
Abstract
Background:
The application of laparoscopic surgery using instruments that are 3 mm or less in diameter for patients with early gastric cancer (EGC) has not yet been established. We aimed to evaluate the feasibility and safety of laparoscopic gastrectomy using instruments with minimal diameter.
Methods:
We retrospectively analyzed 41 patients who underwent laparoscopic subtotal gastrectomy with D1-positive lymph node dissection for EGC. Among them, 17 patients underwent laparoscopic gastrectomy using instruments with a minimal diameter (experimental group), while 24 patients underwent conventional laparoscopic gastrectomy (control group). In the experimental group, we used two 3-mm trocars, one 5-mm trocar, and the GelPOINT® Advanced Access Platform. We compared operative outcomes between the two groups and assessed the learning curve of laparoscopic gastrectomy using instruments with minimal diameter.
Results:
The operative outcomes were similar between the two groups. The preoperative-to-postoperative day 2 ratio of neutrophil count in the experimental group was significantly lower than in the control group (2.07 versus 2.65; P = .038). Morbidity was not observed in the experimental group and 3 patients experienced complications in the control group, although it was not significantly different (P = .252). The operation time according to the accumulation of cases was stable without any significant change in the experimental group.
Conclusions:
Laparoscopic gastrectomy using instruments with minimal diameter is technically feasible and safe for EGC and could also be a good alternative to conventional laparoscopic gastrectomy to minimize the impact of surgical invasiveness when performed by experienced surgeons.
Introduction
Laparoscopic gastrectomy with lymph node dissection (LND) has been widely accepted as a standard alternative for the treatment of early gastric cancer (EGC), 1 and has been popularly performed in East Asian countries, such as Korea and Japan.2–4 One recent multicenter randomized controlled clinical trial proved that laparoscopic gastrectomy was revealed as superior in terms of surgical outcomes 5 and noninferior regarding its postoperative survival rate 6 compared to open gastrectomy in patients with EGC.
Conventional laparoscopic surgery for gastric cancer usually requires five incisions for 5- to 12-mm trocars to perform gastric resection with adequate LND and consequently mini-laparotomy for specimen extraction or reconstruction. 7 Although those procedures significantly reduce surgical invasiveness relative to open gastrectomy, surgeons have still endeavored to reduce the size and number of trocars for laparoscopic gastric cancer surgery to achieve even better postoperative outcomes and improve the quality of life. Remarkable advancements in minimally invasive surgery, such as novel approaches and improved equipment, have led to the development of new procedures such as single- or reduced-port surgeries.8–11 However, those kinds of procedures have not been popular due to the required learning curve even in experienced surgeons for laparoscopic surgery. 12
Some researchers have tried to replace the standard 5-mm or larger sized trocars used during conventional laparoscopic surgery with novel instruments that have a 3-mm or less diameter, which are used during laparoscopic cholecystectomy, 13 herniorrhaphy,14,15 and salpingo-oophorectomy. 16 These previous studies concluded that the laparoscopic procedures using instruments with a minimal diameter were feasible and could be a good alternative to conventional procedures in those surgeries.
Unlike the relatively uncomplicated operations, laparoscopic gastrectomy with lymphadenectomy for gastric cancer requires more sophisticated procedures such as a variety of vessel ligation and dissection for perivascular lymph nodes (LNs). Recently developed instruments with a minimal diameter might accomplish complicated procedures like conventional laparoscopic operation. However, this has not been proven in clinical studies regarding laparoscopic surgery for gastric cancer.
Here, we designed laparoscopic gastrectomy using instruments with a minimal diameter for patients with EGC. The main object of this study was to investigate the feasibility and safety of laparoscopic gastrectomy using instruments with a minimal diameter to conventional laparoscopic gastrectomy. In addition, we aimed to evaluate the learning curve for laparoscopic gastrectomy using instruments with minimal diameter.
