
Abstract
Background:
Slipping rib syndrome (SRS) is an often underdiagnosed cause of lower chest wall and abdominal pain. The diagnosis of SRS is established by physical examination with or without dynamic ultrasound. The pain can be debilitating and surgical excision of the nonattached, subluxing cartilages is curative for most patients, but frustratingly, up to a quarter of patients have transient or limited relief and require reoperation. Some of these patients were found to have subluxation of the remaining bony ribs, suggesting that excision of rib cartilage alone may not be curative in a subset of patients.
Materials and Methods:
A retrospective review was performed of 3 patients with recurrent slipping rib pain and hypermobile bony ribs on reoperation. In an effort to stabilize the hypermobile ribs, vertical bioabsorbable plating across their ribs was performed. The plates secure the ribs apart from each other, preventing the movement of ribs against each other and therefore the pain.
Results:
All patients tolerated the procedure well. Mean length of stay was 2.6 days. Mean follow-up is 7 months and all report significant improvement in pain.
Conclusions:
Rib plating allows stabilization of hypermobile ribs, while preserving the patient's anatomical rib cage, and is a safe treatment for recurrent pain after the initial procedure. This is a novel approach in patients with recurrent slipping rib symptoms.
Introduction
Slipping rib syndrome (SRS) is an underdiagnosed cause of upper abdominal/lower chest wall pain. Pain occurs when the false cartilages (ribs 8 through 10) are not attached to each other by their usual cartilaginous attachments and therefore are able to slide underneath the adjacent cartilage or rib. This subluxation irritates the intercostal nerve and can cause debilitating pain. Diagnosis is based primarily on clinical suspicion, followed by physical examination and dynamic ultrasound.1–5 Once the diagnosis is made, depending on the pain and its physical limitations, the standard therapeutic options include observation, paravertebral or intercostal nerve injections, or surgery to remove the rib cartilages. 3 This operation has been reported to be successful for almost 100 years. 1 However, a frustrating challenge for surgeons is recurrent pain following cartilage resection, and some surgeons have removed the bony rib suspecting the rib itself to be inciting pain. Our experience mirrors the literature in which ∼26% of patients require reoperation. 6 To decrease the incidence of recurrence, we present a new technique to stabilize the cartilages and ribs, recreating a stable costal margin.
Materials and Methods
Following IRB approval (#19–263), a retrospective case review was performed of all patients who underwent bioabsorbable plating (Poly-L/DL Lactide 70:30 blend; BioBridge™, Acute Innovations, Hillsboro, Oregon) for recurrent symptoms after surgery for SRS. Demographic data and preoperative, operative, and postoperative variables were collected from charts. Dynamic ultrasound results of the patients were reviewed, as well as any other radiologic study. Pain clinic data were also reviewed.
The description of the procedure
After determining the sites based on physical examination and ultrasound findings, an incision was made at the previous lower costal scar and dissection performed to expose the chest wall. Ribs that moved either over or under the adjacent ribs were at risk for inciting pain and the decision was made to proceed with plating with bioabsorbable plates. Any excess scar tissue at the medial portions of the bone was removed without injuring surrounding structures or intercostal bundle if present.
The bony portion of a nonslipping rib was identified for anchoring the plate. This anchoring rib is often the one superior to the most cephalad previously resected rib. For example, if the ninth cartilage is the highest one removed, the eighth would be the anchoring rib for plating. Bioabsorbable plates are malleable when placed in a warm saline bath at 140° Fahrenheit. The plate is then shaped to the curve of the ribs, measured to the appropriate length, and cut (Fig. 1). Two nonabsorbable sutures are placed through each rib and then through the holes in the plate. Once all rib sutures were placed, the plate is then parachuted down onto the ribs and the sutures tied sequentially (Fig. 2). Once the plate is secure, the ribs are not able to move independently toward each other, thus securing the costal margin (Fig. 3).
