
Abstract
Background:
Laparoscopy is widely accepted for the surgical treatment of benign ovarian lesions in adult women, with results similar to an open approach when spillage is avoided by different means such as endobag retrieval. This approach is controversial in children.
Materials and Methods:
Retrospective study (2009–2018) of all pediatric ovarian tumors with histological confirmation treated in a tertiary center. Data regarding preoperative selection criteria, surgical technique, and follow-up were registered. Laparoscopy was used only in tumors without malignant features and whose size allowed retrieving them through a small incision without morcellating. Emphasis was set in ovarian sparing surgery (OSS), comparing the results of open (OP) and laparoscopic (LPC) approach.
Results:
During the study period, 48 suspicious lesions in 45 patients were operated. Thirty cases (32 tumors) showed benign features (10 cystadenomas, 14 mature teratomas, 6 nontumor lesions); treatment consisted in oophorectomy in 13 (OP 6, LPC 7) and OSS in 17 (OP 5, LPC 12). There was one conversion in the LPC group. Mean follow-up was 3.44 years (range 0.03–8.84), based on annual ultrasound (US) and tumor markers during at least 5 years, recommending a lifetime follow-up by a gynecologist. There was only one relapse in a laparoscopically enucleated cystadenoma, and 2 patients developed contralateral metacronous teratomas. No procedure-related complications happened.
Conclusions:
Our series, although small and with a limited follow-up, suggest that laparoscopy could be an option of treatment in a subset of highly selected patients, although laparotomy remains the gold standard approach if malignancy is suspected.
Background
Ovarian tumors represent only 1% of all tumors in pediatric age. 1 In addition, more than 85% of these are benign, being mature teratomas the most frequently encountered ovarian masses. 2 Traditionally, surgical treatment involved salpingo-oophorectomy of the affected side, 3 decreasing ovarian tissue reserve. It is also remarkable that in up to 12% of cases, both ovaries can be affected. 4 Due to concerns in long-term ovarian reserve and possibility of development of metacronous contralateral lesions, during the last decade ovarian-sparing surgery (OSS) has become the recommended approach for benign ovarian masses in girls, with excellent results in terms of ovarian function and few local relapses. 5 Most pediatric authors favor an open approach, based on the difficulty of laparoscopic handling of large tumors and concerns about possible rupture and spillage of these benign tumors with an otherwise excellent prognosis. 6 In adult women, laparoscopic OSS with gonadal preservation has gained popularity as a safe method for benign tumor removal,4,7 with large series of patients published. In the pediatric literature, since the first published series, 8 a few reports and case series using a similar laparoscopic approach have emerged during the last years. However, preoperative assessment of the benign/malignant nature can be difficult in some cases.9,10 The aim of the present study is to describe our recent experience in the surgical treatment of ovarian adnexal masses in children, focusing on the results of the laparoscopic approach, in terms of feasibility, safety, and midterm outcomes, and to discuss our patient-selection criteria.
Materials and Methods
Retrospective review of clinical records over a 10-year period (January 2009–December 2018) of all pediatric patients with ovarian tumors treated in a pediatric oncology tertiary center. Patients with malignant tumors were excluded for analysis. From the benign tumor subgroup, data regarding demographics, symptoms, preoperative workup, surgical technique, and follow-up were registered.
Patients with preoperative suspicion of ovarian torsion or acute abdomen were operated on an emergency basis, with the surgical approach chosen by the physician on call. Laparoscopic oophorectomy was performed exceptionally in emergency surgeries when long evolution ovarian torsion was present, and image features were clearly of benign lesions. Otherwise, patients were admitted to hospital, and diagnostic tests were completed to decide the most suitable surgical approach.
OSSs were performed only as elective procedures, after appropriate preoperative studies, selecting tumors with clearly benign features, specifically, normal serum tumor markers (alpha-fetoprotein, β-hCG, CEA, CA-125, inhibin-B, and LDH) and absence of malignant traits on preoperative image studies (tumor characteristics, diameter of solid component ≥8 cm, invasiveness, pathologic lymphadenopathies, distant metastasis). Tumor size was recorded as the largest diameter noted on preoperative imaging. All OSS, both open and laparoscopic, were performed by two surgeons of the pediatric surgical oncology unit, following the same criteria and technique.