Methods
Study design and patients
The Institutional Review Board of the Ajou University Hospital, Suwon, Korea approved this study (AJIRB-MED-19-122). We retrospectively reviewed the medical records of 41 consecutive patients who underwent subtotal gastrectomy for EGC either by laparoscopic surgery using instruments with minimal diameter or conventional laparoscopic surgery from January 2017 to September 2017 at the Department of Surgery, Ajou University School of Medicine. Of 41 patients, 17 underwent laparoscopic gastrectomy using instruments with a 3-mm or less diameter (experimental group); the other 24 underwent conventional laparoscopic gastrectomy (control group).
Starting in January 2017, we performed laparoscopic gastrectomy using instruments with minimal diameter. We included initial and subsequent patients in the experimental group and patients in the same period in the control group. We excluded patients with upper-third gastric cancer that required total gastrectomy. All cases of gastrectomy were performed by a single surgeon (H.H.) who had previously performed about 500 and more laparoscopic gastrectomies for gastric cancer. Regardless of the introduction of instruments with a minimal diameter, the preoperative care protocols, operative procedures, and postoperative care protocols remained the same throughout the study period.
Conventional laparoscopic gastrectomy
We performed conventional laparoscopic subtotal gastrectomy with LND using two 12-mm trocars and two 5-mm trocars. One 12-mm trocar was inserted into the infra-umbilicus for the laparoscope and the other 12-mm trocar was placed in the right lower quadrant area to introduce ultrasonic shears and laparoscopic surgical staplers. Two 5-mm trocars were inserted in the right upper and left lower quadrant area. The extent of gastric resection depended on the location and size of the primary tumor. Regarding the extent of LND, D1-positive LND was performed according to the Japanese gastric cancer treatment guidelines 2014 (ver. 4). 17 The resected specimen was inserted into a retrieval bag and extracted via infra-umbilical mini-laparotomy. The reconstruction of the digestive tract was performed with an intracorporeal anastomosis.
