
Abstract
Background:
The purpose of this research was to investigate the feasibility and strategies of right central lymph node dissection (CLND) in endoscopic thyroidectomy through chest–breast approach.
Materials and Methods:
Retrospective analysis on the conduction of 68 cases of endoscopic thyroidectomy through chest–breast approach with right side CLND (endoscopic group) and 31 cases of thyroidectomy through low-neck collar cervical approach with right side CLND (open group) from July 2014 to February 2019. The intraoperative and postoperative data were compared between the two groups.
Results:
All the surgeries in open group were successfully completed as well as the endoscopic group without any intraoperative conversion into open surgery. There were no difference in sizes of tumor, incidence of lymph node metastasis, number of dissected and metastatic lymph nodes, and postoperative hospitalization days between the two groups. Temporal hypoparathyroidism occurred in both groups with endoscopic group to be 24 cases and open group to be 15 cases but no case in both groups suffering from permanent hypoparathyroidism, recurrent laryngeal nerve injury, lymphatic leakage, or death. One case in endoscopic group was treated with secondary surgery for lateral cervical lymph node metastasis and no evidence of recurrence or metastasis was found in other cases during postoperative follow-up.
Conclusions:
With strict control in surgical indications and contraindications, endoscopic surgery is safe and feasible for selected cases with the same effect as open surgery on dissection of lymph nodes in the right central region, which is in line with the principle of radical treatment of tumors.
Introduction
Endoscopic thyroidectomy, a proven safe and effective method for the thyroid cancer surgery treatment, can also achieve good effect in central lymph node dissection (CLND). Due to the anatomical difference in bilateral recurrent laryngeal nerve (RLN) and the positional relationship difference between central lymph node and RLN, bilateral CLND present various characteristics; CLND in the right side is difficult in endoscopic thyroidectomy through chest–breast approach. In this study, we conduct a retrospective collection on 68 cases of thyroid cancer treated by endoscopic thyroidectomy through chest–breast approach with right side CLND by comparison with open surgery to summarize the feasibility and strategy of right side CLND in endoscopic thyroidectomy through chest–breast approach.
Materials and Methods
Study design and patient status
Collection of clinical data of the thyroid cancer patients with right side CLND was from July 2014 to February 2019 in the thyroid surgery department of the First Affiliated Hospital of Jinan University.
Selection criteria: (1) patient with tumor diameter <3 cm; (2) patient with treatment through endoscopic approach or open surgery, both were through unilateral or bilateral lobectomy with total or near-total thyroidectomy and right CLND; (3) patient having regular postoperative review and the follow-up with full data; and (4) postoperative pathological diagnosis as papillary thyroid carcinoma (PTC).
Exclusion criteria: (1) cases of left CLND treatment at the same surgery; (2) with lymph node dissection in the lateral neck area (Region I, II, III, IV, and V) at the same surgery; (3) preoperative ultrasound or computed tomography (CT) indication of lateral cervical lymph node metastasis (Region I, II, III, IV, and V); (4) secondary surgery, with previous neck surgery or history of other cervical disease; (5) suspected or confirmed local invasion or distant metastasis in preoperation.
Finally, this study covers a total of 99 cases that includes 68 cases in the endoscopic group and 31 cases in the open group with subgroup sets based on the unilateral and bilateral thyroidectomy in each group according to the range of operation. All patients were clearly explained about these two surgical techniques before reoperation and then allowed to choose freely their preferred surgery with written informed consent. Due to the retrospective design, ethics approval was deemed to be exempt by the local Ethics Committee. Comparison and analysis were conducted on the operative time, intraoperative blood loss, postoperative hospitalization days, postoperative complications, and follow-up data (up to May 31, 2019) between the endoscopic group and the open group. The comparison of general data between the two groups is shown in Table 1.
Comparison of General Data Between Endoscopic Group and Open Group
Values are expressed as mean ± standard deviation.
