
Abstract
Abstract
Background:
To clarify the definite incidence of isolated tumor cells (ITCs) in lateral lymph nodes (LLNs) and its prognostic significance in rectal cancer patients after laparoscopic lateral lymph node dissection (lap-LLND).
Methods:
Consecutive rectal cancer patients who underwent standard total mesorectal excision (TME) and lap-LLND were included. All the LLNs were re-examined by hematoxylin and eosin (H&E) stain and immunohistochemistry (IHC) with a monoclonal antibody against cytokeratin 20 to confirm the status of ITCs, micrometastasis, and overt metastasis. Clinicopathological characteristics and oncological outcomes were analyzed.
Results:
Forty-six patients with TME and lap-LLND were included. Twelve (26.1%) patients with overt metastasis were identified. A total of 705 LLNs from 46 patients were re-examined by H&E with IHC, and ITCs were detected in 27 (3.8%) lymph nodes from 11 (23.9%) patients. No LLNs micrometastasis was found. Patients with overt metastasis had more advanced N stage and more perirectal lymph nodes metastasis. Three patients with LLNs recurrence were identified and lung metastasis was the most common metastatic site. Compared with patients with ITCs and without any metastasis, patients with overt metastasis had worse 3-year cumulative overall survival (85.7%, 83.9%, and 53.3%, respectively) and 3-year cumulative disease-free survival (85.7%, 85.2%, and 43.8%, respectively). Patients with ITCs had higher overall recurrence than patients without any metastasis (42.9% versus 11.5%, P = .035). Multivariate analysis showed that ITC status in LLNs was a significant prognostic factor (hazard ratio 2.689, 95% confidence interval 1.072–6.747; P = .035).
Conclusion:
ITCs in LLNs detected by the IHC method like overt metastasis detected by H&E staining contributed to higher overall recurrence.
Introduction
It is well known that lymph node metastasis detected on conventional histopathologic examination by using hematoxylin and eosin (H&E) staining (overt metastasis) was an important prognostic factor for colorectal cancer (CRC) and had an impact on treatment decision-making. 1 Up to 20%–30% of patients with stage I/II CRC die as a result of recurrent disease. 2 This demonstrated that occult metastatic disease including isolated tumor cells (ITCs) or micrometastasis within regional lymph nodes might play a role in systemic tumor spread. 3 Some systematic reviews and meta-analysis had confirmed that occult disease detected by using molecular detection techniques such as immunohistochemistry (IHC) or reverse transcriptase–polymerase chain reaction (RT-PCR) was associated with disease recurrence and poor survival in patients with node-negative CRC.4,5
Recently, the management of lateral lymph nodes (LLNs) in patients with rectal cancer has increasingly become an important clinical issue. 6 However, as prophylactic lateral lymph node dissection (LLND) is not widely accepted in the world other than Asian countries, there is still controversy on whether occult disease (ITCs or micrometastasis) within LLNs had an impact on prognosis in rectal cancer patients.7,8 To clarify this issue, we perform a retrospective study to evaluate the prognostic significance of occult disease in LLNs detected by the IHC method.
Materials and Methods
Study population
Between 2010 and 2017, patients with locally advanced low rectal cancer who underwent standard total mesorectal excision (TME) and laparoscopic LLND (lap-LLND) at our institution were included. The indication of lap-LLND in our hospital was patients with suspected LLNs on pretreatment imaging. All of these patients had no distant metastasis at surgery and underwent curative resection. Patients without available paraffin-embedded LLNs were excluded. All the information was collected from the prospective database. Informed consent was obtained from all patients before surgery.