Laparoscopic gastrectomy using instruments with a minimal diameter
After induction of general anesthesia with endotracheal intubation, the patient was placed in a lithotomy position with legs apart. The surgeon stood on the patient`s right side. The first assistant stood on the patient's left side and the scopist stood between the patient's legs. We used the GelPOINT® Advanced-Access platform (Applied Medical, Rancho Santa Margarita, CA) since 12-mm trocar for laparoscopic surgical staplers and 10-mm trocar for laparoscope with high-definition camera are necessary for laparoscopic gastrectomy (Fig. 1a).
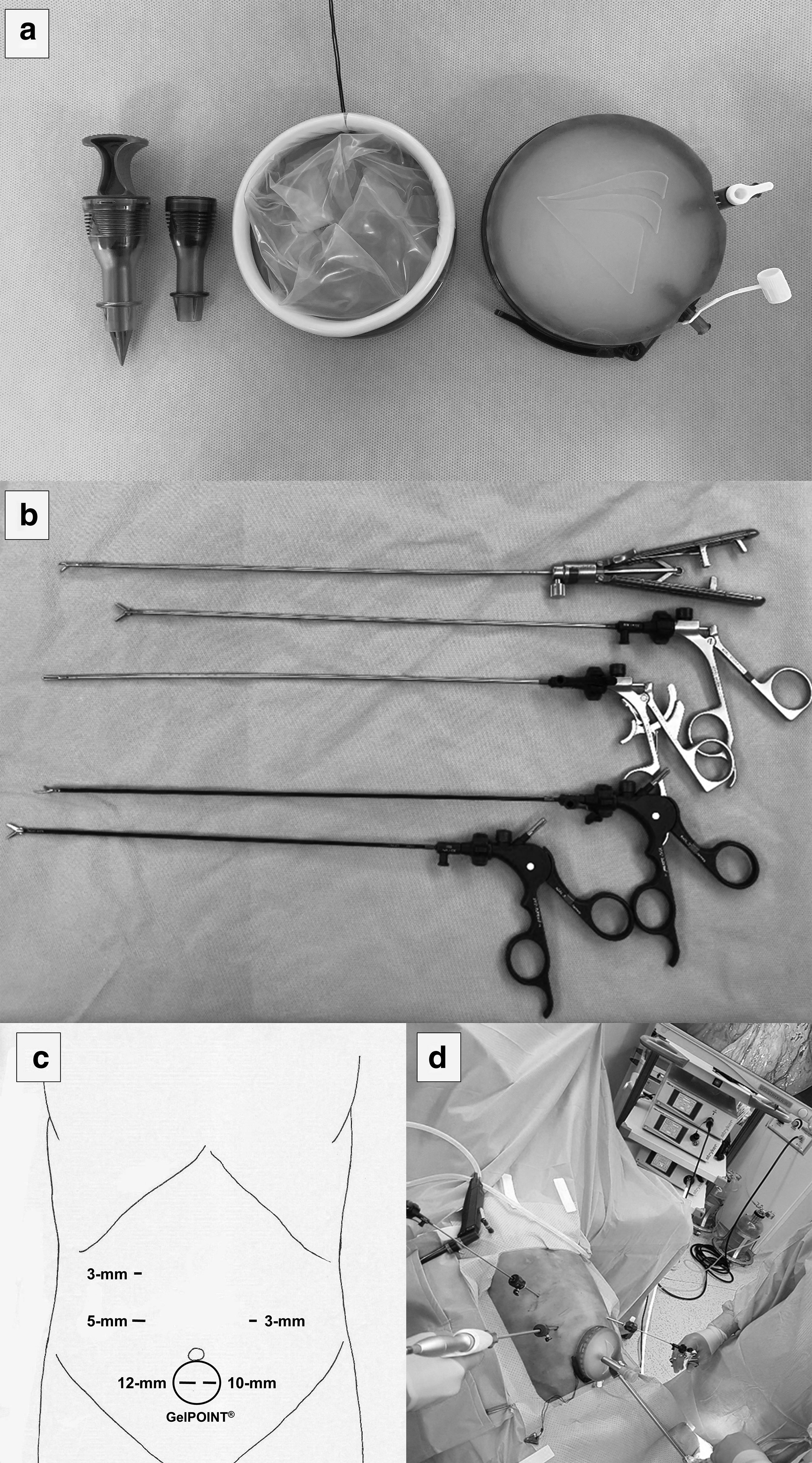
Instruments with minimal diameter for laparoscopic gastrectomy.
We made a 4-cm infra-umbilical incision perpendicular to the abdominal wall and inserted the Alexis Wound Protector® (GelPOINT Advanced-Access platform). Subsequently, after inserting 12-mm and 10-mm Low Profile Sleeves (GelPOINT Advanced-Access platform) into the GelSeal Cap (GelPOINT Advanced-Access platform), we sealed the GelSeal Cap onto the Alexis Wound Protector. A 10-mm Low Profile Sleeve was used to introduce the laparoscope and a 12-mm Low Profile Sleeve to introduce the laparoscopic surgical staplers.
After making pneumoperitoneum with insufflating carbon dioxide via the GelSeal Cap, two 3-mm trocars were inserted in the right upper and left lower quadrant areas to introduce graspers, scissors, and a needle holder with a 3-mm diameter (Fig. 1b), and a 5-mm trocar was placed at the right lower quadrant area to introduce ultrasonic shears under direct laparoscopic vision (Fig. 1c, d).
The gastric resection with LND was performed as in conventional laparoscopic gastrectomy. To ligate the vessels, except for the left gastric artery, a 5-mm clip was introduced through a 5-mm trocar at the right lower quadrant and a 10-mm clip was introduced through the 12-mm Low Profile Sleeve inserted in the Alexis Wound Protector for ligation of the left gastric artery (Fig. 2a, b). The staplers for resection of the duodenum and the stomach were introduced through the 12-mm Low Profile Sleeve inserted in the Alexis Wound Protector, and the gauzes were also introduced through this trocar if they were required to clear the operative filed.