Operative procedure
Operative method of thyroidectomy was as referred to the guidelines of the American Thyroid Association (ATA) 1 and Chinese Thyroid Association (CTA) 2 : (1) The patient with single differentiated thyroid cancer (DTC), located in the right lobe of thyroid gland, primary tumor less than 1 cm, low risk of recurrence and no history of radiation or family history of head or neck as well as without lateral cervical lymph node metastasis or distant metastasis, and no finding of a nodule in the left lobe of the thyroid gland, a right side thyroid lobectomy, isthmus and cone resection were performed. (2) For patient with tumor diameter greater than 1 cm and less than 3 cm, multiple cancer lesions, or with nodules in the left lobe, and head and neck radiation history or family history, a total or near-total thyroidectomy was performed.
The endoscopic group adopts a chest–breast approach. The methods of building the operative space and thyroidectomy were according to the introduction in previous research.3–6 The order of lymph node clearance is first from both sides to the middle and from superior to inferior, starting from the anterior of RLN to the posterior, then the specimen is removed.
Details are as follows: (1) Separate the loose tissue between the trachea and pretracheal fat by clinging to the trachea in front of the trachea after lobectomy, then enter into the anterior tracheal space to lift the pretracheal lymphatic adipose tissue, and move down forward to the rear of the thymus. The gap between the lymphatic adipose tissue and the thymus before the trachea was detached to reveal the innominate artery and the right common carotid artery. (2) Pull the lymphatic adipose tissue to the left to reveal the vascular sheath, and open the visceral fascia from inferior to superior, medial to the carotid sheath until the cricoid cartilage is horizontal. Pay attention to protect the thymus and prevent from damaging the parathyroid blood supply or the parathyroid tissue hidden in the thymus. (3) Start from the lower positioning to expose RLN upward all the way. First clear the superficial lymphatic tissue of the RLN area, and cover gauze strip on the exposed RLN surface to avoid thermal damage from the ultrasonic scalpel. The ultrasonic scalpel detaches the blood vessels around the RLN and separates the gap between the RLN and the trachea, then pulls the RLN to the outward, and from behind, medial, to disassociate the lymph node posterior to the right RLN (LN-prRLN) to the nerve into the larynx. Attention should be paid on the pulling force to protect the cervical sympathetic nerve. At the nerve into the larynx pull the free lymphatic tissue from behind the RLN outward with nerve at the medial for further clearance of LN-prRLN near the larynx and removal of the specimen with the superficial lymph nodes.
Low-neck collar cervical incision was performed in the open group, with consistent lymph node dissection range in the endoscopic group. First, dissect the right side of trachea, then lymph node in front of the trachea.
All the resected specimens were routinely examined in vitro for suspicious parathyroid tissue, and then cut and planted in the left sternocleidomastoid muscle or forearm subcutaneous after being confirmed by intraoperative rapid pathology or intact parathyroid hormone (iPTH) test strip.
Postoperative management and follow-up
For patients who underwent total or near-total thyroidectomy, routine blood test was performed immediately after returning to the ward (about 1 hour after the operation) to check the level of serum calcium and parathyroid hormone with preventive administration of intravenous calcium gluconate, oral calcitriol, or calcium carbonate to prevent numbness and convulsions in hands and feet. The patient with hypoparathyroidism confirmed by blood test should continuously take oral calcitriol and calcium carbonate until the parathyroid function returns to normal.
Oral L-T4 was routinely taken after surgery with periodic review to monitor thyroid function, thyroglobulin (TG), TG antibody, and thyroid ultrasound for double risk assessment according to the risks of recurrence stratification and side effects of thyroid stimulating hormone (TSH) inhibition treatment stratification to maintain the target TSH. According to the 2012 CTA guidelines and Chinese Nuclear Medicine in clinical diagnosis and treatment, 7 131I treatment was selectively performed according to Tumor Node Metastasis (TNM) staging.
Statistics
Chi-square and t-tests were used to compare the difference between the endoscopic group and the open surgery group. Continuous variables were presented as mean (standard deviation) values. A two-tailed P value of <.05 indicated a statistically significant difference for all tests. All analyses were performed with SPSS version 17.0 software (SPSS, Inc., Chicago, IL).