Surgical approach was categorized as laparoscopy (LPC) or open (OP), and surgical procedure as ovarian-sparing tumor surgery or oophorectomy. A clear and safe dissection plane between the healthy parenchyma and tumor tissue was indispensable during intraoperative decision-making to proceed with organ-saving surgery. Occasionally, controlled drainage of the largest cysts was performed to allow a safer and less mutilating surgery.
A Pfannenstiel was the preferred incision used for laparotomy in elective procedures. Laparoscopic surgery was considered for cystic lesions and solid tumors measuring 5 cm or less, as larger solid lesions would need a conventional Pfannenstiel incision for tumor extraction without morcellation.
Laparoscopic approach was performed with three ports; a 10-mm umbilical port for the camera and retrieval of the lesion and two 5 mm working ports in the right and left iliac fossae. An initial exploration of the abdomen was first undertaken to confirm the diagnosis, exclude malignancy, and inspect the contralateral ovary. Peritoneal fluid from the Douglas cavity was obtained for cytological examination. The affected ovary was stabilized inside a sterile plastic bag (Fig. 1A), and a superficial incision of the ovarian cortex was made with diathermy near the tumor limits (Fig. 1B). The incision was gently enlarged by blunt and sharp dissection to locate the cleavage plane between the tumor wall and the ovarian cortex, followed by excision of the cyst inside the bag (Fig. 1C). Cautious bipolar coagulation was used to achieve hemostasis. After removing the specimen, the ovarian capsule was left unsutured in most cases. The 10 mm umbilical incision was extended as needed to allow smooth passage of the specimen inside the bag, avoiding morcellation and therefore accidental spilling. Postoperative follow-up was carried on by physical examination, pelvic ultrasound (US) 6 months after surgery, then annual US, and tumor markers during at least 5 years. A lifetime follow-up by a gynecologist was recommended. Patients were deemed lost to follow-up if there was no information available following postoperative care.
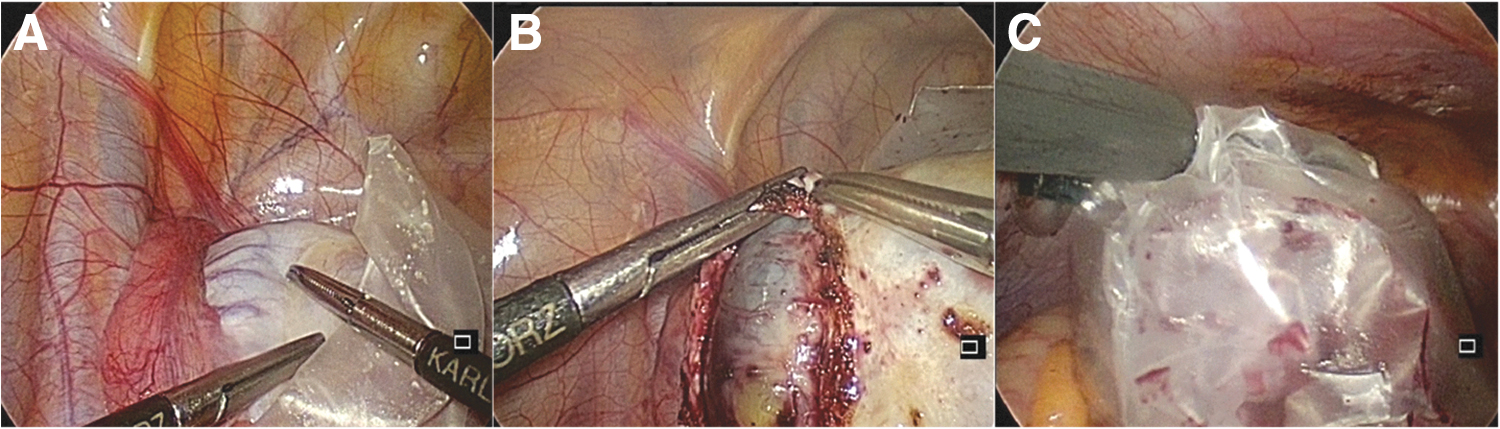
Laparoscopic OSS, surgical details. The affected ovary is placed inside a sterile bag
Statistical analyses were performed with the Stata software (Stata 13.0; StataCorp LP, Texas). Nonparametric tests were used (Mann–Whitney U test) due to the characteristics of the sample (nonnormal distribution). Statistical significance was assigned to P < .05.