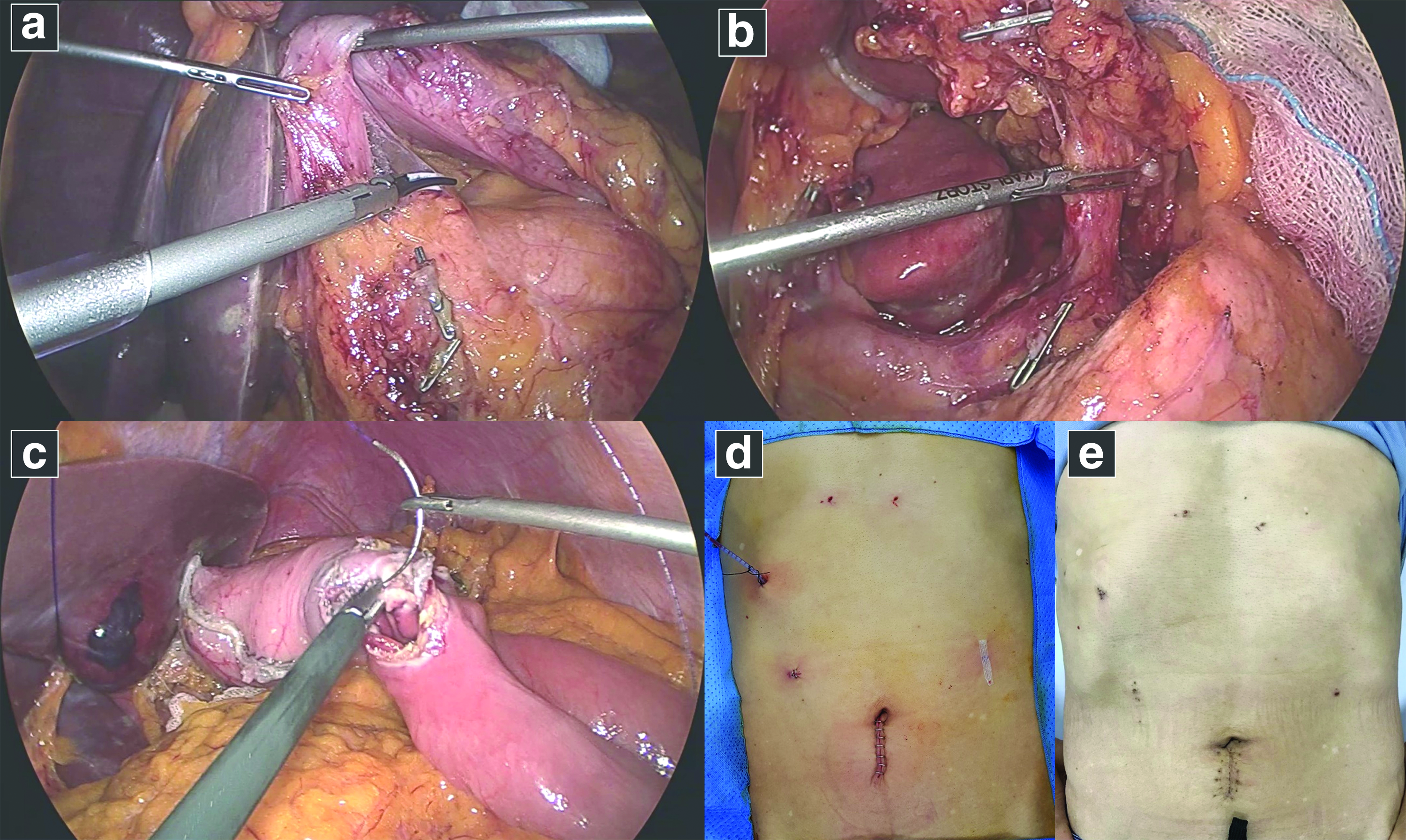
Intraoperative finding using instruments with a minimal diameter and surgical wound.
All patients underwent intracorporeal anastomosis for the reconstruction of the digestive tract. After anastomosis using an endoscopic linear stapler, we performed subsequent procedures to close the entry hole of the linear stapler using knotless barbed sutures with a 3-mm needle holder (Fig. 2c). Finally, the resected specimen was extracted through an infra-umbilical incision and closed suction drain with 100-cc was inserted into the 3-mm trocar site in the right upper quadrant. Except for the infra-umbilical wound, we approximated the edge of the skin incision without closure of the fascia and the subcutaneous layer (Fig. 2d, e).