Results
In the endoscopic group, there are 18 cases of right lobectomy and 50 cases of near-total/total thyroidectomy, whereas 6 cases of right lobectomy and 25 cases of near -total/total thyroidectomy in the open group (Table 1). All surgeries were completed successfully without any conversion into open surgery in the endoscopic group. There are no significant differences in the diameter of the resected right lobe thyroid tumor (11.0 ± 6.3 versus 12.2 ± 8.3 mm), incidence of lymph node metastasis (61.76% versus 45.16%), the number of dissected lymph nodes (7.7 ± 5.3 versus 6.8 ± 3.9), number of metastatic lymph nodes (2.0 ± 2.5 versus 1.3 ± 1.7), intraoperative blood loss (2.6 ± 9.1 versus 7.7 ± 19.4 mL), and postoperative hospital stay (6.5 ± 1.2 versus 6.8 ± 1.7 days) between the endoscopic group and open group. Operative time of unilateral thyroidectomy was 179.1 ± 21.4 versus 151.8 ± 39.4 minutes, and bilateral thyroidectomy was 201.6 ± 38.7 versus 183.2 ± 22.9 minutes in both groups.
All the pathological results suggested PTC of the right lobe, among which, 3 cases were combined with hyperthyroidism, 22 cases with nodular goiter, 9 cases with papillary carcinoma of left lobe, and 16 cases with lymphocytic thyroiditis in endoscopic surgery group, whereas 13 cases were combined with nodular goiter, 5 cases with papillary carcinoma of left lobe, and another 3 cases with lymphocytic thyroiditis in open group. The results are as shown in Table 2.
Comparison of Surgical Results Between Laparoscopic and Open Groups
Values are expressed as mean ± standard deviation.
After bilateral near-total/total thyroidectomy surgery, 24 cases (48.0%) had transient hypoparathyroidism in the endoscopic group, and 15 cases (60%) in open surgery group. Although their instant postoperative blood tests showed low parathyroid hormone and/or low calcium, no symptoms of hypocalcemia was found owing to the preventive treatment of calcium supplement and calcitriol. In addition, there was no case of permanent hypoparathyroidism, RLN injury, lymphatic leakage, or death.
All patients were followed up by May 31, 2019 with average follow-up time to be 19.3 ± 14.8 versus 18.2 ± 14.4 months and the median follow-up time to be 15.5 versus 15 months in both groups. The level of the serum parathyroid hormone and calcium returned to normal in all cases of hypoparathyroidism in 6 months of follow-up. There were 26 cases (52.0%) receiving 131I radioactive therapy in the endoscopic surgery group versus 11 cases (44.0%) in the open surgery group after surgery. In the follow-up of the endoscopic group, postoperative reexamination showed 1 case of right region IV lymph node metastasis with rising TG to conduct secondary surgery. In the remaining cases, there was no evidence of recurrence or metastasis.
Discussions
The Level Division Scheme for Cervical Lymph Nodes formulated by the America Surgery Academy of Otolaryngology in 1991, with continuous refinement and standardization, has been widely used in clinical practice, in which the lymph nodes in region VI are central region, also known as peripheral visceral lymph nodes, including prelaryngeal lymph nodes (Delphian lymph nodes), pretracheal lymph nodes, and paratracheal (tracheoesophageal sulcus) lymph nodes, with common carotid arteries to be the bilateral boundary, hyoid bone to be the superior boundary, suprasternal fossa to be the inferior, superficial layer of deep fascia at the anterior, and deep layer of deep fascia at the posterior. The lymph of the thyroid returns to this area first, which is where the first station of the lymph node metastasis occurs in thyroid cancer.
Differential thyroid cancer, the most commonest type that accounts for up to 90% of thyroid cancer, with a central lymph node metastasis rate as high as 20%–90%,8–10 makes thyroidectomy plus CLND the basic operative method treatment for it. Due to the limitation of the operating space and occlusion of the sternum and clavicle, CLND under endoscope through chest–breast approach is difficult and hard to operate especially when dissecting the lymph nodes in the right central region, the right RLN bypasses the subclavian artery leading to superficial ascending position, as well as the deep hidden lymphatic adipose tissue behind RLN. Therefore, its adaptation range, operation steps, and techniques are worth exploring.