Clinical staging and treatment strategy
Patients' clinical staging included physical examination, laboratory test, computed tomography (CT), and magnetic resonance imaging. In our center, LLNs were regarded as regional lymph nodes, and LLN metastasis was considered as a regional disease based on the Japanese guideline. 9 lap-LLND was performed in patients with clinically suspected LNN metastasis, which based on pretreatment imaging characteristics included tumor location, tumor stage, LLNs short-axis diameter, and LLN malignant features (border irregularity and mixed signal intensity).10–15 Overall, patients with advanced rectal cancer received 5-fluorouracil-based neoadjuvant chemoradiotherapy (nCRT) with a total dose of 45 or 50.4 Gy, which was determined by the multidisciplinary team meeting. Usually, the operation was performed 8–12 weeks after completion of nCRT. Patients with high-risk stage II or stage III, 5-fluorouracil-based adjuvant chemotherapy was recommended.
TME and lap-LLND procedure
All operations were performed by surgeons specializing in both standard TME and lap-LLND. According to the Japanese guideline, LLNs were divided into four parts: the internal iliac, obturator, external iliac, and common iliac nodes. 9 After completion of the TME procedure, lap-LLND was performed. The lateral, medial, cranial, caudal, and dorsal anatomical borders of lap-LLND were the external iliac artery, pelvic plexus, bifurcation of the common iliac artery, levator ani muscle, and sciatic nerve, respectively. During the entire procedure, the ureter, obturator, and pelvic autonomic nerves were identified and protected carefully.
Pathology and IHC
The surgical resection specimens were evaluated using a standardized protocol in our pathology department. 16 To evaluate the definite status of LLNs micrometastasis, the IHC method was used to re-examine the conventional pathological negative LLNs. In brief, two serial 4 μm sections were cut from the paraffin blocks of all the LLNs and stained with H&E and anticytokeratin (CK) antibody CK20 (ZsBio, Beijing, China). Sections from the primary tumor were set as the positive control. Negative control was set with phosphate-buffered saline stained by using another section from LLNs. A streptavidin–biotin immunoperoxidase method was used. The staining procedures have been previously described in detail.8,17 All slides were reviewed by independent experienced pathologists (D.J. and X.D.) who were blinded to clinical data.
According to the 8th Union for International Cancer Control guideline, micrometastasis was defined as a metastatic focus measuring between 0.2 and 2 mm in diameter or clusters of >20 cells and ITCs including single cancer cells and small cell clusters (up to 20 tumor cells). 18 In this study, patients with LNN metastasis detected by conventional H&E examination were defined as patients with overt metastasis. Patients with ITCs in LLNs detected by IHC were defined as patients with ITCs. Patients with LLNs micrometastasis detected by IHC but without overt metastasis and ITCs were defined as the patients with micrometastasis. Patients who had no LLNs overt metastasis or micrometastasis or ITCs were defined as the patients without any LNN metastasis.
Follow-up
The follow-up after surgery was in accordance with the National Comprehensive Cancer Network guideline. In brief, all patients were followed up every 3 months for the first 2 years and then annually thereafter until 5 years. Blood test including carcinoembryonic antigen and CA199 was performed every 3 months and chest and abdominal CT scans were performed every 6 months for 2 years and henceforth annually. In addition, colonoscopy examination would be performed 1 year after the operation and repeated every 3 years if no lesions were confirmed. Distal recurrence and local recurrence were recorded.
Statistical analysis
All statistical analyses were performed using SPSS® software version 20.0 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.). Data are presented as frequencies (percentages) for categorical variables, and Fisher's exact test or χ2 test was used to analyze the categorical variables. The Kaplan–Meier method with the log-rank test was used to compare the survival curves. The Cox proportional hazards model was used to assess the prognostic significance of clinicopathologic features for recurrence after surgery. P value <.05 was considered statistically significant.
