with the classic Pringle maneuver with intermittent clamping for surgical resection of HCC. This approach is not an option if the tumor involves the portal pedicles to the hepatic hilum. Special attention should be given to avoid major hemorrhage possibly caused by variations in venous and Glissonean pedicle anatomy of the liver. Combinations of imaging techniques such as three-dimensional computed tomography angiography and intraoperative ultrasound localization with clinical features of individual patients hold great promise in precision medicine for improving hemorrhage control and clinical outcomes of patients with HCC in the future. Our results encourage more and larger studies regarding improvement of the Glissonean pedicle transection method to achieve optimal therapeutic effects against liver cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The study did not receive any specific funding from public, commercial, or non-profit sector funding agencies.