Results
Forty-eight suspicious lesions in 45 patients were operated during the study period. Of these, 32 tumors (66.7%) in 30 patients presented benign characteristics in the preoperative workup, being the focus of our study (Fig. 2).
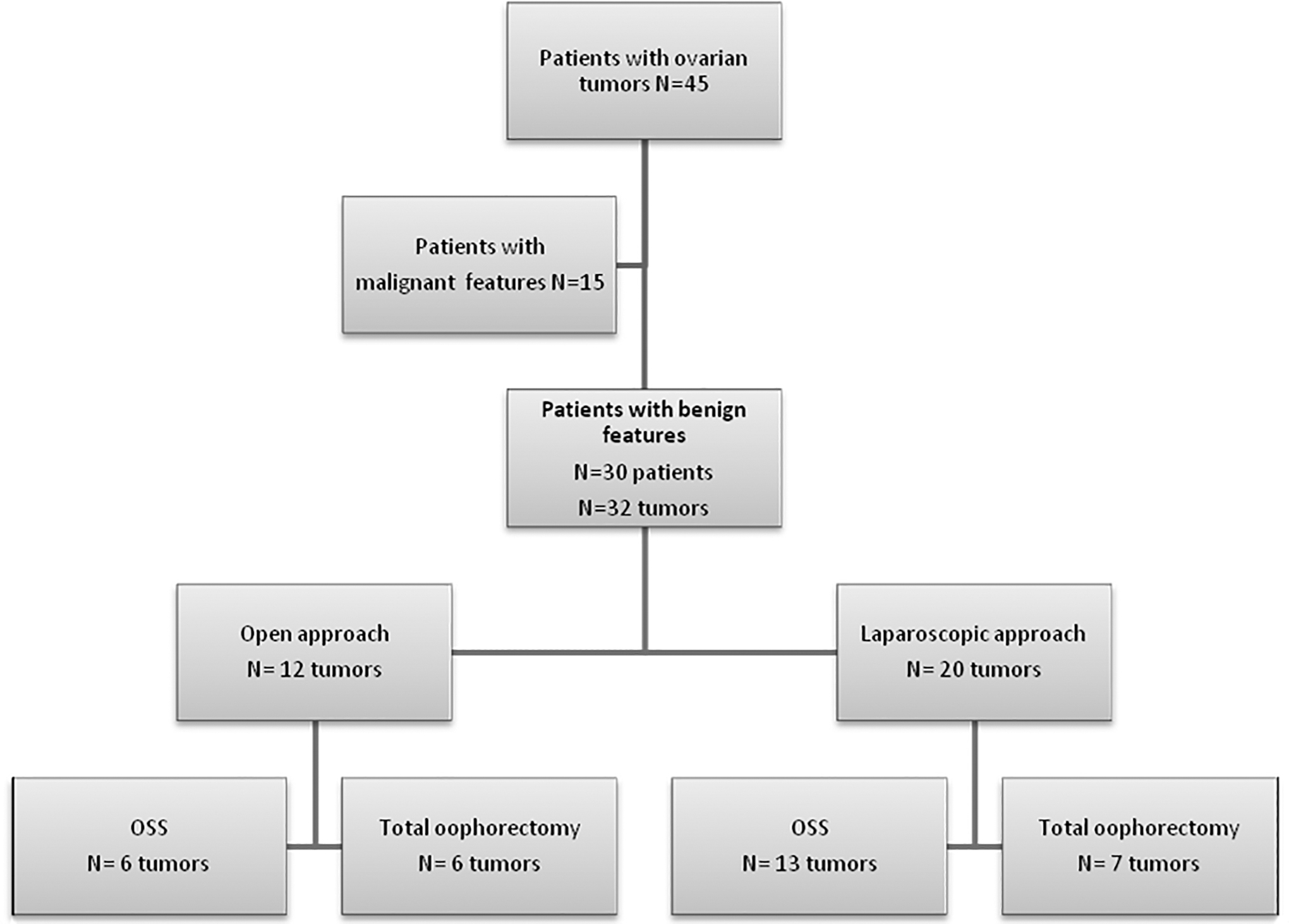
Patients' flowchart.
Patients mean age in the benign subgroup was 10.6 years (range 0–16.9) compared to 11.3 years (range 1.3–15.9) in the malignant subgroup. Final histological examination of this group confirmed a total of 25 benign tumors in 24 patients (14 teratomas and 11 cystadenomas, including 1 bilateral case) and 7 nontumor lesions in 6 patients (2 evolved torsions, 2 giant follicular cysts, 3 endometriosis, and 1 case with bilateral involvement). Their characteristics are summarized in Table 1.