Results
Demographic characteristics and incidence of ITCs
Forty-six consecutive patients with TME and lap-LLND were identified from the prospectively collected data. A total of 705 LLNs from 46 patients were re-evaluated by H&E and IHC method. Twelve (26.1%) patients had LLNs overt metastasis detected by H&E staining. ITCs were detected in 27 (3.8%) LLNs from 11 (23.9%) patients (Fig. 1). Of these 11 patients, 7 patients were proved to only have ITCs detected by IHC and 4 patients had both LLNs overt metastasis detected by H&E and ITCs detected by IHC. There were no patients with LLNs micrometastasis. Therefore, 7 patients with ITCs in LLNs, 12 patients with LLNs overt metastasis, and 27 patients without LLNs metastasis were identified. The clinicopathological features were compared among those patients, as shown in Table 1. Patients in the overt metastasis group had more advanced clinical or pathological N stage, and perirectal lymph node metastasis was more common in this group.
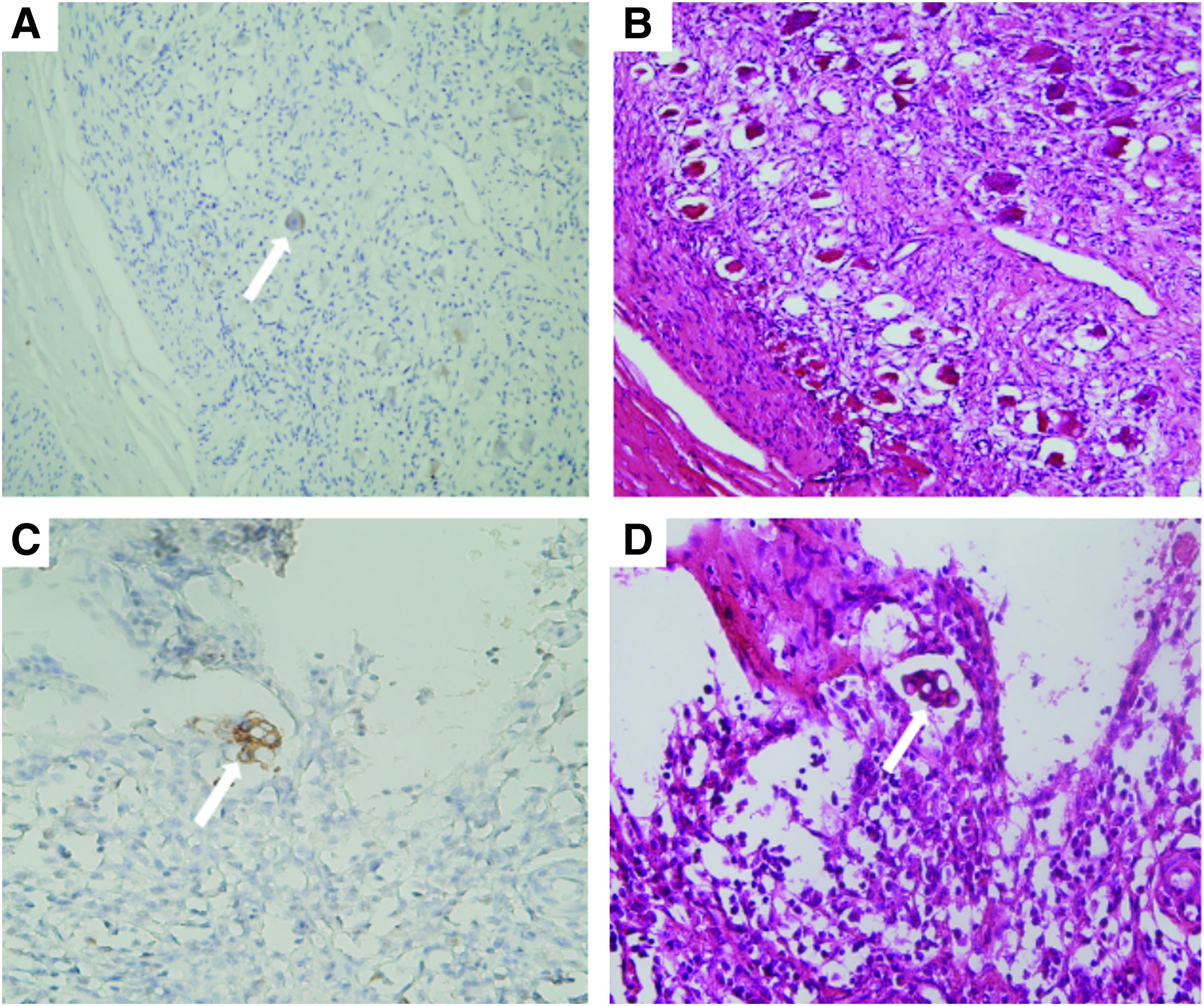
A single cancer cell was detected by immunostaining with CK20 in lymph node (arrow)
Clinicopathological Features Among Patients with Lateral Lymph Nodes Metastasis (Isolated Tumor Cells or Overt Metastasis) or Patients Without Any Lateral Lymph Nodes Metastasis (n = 46)
Bold indicates P values considered to be statistically significant.