Indication and contraindication of endoscopic thyroidectomy
Due to the hardness of tumor (poor elasticity) and the limitation of the size of Trocar tunnel, the size of cancer lesions under endoscopic thyroidectomy with CLND is generally required to be no bigger than 2 cm, so that the resected tumor can be removed from the tunnel smoothly to avoid the risks of cancerous rupture and implantation metastasis from tearing. Preoperative evidence suggesting lymph node metastasis in region VII is difficult to observe accurately under the endoscope through chest–breast approach, therefore, open surgery or combined with endoscopic thyroidectomy through oral approach 11 should be selected in this situation, to obtain the exact surgery field by observing from the top toward down. In addition, it should be noted that radical treatment of the tumor shall be the principle of operation for thyroid cancer, especially for the patients without cosmetic needs, or for cases that are difficult to achieve radical tumor resection, open surgery ought to be the choice. In Table 1, with statistically significant differences in age and gender, more young female patients were willing to choose endoscopic surgery for their beauty needs.
The indications and contraindications of this operation remain to be discussed. The summary of our experience is as follows: Indications: (1) tumor diameter ≤2 cm; (2) no extra-gland invasion suggested in preoperative imaging examination; (3) patients with hyperthyroidism taking oral iodine for preoperative preparation, along with evaluation on successful establishment of surgical operation space; and (4) tumor diameter greater than 2 cm and less than 3 cm can be considered as relative indication with evaluation on successfully passing through the Trocar tunnel. Contraindication: (1) tumor diameter >3 cm; (2) preoperative evidence suggesting lymph node metastasis in region VII; (3) patient intolerant to general anesthesia or with severe coagulopathy; and (4) secondary surgery or history of other neck surgery as a relative contraindication.
Selection of incision and establishment of space for endoscopic surgery