Patients' Demographics and Characteristics
Only ovarian-sparing surgery cases were included.
MRI, magnetic resonance image; US, ultrasound.
Following the recommendations of the main pediatric oncology collaborative groups (Childrens' Oncology Group, International Society of Paediatric Oncology), we do not perform laparoscopic resection for malignant ovarian tumors, so those cases were not analyzed.
Mean age at surgery was 10.78 ± 5.07 (range 0.53–17.47) years. The chief presenting complaint was chronic nonspecific abdominal pain in 15 patients (50%) followed by progressive abdominal distension in 7 (23.3%).
Ultrasonography was performed in all patients but one. In addition, MRI or CT was performed in 20 patients (especially if laparoscopic OSS was the proposed approach). Interestingly, in one malignant case, MRI identified a bilateral lesion that was missed on US and since then, preoperative MRI became our common practice. Two patients suffered from bilateral involvement at the time of diagnosis, and 2 other patients developed metacronous teratomas during follow-up after initial surgery.
Tumor markers were preoperatively measured in 28 patients (93.3%). Mean diameter of adnexal masses from radiological imaging was 11.02 ± 8.66 cm (ranging from 1.9 to 37 cm).
OSS was performed in 17 cases (56.7%), 5 through OP surgery and 12 LPC. The remaining thirteen were treated with oophorectomy (OP 6, LPC 7), including 8 ovarian torsions (6 during the first years of our study and 2 congenital ovarian torsions), large tumors with solid component >8 cm, doubtful tumor markers (mildly elevated alpha-fetoprotein or CA-125), and atypical findings or unconclusive on image studies, or certain diagnoses such as one case of endometriosis with no evident ovarian tissue. Patients who underwent open approach presented statistically significant larger tumors than the laparoscopic group (mean 16.76 cm versus 6.78 cm). There was one conversion to open surgery in the laparoscopic group due to an endometriosis firmly attached to all the surrounding structures. There were no procedure-related complications (including tumor rupture) and only one postoperative complication happened, in the OS group; a bleeding from the mesocolon in a patient with a portal hypertension and bilateral endometriosis.
Histological examination revealed mature teratomas in 14 ovaries, cystadenomas in 11 (1 bilateral case), and nontumor lesions in 7 (1 bilateral case).
Median follow-up for the entire cohort was 3.44 years (range 0.03–8.84 years), 2.82 years (0.59–4.41) for the open OSS subgroup and 3.61 (1.28–8.07) for the laparoscopic OSS subgroup. Two patients were lost to follow-up within the first postoperative year. During our study period, there was only one relapse in one ovary, in a patient from the LPC group with large bilateral cystadenomas, 1 year after surgery. She underwent an uneventful ovarian-sparing re-resection through a Pfannenstiel incision.
Two patients developed contralateral metacronous teratomas 1.5 and 5 years after surgery; ovarian-sparing resection was performed in both cases (one by OP approach and one LPC).
All enucleated patients maintain bilateral ovarian parenchyma on US, being the healthy ovary/affected ovary ratio 1.41 ± 0.63 in the OP group and 1.2 ± 0.27 in the LPC group (P > .05).
Discussion
Approximately, half of all ovarian lesions in children and adolescents are not neoplastic 1 ; ovarian tumors are distributed approximately into germ cell tumors (80%), stromal or sex-cord tumors (15%), and epithelial tumors (15%). Among germ-cell tumors, 95% of cases correspond to benign mature teratomas 11 and, regarding epithelial lesions, the majority are benign cystadenomas.
Benign and malignant tumors are difficult to differentiate based only on initial clinical findings, making thorough preoperative studies essential. 12 Common symptoms at diagnosis for both benign and malignant lesions are palpable abdominal mass, pelvic pain, or clinical findings of acute complications, such as torsion or rupture.