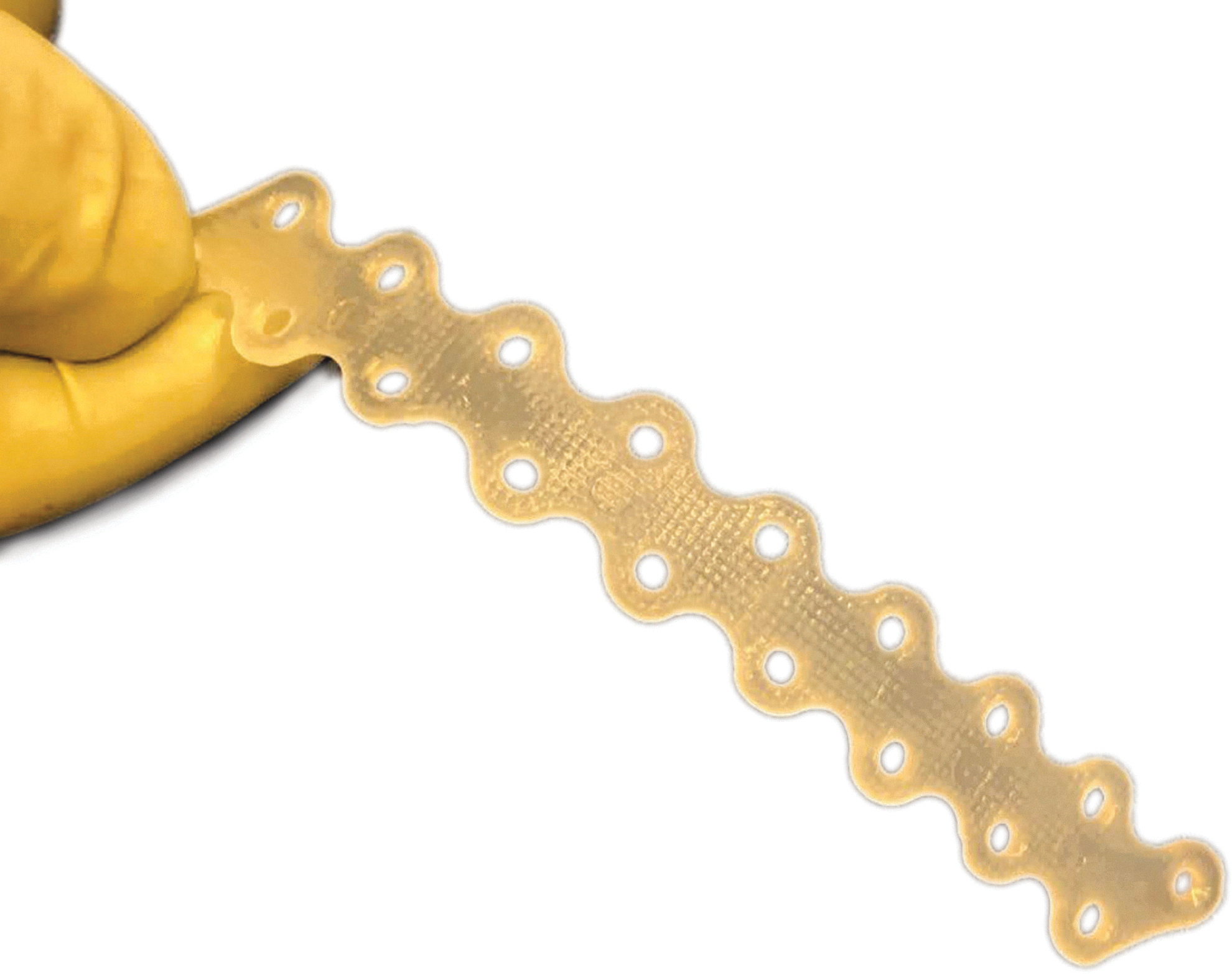
The bioabsorbable plate is easily bent in a hot-water bath and matched to the chest wall and ribs.