Data are n (%).
Median (range).
CEA, carcinoembryonic antigen; ITCs, isolated tumor cells; LLN, lateral lymph node.
Oncological outcomes
The median follow-up time was 37.5 months (range 2–124). The recurrence after survival is summarized in Table 2. Recurrence disease developed in 4 out of the 7 patients (57.1%) with ITCs in LLNs and 7 out of 12 (58.3%) patients with LLNs overt metastasis and 5 out of 27 (18.5%) patients without LLNs metastasis. Three patients (6.5%) with lateral pelvic local recurrence were identified in each group. Notably, the lung was the most common metastatic site in each group.
Location of Recurrence After Curative Resection for Rectal Cancer
Numbers in parentheses represent percentage of patients with recurrence in total population.
Numbers in parentheses represent the proportion of specific recurrence site in all recurrences.
ITCs, isolated tumor cells; LLN, lateral lymph node.
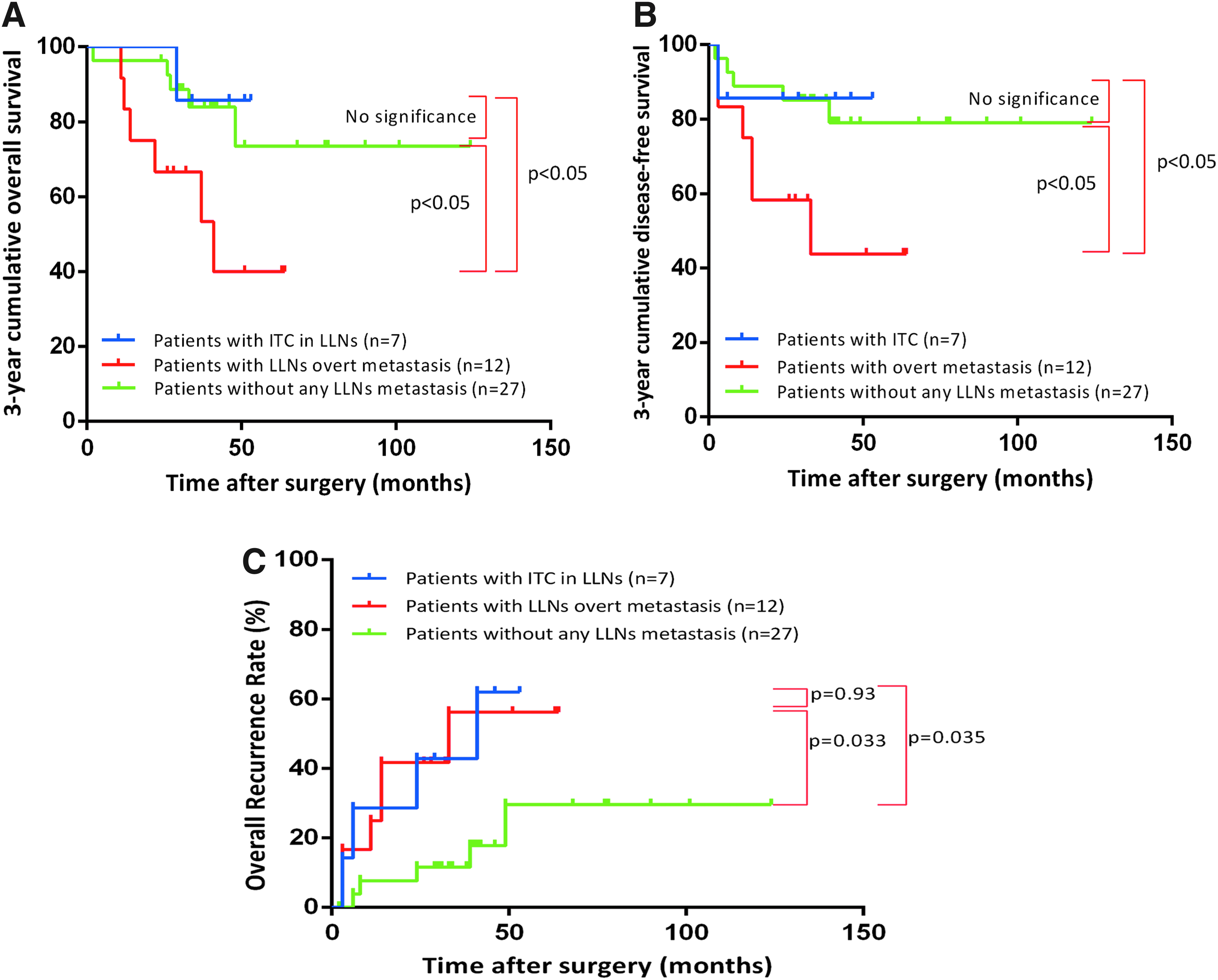
The 3-year cumulative overall survival (OS) in patients with ITCs, overt metastasis, and without any LLNs metastasis was 85.7%, 53.3%, and 83.9%, respectively (Fig. 2A). The 3-year cumulative disease-free survival (DFS) in patients with ITCs, overt metastasis, and without any LLNs metastasis was 85.7%, 43.8%, and 85.2%, respectively (Fig. 2B). Patients with overt metastasis had worse OS and DFS compared with patients with ITCs and without any LLNs metastasis. The 3-year cumulative overall recurrence rate in patients with ITCs, overt metastasis, and without any LLNs metastasis was 42.9%, 56.3%, and 11.5%, respectively (Fig. 2C). With regard to the overall recurrence rate, patients with ITCs in LLNs had higher overall recurrence rate than patients without any LLNs metastasis.
Multivariate analysis of the 34 patients without LLNs overt metastasis was performed to ascertain risk factors for recurrence after curative resection (Table 3). The results showed that age and ITC status in LLNs were significant prognostic factors (hazard ratio [HR] 0.104, 95% confidence interval [CI] 0.012–0.910; P = .041) (HR 2.689, 95% CI 1.072–6.747; P = .035).