In a British retrospective case-note study published in 2010 by Hernon et al., preoperative tumor markers were obtained in only 10% out of 155 cases of pediatric ovarian cysts and tumors, highlighting the lack of adequate preoperative assessment in this age group. 13 This is determinant for accurate and safe surgical decision-making. Preoperative assessment of tumor markers (AFP, B-hCG, CA-125, CEA, LDH, and inhibin B) should be mandatory in an elective surgery basis, especially if an ovarian-sparing resection is to be performed. In case of precocious puberty, hormonal levels must be included in the preoperative workup. First-line radiologic diagnostic method is pelvic ultrasonography, which evaluates the localization, size, and characteristics of the lesion. Abdominal MRI, in our experience, is a very valuable tool when ovarian-sparing procedures are planned, helping to assess tumor location into the ovary, expected remaining healthy tissue and possible bilateral disease, and should always be performed if malignancy is suspected.
Classically, treatment for ovarian lesions was oophorectomy either through an open or laparoscopic approach. During the last decades, given the excellent results in terms of cure and survival of benign ovarian tumors in children, focus has been set on long-term sequelae, particularly in cosmetic results and ovarian reserve. Ovarian reserve has been defined as the reproductive potential of the patient at a certain point in time. 14 Conservative ovarian surgery in childhood and adolescence is therefore important for the development of normal puberty and future fertility. 15
Since the first reports in the 90's 16 laparoscopic OSS has become the preferred approach for benign ovarian cysts in adult women, providing both the benefits of a minimal invasive approach and parenchyma sparing resections. 14 However, even this conservative management has been proved to reduce the ovarian reserve at some degree, having identified some factors related to this damage, such as tumor size and burden (bilaterality), histology, surgical technique (tissue handling), and hemostatic methods (electrocoagulation). 13 Regarding laparoscopic OSSs, some adult reports have even stated that a minimal invasive approach provides a better preservation of healthy ovarian tissue, when compared to open surgery,17,18 but we found no statistical significance favoring an open or laparoscopic approach; however, this is a small series.
Laparoscopic ovarian-sparing tumorectomy is increasingly being performed in children and adolescents during recent years, but has not become the standard of care. There is a logical concern regarding risk of tumor rupture, especially if a malignant lesion is inadvertently treated as a benign one. This is of particular interest for granulosa-theca tumors, whose prognosis is dismal in case of local spillage. Nevertheless, there seems to be increasing evidence favoring this approach. Karpelowsky et al. published in 2009, one of the first series, 19 followed by Chabaud-Williamson in 201111 and more recently by Abbas et al. in 2016. 5 This proves an increasing interest on this approach, which apparently provides similar results to open surgery when patients are correctly selected and surgical technique is focused on preventing complications.
The importance of prevention of rupture and spillage risk is always mentioned.20,21 In our experience, results are comparable to an open approach when spillage is avoided by different means such as delicate handling of tissues, performing tumor resection inside a sterile plastic bag and bagged retrieval. Our selection criteria proved to be adequate, as there was no conversion in the LPC group, surgeries could be completed successfully, there were no complications (tumor ruptures, bleeding…) and only one patient relapsed locally.
In our series, one selection criteria for laparoscopic approach was solid tumor size around 5 cm, which is consistent with the literature 22 ; probably, this is a practical matter, as bigger solid lesions require a Pfannenstiel incision for extraction, making laparoscopic approach of lesser interest.
Benign tumors in the subset of ovarian torsion deserve a special comment. Despite our practice during the study period has been to perform oophorectomy (through an open or minimal invasive approach), this would be a suboptimal management. In light of growing evidence, the most accurate attitude would be to perform an exploratory laparoscopy, to detorse the ovary (even with severe ischemic damage), and to complete further studies. Then, during a second surgery, an OSS could be safely performed with guarantees if indicated. 23 When findings during laparoscopy suggest a clearly malignant appearance (which happens in only 1.8% of all pediatric ovarian torsions), 24 an open oophorectomy could be performed if oncological principles are strictly followed.
Conclusions
Our small series comes to support growing evidence suggesting that laparoscopy could be a safe option of treatment in a subset of highly selected pediatric patients, as long as oncological principles are maintained. Preoperative assessment with detailed tumor markers and diagnostic image (to evaluate tumor characteristics and to select lesions under 5–6 cm) has provided us a 100% success in terms of identification of benign lesions and laparoscopic feasibility.
Despite improved results in terms of ovarian reserve with parenchyma-sparing techniques, patients should be informed of possible long-term implications in fertility, as literature from adult women seems to confirm.
Efforts should be implemented to assure safe resections, maybe including techniques such as ultrasound-guided laparoscopic resections, to our pediatric surgeons' practice. Multicentric prospective studies with longer follow-up would be desirable to confirm our findings.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.