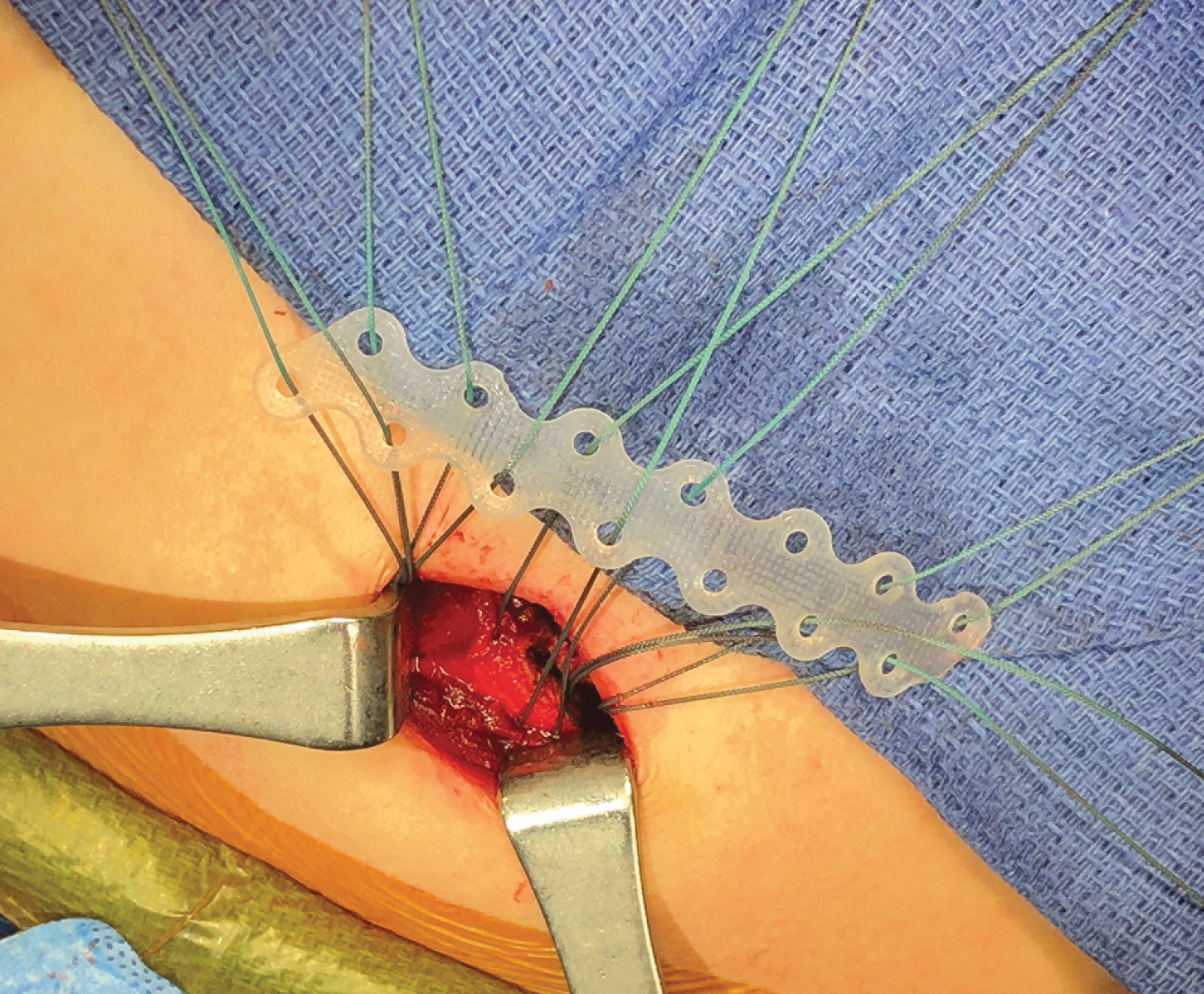
After determining which ribs are hypermobile, the bioabsorbable plate is shaped to the chest wall and measured in situ. Two nonabsorbable sutures are placed through each rib and then through the corresponding holes on the plate. This is then placed into the incision and the sutures are secured.