Postoperative management
Both groups received the same postoperative management. On postoperative day (POD) 1, the urinary catheter was removed, and postoperative mobilization was encouraged. Sips of water were also initiated on POD 1, followed by a clear liquid diet and soft diet. Patient-controlled analgesia was used for postoperative pain control and oral analgesics were initiated with diet. Postoperative pain was scored from 0 to 10 using the visual analog scale. Patients without any complications were discharged on POD 5 or 6. Early postoperative complications were defined as any adverse event associated with the surgical procedure that required additional therapy within 30 days after surgery. Late postoperative complications were defined as occurring after POD 30. The follow-up period was 12 months after surgery.
Definition of the learning curve
We used the operation time to define the learning curve in the experimental group. We also included the number of retrieved LNs since it is a surrogate marker of long-term oncological outcomes. Overall trends of the operation time and number of retrieved LNs according to the number of cases were used to identify the effect of laparoscopic gastrectomy using instruments with minimal diameter. The rate of complications was not included since it was too low to perform a reliable statistical analysis.
Statistical analysis
Data analysis was performed using IBM SPSS® Statistics for Windows, Version 23.0 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.). Continuous variables were analyzed with the Student's t-test to compare the mean values. Categorical variables, which are presented as number (n) and percentage (%), were analyzed with the chi-square test or Fisher's exact test. Pearson's correlation coefficient was used to investigate the correlations between surgical experience and operation time, and between surgical experience and the number of retrieved LNs. Statistical significance was defined as a P value <.05 (two-sided).
Results
Patient characteristics
The mean age of the experimental group (55.6, range 34–77 years) was significantly lower than that of the control group (65.8, range 55–89 years; P = .010). However, when age was divided into younger than 65 and 65 years or more, there was no significant difference between the two groups (P = .114). The experimental group (n = 13, 76.5%) exhibited a significantly higher proportion of women than the control group (n = 8, 33.3%; P = .006). No significant differences were observed between the two groups, including body mass index, presence of preoperative endoscopic submucosal dissection, history of abdominal surgery, presence of medical comorbidities, and tumor locations (Table 1).
Clinical Characteristics of Patients
Bold values denote statistical significance at the p < 0.05 level.
Fisher's exact test.
Patients with any of the comorbidities of hypertension, diabetes mellitus, coronary artery disease, stroke, and COPD were categorized into the comorbidity group.
BMI, body mass index; COPD, chronic obstructive pulmonary disease; ESD, endoscopic submucosal dissection; SD, standard deviation.
Operative outcomes
At any time during the operation, the surgeon had the option of conversion to conventional laparoscopy or open surgery for the safety of the patients. However, there was no requirement for upsizing the trocars or conversion to open surgery in the experimental group. There was also no conversion to open surgery in the control group. We observed similar perioperative outcomes regarding the type of reconstruction, operation time, estimated blood loss, and duration of hospital stay between the two groups. We retrieved more LNs in the experimental group than in the control group, although it was not statistically different (40.1 [range, 29–60] versus 33.9 [range, 15–65]; P = .081). The overall morbidity rates were not significantly lower in the experimental group than in the control group (11.8% versus 16.7%; P = .999) (Table 2).
Operative Outcomes
Conversion to conventional laparoscopy or open surgery in experimental group and conversion to open surgery in control group.
Fisher's exact test.
N/A, not applicable; POD, postoperative day; SD, standard deviation.
When we examined laboratory parameters including white blood cell (WBC) count, hemoglobin level, neutrophil count, and C-reactive protein (CRP) level on pre- and postoperative days, the preoperative-to-POD 2 ratio of neutrophil count was significantly lower in the experimental group than in the control group (2.07 versus 2.65; P = .038). The preoperative-to-POD 2 ratio of WBC count and CRP level were similar between the two groups. The preoperative-to-POD 2 ratio of hemoglobin and pain scales on POD 2 was also not significantly different between the two groups (Fig. 3).