Since the bottom to upper endoscopic view of the chest–breast approach, the lymphatic adipose tissue close to the manubrium of sternum and the clavicle is easy to be blocked without affecting the operation. Effective and good exposure is very important. Overextension of the neck, to keep it at the same level as the chest (Fig. 1), can elevate the lower lymphatic adipose tissue. For female patients with larger areola, complete areola approach can be the choice3,6 (Fig. 2) to achieve good cosmetic results. Endoscopic operation through the areolar approach is difficult to perform in male patients due to the lack of chest fat and muscularity, but can move above the incision as a solution (Fig. 3).
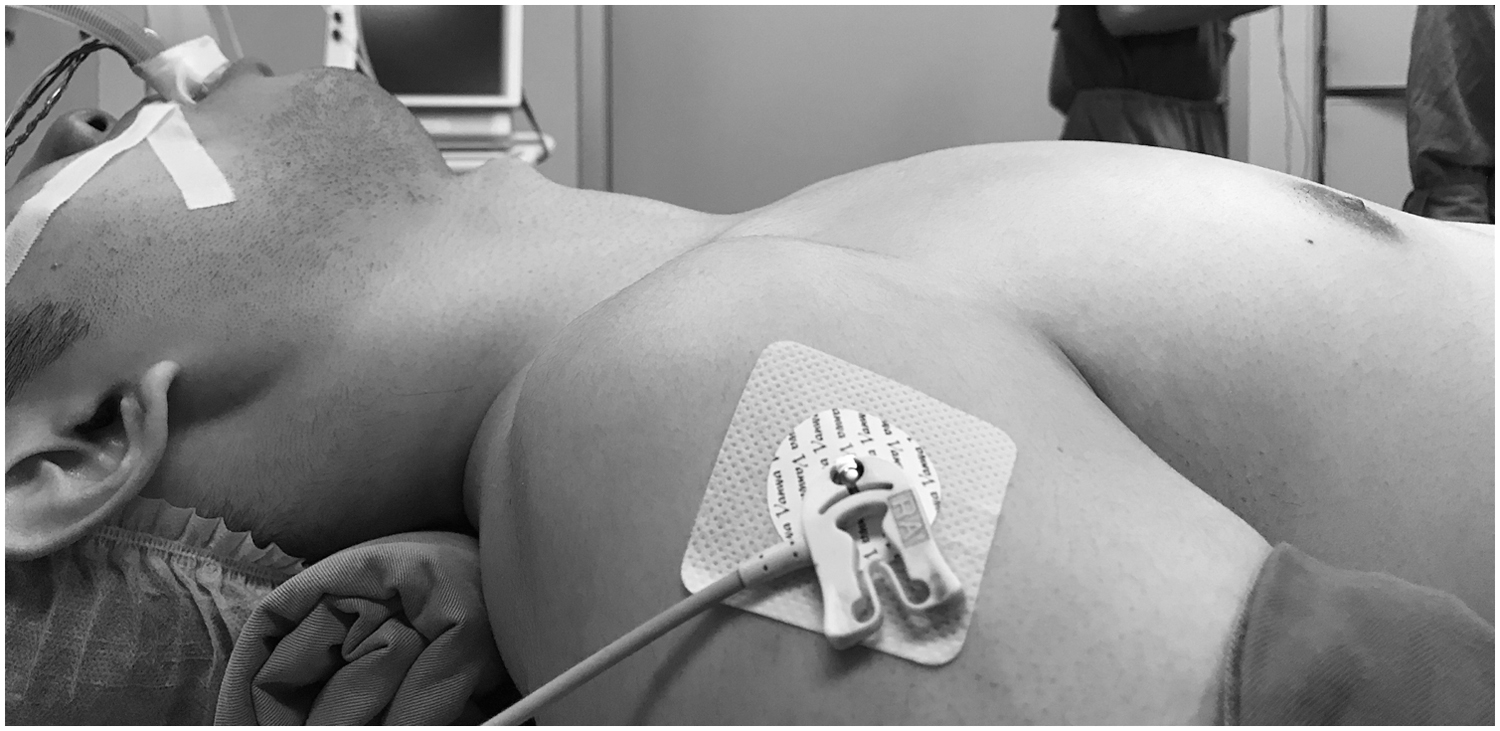
Overextension of the neck position.

The incisions of chest–breast approach in female patients.

The incisions of chest–breast approach in male patients.
In the endoscopic approach, creating the operating space by separating the superficial free skin flap through clinging to the anterior cervical anterior muscle is suggested. Remove the adipose tissue in front of the sternum to prevent the residual adipose tissue from blocking the lens view during subsequent lymph node dissection. In addition, a clear linea alba cervicalis can be seen after the separation of the layers, which facilitates the accurate downward incision of the linea alba cervicalis to maximum expose the central lymphoid adipose tissue (Fig. 4).
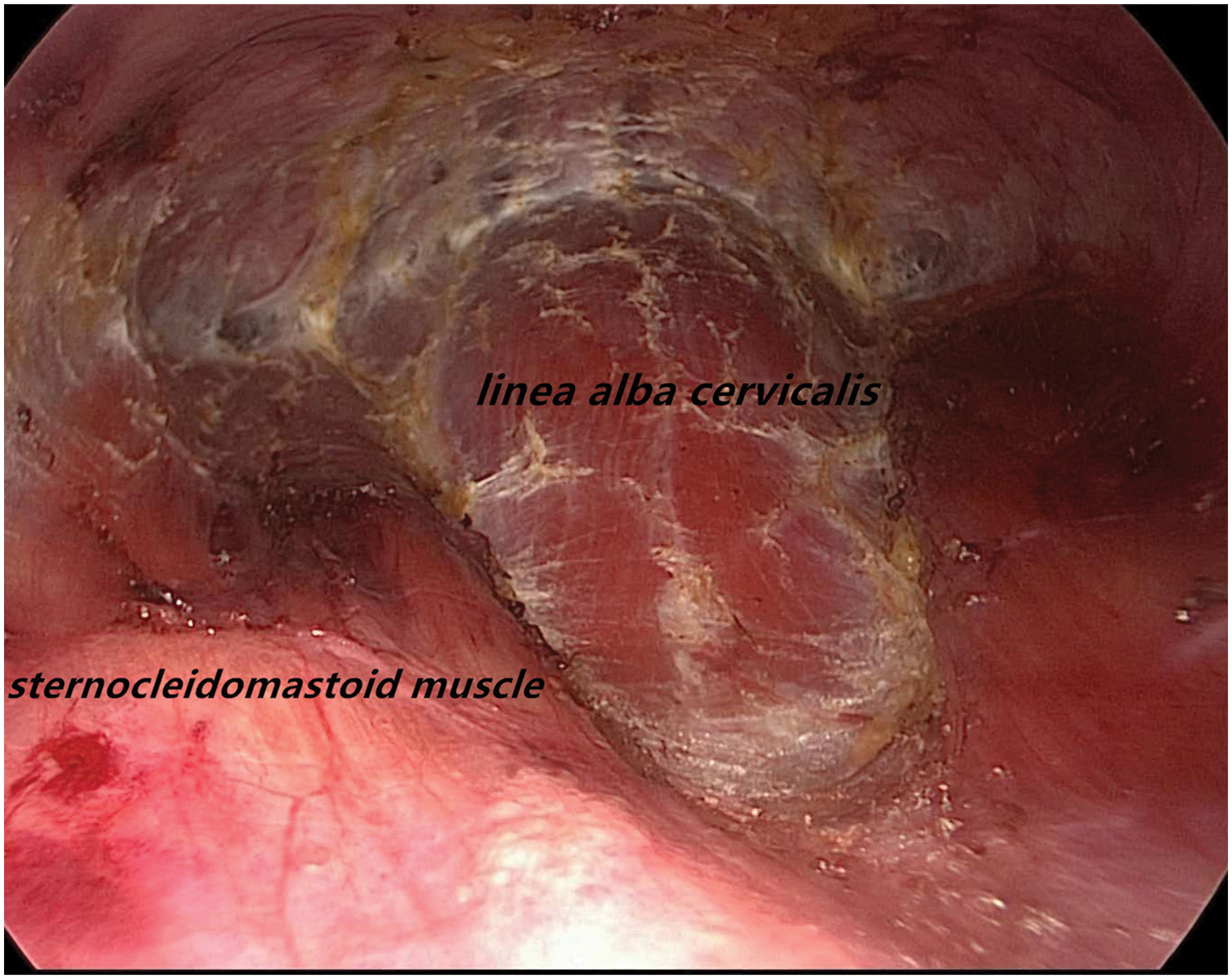
A clear linea alba cervicalis can be seen after the separation of the layers.
Range of lymph node dissection in endoscopic surgery
In principle, the operative range of CLND in endoscope is the same with open surgery. In the right side CLND, the lymph nodes in the front left of the trachea should also be dissected, but need to avoid excessive dissection to damage the left RLN. Because of superficial right RLN, the right central lymph node is divided into two groups as anterior and posterior RLN, namely, the lymph node anterior to the right RLN (LN-arRLN) and the LN-prRLN12,13 when moving through the gap of right central lymph adipose tissue. Due to its deep position, LN-prRLN is difficult to expose under the endoscope that may lead to neglected or omitted clearance. Therefore, for the right CLND, first dissect LN-arRLN, then dissociate the right RLN to dissect LN-prRLN. The right RLN should reach a 360 degree free state after cleaning.
Protection of RLN under the endoscope