Multivariate Cox Regression Analysis of Risk Factors for Recurrence After Surgery in Patients with Isolated Tumor Cells and Patients Without Any Lateral Lymph Nodes Metastasis (n = 34)
Bold indicates P values considered to be statistically significant.
CEA, carcinoembryonic antigen; CI, confidential interval; ITCs, isolated tumor cells.
Discussion
Although overt lymph nodes metastasis had been confirmed as a prognostic risk factor, due to the inconsistent reports, the prognostic significance of molecular tumor cell detected in regional lymph nodes of patients with node-negative CRC remained unclear.4,19 This discrepancy may be explained by the lesser number of events compared with patients with overt lymph nodes metastasis, a wide range of applied detection assays (IHC or RT-PCR), and different standardization.4,20
As a sensitive method for detecting occult metastasis missed by conventional H&E staining, the IHC method was used to identify micrometastasis in various malignancies. 7 However, there remains controversial on the prognostic significance of lymph nodes micrometastasis detected by the IHC method, especially for CRC. 7 Some earlier studies found that occult disease in lymph nodes detected by the IHC method only had limited prognostic value over conventional histologic staging.21,22 However, more studies showed that the IHC technique was capable of identifying occult disease in lymph nodes missed by conventional H&E staining, and occult disease confirmed in patients with Dukes' B CRC was significantly associated with poorer survival outcomes and higher recurrence.23–25 CK staining of lymph nodes was recommended for those patients. The heterogeneity among these studies might be caused by the usage of different anti-CK antibody.