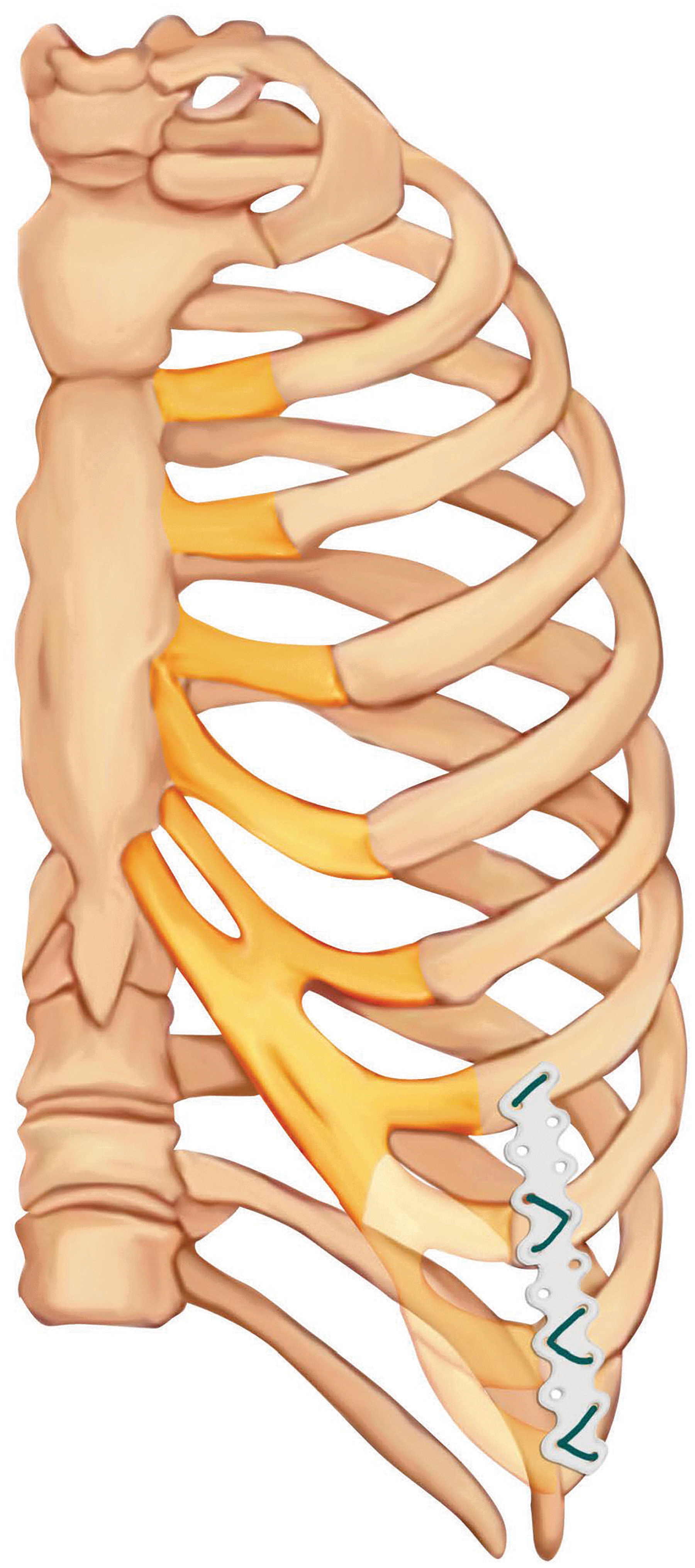
The 8–10th costal cartilages have been removed and the bioabsorbable plate is secured to the 7–10th ribs with sutures, creating a “neocostal margin.” Illustration by Mogumash, 2019.