Compared with open surgery, endoscopy, with the function of easy identification of the RLN and high-definition vision, can clearly and completely show the direction of RLN. Mastering of effective exposure with elaborate operative techniques can overcome the difficulty of lymph node dissection under the endoscope. In the thyroidectomy, the lobectomy should be performed as far as possible for full exposure of RLN in the thyroid bed. During lymph node dissection, searching and exposing the RLN from the low position to upward to gradually join with RLN segment at the thyroid bed is done. Also can conduct gradually an entire RLN exposure down forward from the exposed RLN segment in the thyroid bed if there is any difficulty to find RLN at the low position.
Attention should be paid at all times to avoid thermal damage of the ultrasonic scalpel when dissociating lymphatic adipose tissue around the RLN. It is our usual practice to cover the surface of the RLN with gauze strips after exposing the RLN, to devascularize by keeping the functional side of ultrasonic scalpel away from RLN, or to coagulate the small blood vessels through low gear of ultrasonic scalpel and then cut with scissors for the utmost avoidance of thermal damage of ultrasonic scalpel. During the operation, excessive pulling of RLN frequently happens in the process of exposing RLN due to the block of structure of trachea, anterior cervical muscle, sternum stem, and clavicle, with limited operation space to be avoided especially when the RLN is exposed at a low position. Our regular practice is to retract the anterior cervical muscle further outward with thread to obtain a better view, or use hook to push the trachea to the opposite side to fully expose it.
During the right side of the CLND, one should be alert to the existence possibility of rare nonrecurrent laryngeal nerve (NRLN) with a reported incidence of about 0.5%–1.0% 14 that is mostly found on the right side.15,16 Right NRLN is often associated with right subclavian artery variation or loss of innominate arteries. Preoperative cervical CT scan can predict the presence of NRLN in advance by observing whether there is vascular variability. After the severing of thyroid vein during surgery, all the cord-like structures emanating from the vascular sheath should be carefully screened to ensure no nerve before cutting. We recommend to routinely apply intraoperative neurophysiological monitoring under endoscope for easier identification of RLN direction, early warning of NRLN presence, and for more accurate identification and exposure of RLN.