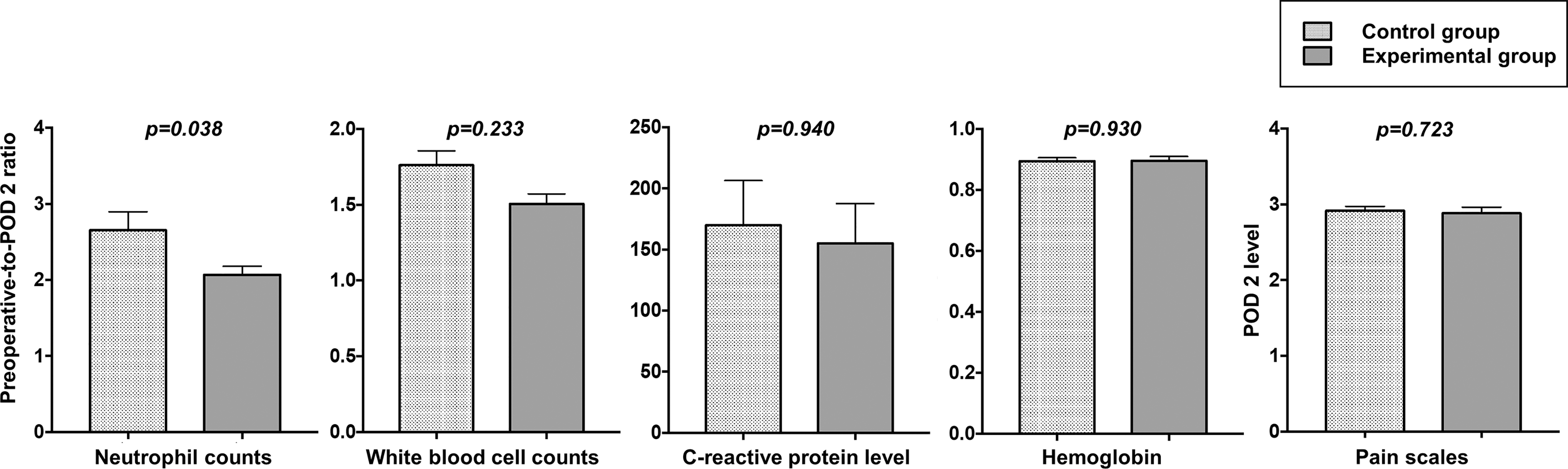
Comparison of inflammatory profiles, hemoglobin, and pain scales. Preoperative-to-POD 2 ratio of neutrophil counts, white blood cell counts, serum levels of C-reactive protein and hemoglobin, POD 2 level of pain scales. POD, postoperative day.
Learning curve for laparoscopic gastrectomy using instruments with minimal diameter
There was no significant change in overall trends of the operation time and number of retrieved LNs according to the number of cases from the initial operation. Pearson's correlation coefficient demonstrated no significant correlations between the accumulation of cases and the operation time (r = 0.156, P = .550), and between the accumulation of cases and the number of retrieved LNs (r = −0.211, P = .416) (Fig. 4).