Results
Three patients were identified, who met criteria in the study timeframe. See Table 1 for demographics and findings. Mean length of stay after plating was 2.6 days (2–3 days). There were no wound infections or surgical complications. All patients underwent physical therapy for 6 weeks after their 2 week follow-up visit for strength and flexibility training. Mean follow-up was 7 months (3–10 months) and all 3 patients are significantly improved.
Operations Performed
L, left, R, right, B, bilateral.
Patient descriptions
Patient 1 is an 18-year-old female volleyball player, who initially presented at age 14 with debilitating left-sided pain. Her SRS was initially diagnosed by hooking maneuver on physical examination. She underwent excision of the left 9th and 10th costal cartilages, leaving the perichondrium intact (as was common early in our experience). She had relief for 1 year and then complained of recurrent pain. She was found to have regrowth of her 9th and 10th costal cartilages as well as increased mobility of her 8th costal cartilages. The rib cartilages were then excised in their entirety to the level of the bony rib. She did well again with relief for a year, but felt recurrent pain with a clicking sensation. This pain was at a point of tenderness, which corresponded with her ninth rib at a point that it flared out. A 2-inch segment of the ninth rib was removed at this operation, as well as a 0.5-inch segment of the eighth. Sixteen months later, her pain recurred and an ultrasound revealed an area of scar tissue with possible neuroma in the area of point tenderness she felt on the left. She was evaluated by pain anesthesia and underwent multiple injections to the direct area with only temporary relief. She continued to have a sensation of movement exacerbating the pain on the left. She was seen in the complex pain program clinic, elected to undergo re-exploration, and was found to have scar tissue and a very flexible ninth bony rib. A 17-hole bioabsorbable plate was custom-bent to lay vertically in an anatomic position across the lateral bony sections of her 8th, 9th, and 10th ribs, and was affixed with multiple nonabsorbable sutures. She has been pain free for 9 months since her last operation.
Patient 2 is a 13-year-old gymnast with severe left-sided SRS. At age 11, she sought care and her pain was reproducible with palpation of her hypermobile lower costal cartilages. She underwent rib blocks that demonstrated relief at the 8th, 9th, and 10th cartilages. Due to her persistent symptoms, she was taken to the operating room and was found to have slipping cartilages at the same levels, and these were excised to the bony rib. Her pain resolved on this side, yet 3 months later, she developed severe, acute pain on the right side. On clinical examination, a hook maneuver, replicated her pain. Her 9th and 10th cartilages were found to be overlapping and slipping without fixation, and were excised to the bony rib. Her recovery from a surgical standpoint with pain was excellent, but she developed a diagnosis of postural orthostatic tachycardia syndrome (POTS). She saw multiple physicians for this and was ultimately treated with antihistamines. She fell down the stairs 4 months after the second surgery and suffered recurrent pain on the left, and was evaluated by the complex pain clinic for possible interventions. Two months later, she underwent dynamic ultrasound that demonstrated her left eighth costal cartilage was slipping on the seventh, reproducing pain. Thirteen months later, after her POTS stabilized, she was found to have flexible bony ribs at eighth to ninth cartilages as well as movement at the articulation at the junction of the seventh and eighth cartilages, and underwent bioabsorbable rib plating of her seventh through ninth cartilages laterally and her seventh and eighth cartilages medially, fixing the site that was palpably moving. She tolerated the procedure well and recovered nicely after without any exacerbation of her POTS symptoms. Follow-up was 3 months.