Protection of parathyroid gland under the endoscope
During CLND, the lower thyroid artery and the important nutrient branch of the parathyroid gland should be carefully dissected and preserved under the radical cleaning to ensure the blood supply to parathyroid gland. Liu et al. 17 found in the study of gene knockout mice that thymus tissue is an auxiliary organ for the production of parathyroid hormone (PTH), and its PTH expression is also regulated by blood calcium levels. The thymus should be retained in situ as much as possible if not affected by the tumor. The lack of instrumentation for endoscopic thyroidectomy is the main reason for the increased difficulty of such surgery and Minilap can be added to assist in lifting for better operation if necessary.
The emphasized premise of parathyroid glands in situ retention is the preservation of vascular pedicles. Autotransplantation to contralateral sternocleidomastoid muscle, deltoid muscle, or subcutaneous of the forearm should be performed actively if the retained parathyroid glands are not confirmed to have a good blood supply. It is our usual practice to transplant the parathyroid gland into the contralateral sternocleidomastoid muscle—directly place and cut parathyroid tissues in front of the trachea under the endoscopic view (cutting in vivo to avoid the parathyroid fragments falling into the Trocar when passing through the subcutaneous tunnel). Pay attention to the blood supply of the parathyroid gland in situ and it is suggested to stab the capsule of the parathyroid gland with a needle if any existence of congestion.
Carefully search for suspicious parathyroid tissue in specimens after removal of thyroid gland and dissection of lymphatic adipose tissue and perform autotransplantation after confirmation of intraoperative freezing pathology or iPTH test strip.
Cervical sympathetic nerve and lymphatic vessel
The low incidence of cervical sympathetic nerve and lymphatic injury in CLND is rarely mentioned. But, we believe that under endoscopy, inexperienced surgeons are prone to cause damage by excessive traction that pulls the sympathetic nerves and lymphatic vessels located behind the vascular sheath to the medial side due to the difficulty of exposure. When cleaning LN-prRLN, the hook and Minilap can be used to help expose the surgical field by properly lifting the visceral fascia, accurately distinguishing the gap between the vascular sheath and the visceral fascia, and cutting the visceral fascia inside of the vascular sheath.
Lymph node clearance
The routine use of nanocarbon injection is recommended in surgery to trace the thyroid and regional lymph nodes, which can increase the dissected number of intraoperative lymph node and metastatic lymph node as well as negative tone developing parathyroid glands for the in situ retention of the parathyroid glands and reduction on incidence of intraoperative parathyroid injury and midsection rate. 18
In this study, no statistically significant difference was found in the number of dissected lymph nodes and metastatic lymph nodes, surgical complications, or postoperative recurrence rate between the two groups, which indicates the right side CLND under endoscope to be safe and feasible, combining radical tumor resection effect with esthetic effect. It is necessary to master the surgical characteristics and operation skills of the right side CLND under the endoscopy due to the difficulty of the surgery to further explore and study this technique.
There are still a lot of controversies at present as for whether routine CLND is required in thyroid cancer surgery. We agree with the recommendation in the CTA guidelines to perform ipsilateral CLND under the condition of effective preservation of parathyroid gland and RLN. In a word, the operation should take into account the radical cure and function protection of the tumor, and strictly grasp the surgical indications. It is not suggested to seek the cosmetic effect of endoscopic surgery, but sacrifice the radical cure of the tumor.
Conclusion
During the right CLND in endoscopic thyroidectomy through the chest–breast approach, the surgeon needs to be familiar with the anatomical characteristics of the right central area with rich experience and operating skills in endoscopic thyroidectomy due to its difficulty. Surgical indications and contraindications of this approach should be strictly controlled. For selected cases, endoscopic surgery is safe and feasible with the same dissected effect of lymph nodes in the right central region as open surgery, which is in line with the principle of radical treatment of tumors.
Footnotes
Acknowledgment
The authors thank Rujia Zeng for her great help with language.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.