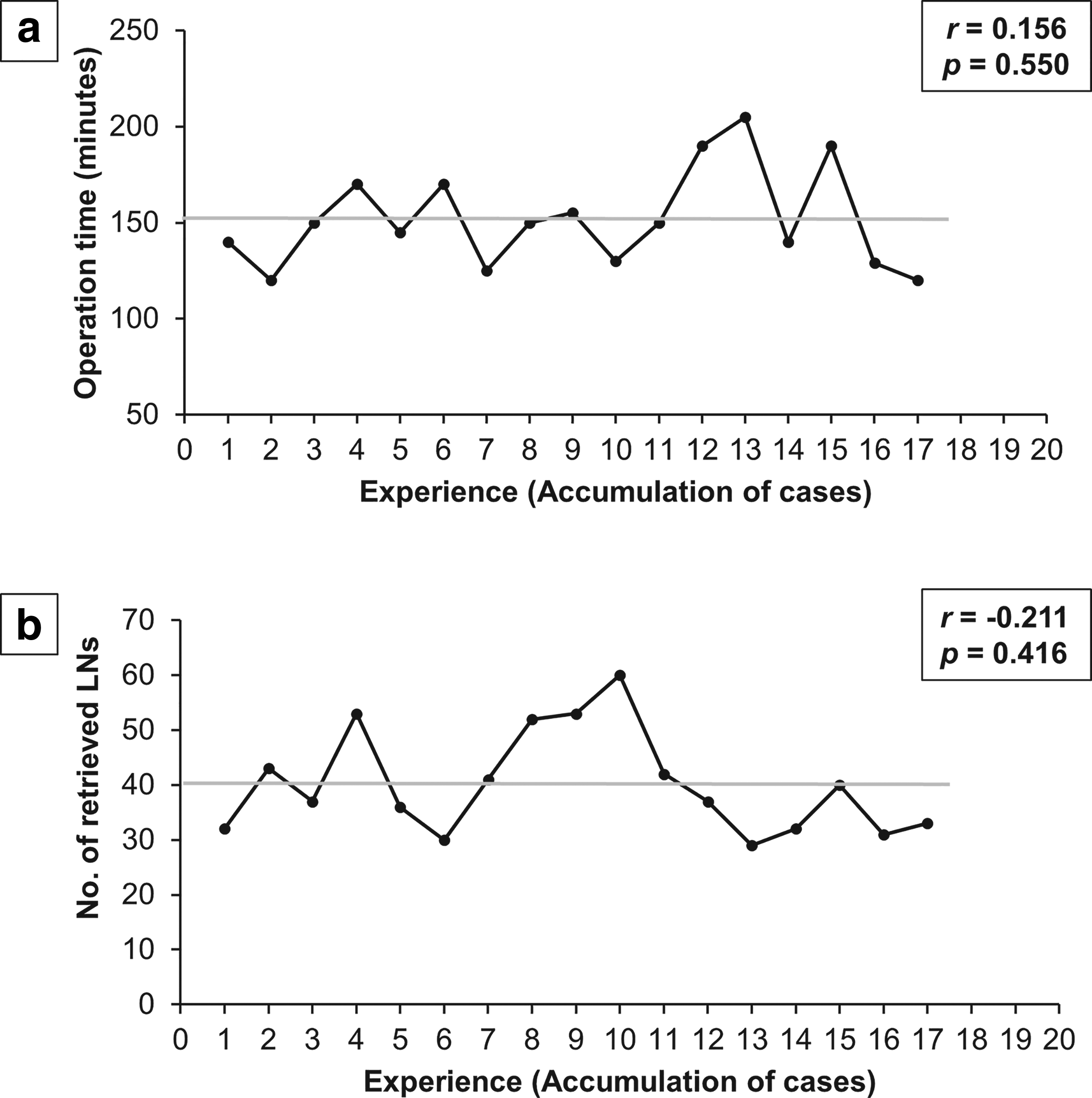
Learning curves for laparoscopic gastrectomy using instruments with minimal diameter.
Discussion
We successfully performed laparoscopic subtotal gastrectomy using instruments with a minimal diameter without conversion to conventional laparoscopy surgery. We identified that the short-term surgical outcomes were comparable to conventional laparoscopic subtotal gastrectomy for EGC. Moreover, we examined that these procedures for gastric cancer did not require a specific learning curve in the experienced surgeon because the operation time and number of retrieved LNs were almost steady according to the accumulation of experiences.
The major limitation of single- or reduced-port laparoscopic surgery for gastric cancer is the required learning curve even in experienced surgeons.12,18,19 However, in the present study, we showed that there was no significant correlation between the accumulation of experiences, the operation time, and the number of retrieved LNs. In cases of single-port gastrectomy, it is technically challenging for surgeons to perform complex procedures through single-port access due to instrument crowding and loss of triangulation.