Patient 3 was initially seen at age 16 years by an outside pediatric surgeon. This 16-year-old female soccer player presented with symptoms of bilateral slipping ribs for over 2 years. Primary symptoms were upper abdominal/lower chest wall pain related to activity and accompanied by a clicking sensation. The examination documented tenderness of the 9th through 11th ribs and the surgeon was able to elicit a clicking sensation with movement. She had undergone a costal block that provided transient relief. She underwent excision of bilateral 10th and 11th slipping rib cartilages and initially, her pain improved. She then had a laparoscopic appendectomy for acute appendicitis and the same rib pain recurred 4 months later. She did not tolerate gabapentin due to side effects and lidocaine patches had no effect. On physical examination, the ninth ribs seemed to slip beneath the costal margin, bilaterally. Excision of a 3-inch segment of bone from both ninth ribs was performed with good relief for 10 months. The pain returned without a clicking sensation and was described to be tenderness over the rib ends. A computed tomography scan was performed and no bony overgrowth or malposition was found.
She was then referred to me by her initial surgeon with continued discomfort after two prior operations. She described her pain as sharp and dull, radiating across her abdomen. She had not been to school for 3 weeks because of the pain and was on hydrocodone once daily for pain management. On physical examination, there was tenderness at the bilateral 8th and 9th ribs with the 9th rib on the left immediately adjacent to and abutting the 8th; the 10th ribs were unattached bilaterally. She was referred to our complex pain clinic and underwent bilateral intercostal nerve blocks at ribs 9, 10, and 11 with excellent temporary relief. She was advised to start physical therapy, use a transcutaneous electrical nerve stimulation (TENS) unit, alternate ice and heat, and alternate acetaminophen and NSAIDS. She was also instructed to establish care with psychology for cognitive behavioral therapy. One month later, she went to surgery. There, scar tissue was excised and bilateral eighth and ninth ribs were found to be hypermobile, moving easily against each other. A bioabsorbable plate was used to attach the 7th through 10th ribs vertically, which fixed the ribs in their natural anatomic state without allowing subluxation or abnormal contact. She has been pain free and off narcotics completely at the 8-month follow-up.
Discussion
Due to the high rate of recurrent pain, SRS can be a difficult problem for the surgeon as well as the patient. A common finding in patients with recurrent pain after surgery for slipping rib is persistent excessive movement or subluxation of the remaining rib or ribs, often lateral to the prior cartilage resection. While it is clear that a mechanical reason exists for the pain, it is unclear how much of the rib is actually inciting the pain. Historically, all of the cartilaginous portion of the rib, and occasionally, some of the bony rib have been removed. Although the rib cartilages provide no structural support or protection when they are not attached, and even cause pain, the bony ribs likely do provide some protection and removing them may not be in the patient's best interest. Securing the hyperflexible ribs apart from each other, in a way that mimics a neocostal margin, prevents the movement of the ribs against each other, decreases the sensation of slipping, and alleviates the resultant pain.
The choice of a bioabsorbable plate has some clear advantages in this particular application. It is safe and has been used in multiple chest wall procedures.7,8 It is easily molded to the appropriate shape by placing it in a warm bath (140°) and is easily secured to cartilage and bone with sutures. Unlike most metal rib plates, the bioabsorbable plates are initially flat with a low profile and can be placed vertically without creating a visible ridge. The holes are well suited for suture fixation, thus avoiding the use screws in an area of high movement. The nonmetallic plates are far more resistant to fatigue than titanium plates, as titanium chest wall plates have been associated with failures. 9 The bioabsorbable plate lasts for 18 to 24 months, leaving scar tissue in its place, keeping the ribs separated. 10
There are obvious limitations to this series. There are only 3 patients in this report and the mean follow-up is short at 7 months. There is a selection bias, in that only patients with recurrent pain were treated. In addition, the incidence of recurrent pain after 2 years once the bars resorb completely is not yet known.
Recurrent pain in SRS is frustrating for the patient and physician alike. A multidisciplinary approach, including pain service, psychology, and physical therapy working along with the surgeon, is important to achieve a good outcome. Based on the operative findings of these patients, persistent rib subluxation after cartilage resection appears to be a common finding after failed surgery for SRS. Bioabsorbable plating is a safe method of fixing the hypermobile rib cage in patients with recurrent SRS. This is the first report of using bioabsorbable plating in children for recurrent SRS.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.