One systemic review with meta-analysis showed that molecular detection of occult disease in regional lymph nodes was associated with an increased risk of disease recurrence and poor survival in patients with node-negative CRC. Furthermore, the prognostic significance of molecular tumor cell detection was independent of the applied detection method, molecular target, and number of retrieved lymph nodes. 4 Although more date on the occult disease was needed to determine their prognostic significance, the latest edition (8th) American Joint Committee on Cancer (AJCC) guideline still had an extended discussion of the prognostic significance of ITCs and micrometastasis and the surgeon should deal with this issue with caution.18,26
Recently, more and more evidence had confirmed that LLNs recurrence was the major pattern of locoregional recurrence in rectal cancer even after preoperative nCRT.27,28 Thus, more attention was paid to the treatment of LLNs in rectal cancer patients. 6 However, as prophylactic LLND is not widely accepted in the world, the definitive status and prognostic influences of LNNs micrometastasis in patients with rectal cancer also remain unclear.
To date, there were no more studies concerned on the prognostic significance of ITCs in LLNs in patients with rectal cancer, except the only two studies from Japan. Unfortunately, the results of the two studies were opposite.7,8 In 2003, Shimoyama et al. used an immunohistochemical method with CAM5.2 to detect LLNs micrometastasis in lower rectal cancer and found that LLNs micrometastasis represented a poor prognosis and should be regarded as overt metastasis. However, CAM5.2 antibody was used to detect occult disease in various gastrointestinal and biliary cancers. 7 Therefore, due to relatively low specificity, this method might bring bias. In 2007, Hara et al. reported that compared with H&E positive LLNs, ITCs in LLNs had no impact on prognosis. 8 Actually, heterogeneity existed in different populations with varied risk profiles, data on ITCs from different regions were needed.
Herein, we present data from China. CKs were used for molecular tumor cell detection in the majority of studies. The AJCC guideline also recommends the use of IHC method to detect occult disease, which was based on the time and cost consideration. 4 Therefore, we adopted the IHC method with CK20 monoclonal antibody to identify the occult disease in LLNs. According to our studies, a relatively high incidence of ITCs in LLNs (23.9%) was found. Although ITCs in LLNs had no impact on the 3-year cumulative OS and DFS in rectal cancer patients, it did contribute to the higher overall recurrence like over metastasis detected by H&E staining. Moreover, ITCs in LLNs were the independent prognostic factor for overall recurrence.
This study had limitations with its retrospective nature and relative small-scale simple size. In the future, prospective studies with a large scale are needed to confirm this finding.
Conclusion
In conclusion, the results of this study had demonstrated that a relatively high incidence of ITCs in LLNs was detected by IHC. ITCs had an important impact on overall recurrence in patients with rectal cancer. The issue should cause attention and be handled with caution.
Footnotes
Authors' Contributions
The cofirst authors, X.Y., T.H., C.G., and S.Y., performed the research, collected and analyzed the data, and drafted the article. D.J. and X.D. collected and analyzed the data and revised critical intellectual content. Z.W. and Z.Z. designed the conception and revised critical intellectual content. All authors read and approved the final article and agreed to be accountable for all aspects of the study to ensure that questions regarding accuracy and integrity are investigated and resolved.
Disclosure Statement
No conflicts of interest exist.
Funding Information
This study was supported by the Department of Science and Technology of Sichuan Province (Award Number 2016SZ0043), West China Hospital of Sichuan University (Award Number ZY2016105), and the National Natural Science funding of China (Award Number 81401990).