On the other hand, the use of instruments with minimal diameter was not significantly different from conventional surgery in terms of the trocar number and instrument triangulation. Instruments with a less than 5-mm diameter have not been popularly used in laparoscopic surgery since they are not rigid enough to need to lift intra-abdominal organs. Recently, instruments with a minimal diameter were developed with more grasping power and stiffness compared to conventional laparoscopic instruments. Therefore, the surgeons familiar with conventional laparoscopic gastrectomy can apply laparoscopic gastrectomy using instruments with a minimal diameter without a specific learning curve.
A trocar site hernia is one of the incision-related complications in laparoscopic surgery. Its incidence has been shown to be 0.74% to 1.47% after gastrointestinal operations, 20 and it is commonly seen in trocar sites with a diameter of 10 mm or more. 21 Therefore, a wound of 10-mm or more trocar site should be closed in a layer-by-layer fashion including the fascia, but it can lead to inevitable postoperative pain due to the tension following with fascia closure. In laparoscopic gastric cancer surgery, although it is impossible to skip the mini-laparotomy for specimen extraction, we can at least replace the trocar site using a 10-mm or larger with a 5-mm or smaller instrument to minimize the chance of fascia closure.
However, gastric cancer surgery requires 10-mm instruments like linear staplers and 10-mm clips in gastric resection, vessel ligations, and reconstruction. In the present study, a mini-laparotomy was performed in the early phase of the operation to place the wound protector using multi-ports including a 12-mm trocar to insert the instruments with a diameter of 10-mm or more. All other procedures were practicable without more 10-mm diameters and incisions.
The use of instruments with a minimal diameter arises as a good alternative to minimize the incision site and surgical invasiveness. A key strategy of laparoscopic surgery is an improvement of postoperative recovery by minimizing abdominal wall trauma. Using a half-size trocar results in about one-fourth of the tension on the trocar site. 22 In this context, the use of instruments with a minimal diameter is a natural evolutionary movement of laparoscopic surgery.
However, we observed no difference in postoperative recovery in our study despite the use of instruments with minimal diameter except for immediate inflammatory reaction (the ratio of neutrophil count at the POD 2). Most likely, those analogous results in terms of the postoperative course were caused by small sample size. Several studies that evaluated different types of surgery have shown that laparoscopic surgery using instruments with minimal diameter is associated with a significant reduction in the perceived postoperative pain and hospital stay.23,24 Therefore, a prospective comparative trial would be needed to clarify whether postoperative recovery improves after using these instruments in laparoscopic gastrectomy for gastric cancers.
In addition, as laparoscopic surgery using instruments with a minimal diameter falls within the category of minimally invasive surgery, differences in overall morbidity compared with conventional laparoscopy might be so exiguous. This study also showed that the overall morbidity was comparable between the two groups. However, we identified no perioperative complications in the experimental group, which could represent a promising result.
This study has several limitations. First, the sample size is relatively small compared with other organ surgery studies and we cannot exclude potential selection bias because of the retrospective noncontrolled nature of this study, although the demographics of patients were similar between the two groups. If more patients with laparoscopic gastrectomy using minimal-sized instruments were included in our study, it might be better to define differences in the complication rates and recovery from surgery. Second, we evaluated only the overall pain scale for postoperative pain. An accurate assessment for subjective outcomes of postoperative pain is required to determine the differences in postoperative pain, such as comparison of pain scores for each trocar site, time-serial pattern, or the total amount of analgesics used. Third, we have been able to perform laparoscopic gastrectomy using instruments with minimal diameter for patients with a body mass index of 30.6 kg/m2; however, their use in obese patients above class 1 might be arduous due to improved but still limited stiffness of instruments with a minimal diameter. Advances of the instruments with a minimal diameter including energy devices and surgical staplers would enable the mini-laparoscopic gastrectomy for all patients.
In conclusion, laparoscopic gastrectomy using instruments with minimal diameter is considered a technically feasible and safe procedure and could be a practicable alternative to conventional laparoscopic gastrectomy for the treatment of EGC for experienced surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant from the National R & D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (1320270).