
Abstract
Background:
Surgical management of complicated retroperitoneal mass is one of the most challenging urologic oncologic surgeries. This study aims to describe our technique and experience in dealing with retroperitoneal mass.
Methods:
Three patients with complicated retroperitoneal mass were treated with robot-assisted surgery with four arms through retroperitoneal approach.
Surgical Procedure:
Our standardized anatomic-based “kidney safe first, then mass resection” technique for robot-assisted complicated retroperitoneal mass resection focused on minimizing the chance of renal pedicle injury. Baseline demographics, pathology data, and latest follow-up outcome were obtained.
Results:
In this retrospectively reviewed case series, all 3 patients were successfully treated with robot-assisted surgery with four arms during retroperitoneal space. One patient received paravertebral mass resection 2 weeks after the robotic surgery. Mean data included operative time of 175 minutes, estimated blood loss was 133 mL, and hospital stay was 4 days. No complications occurred.
Conclusions:
Robot-assist surgery for complicated retroperitoneal mass with four arms is a safe and feasible way.
Patient Summary:
Mini-invasive treatment for retroperitoneal mass with robotic four arms through retroperitoneal approach is a feasible way. The approach reduces interruption of intracorporeal structure and organs. And patients could benefit from the retroperitoneal approach with a quicker recovery.
Introduction
Retroperitoneal tumor is a group of masses with various pathologies. It includes primary and secondary tumors that can be either benign or malignant. Tumors originating from retroperitoneal major organs such as the kidneys, adrenal glands, pancreas, duodenum, and colon are not included as retroperitoneal tumors in our report. Primary retroperitoneal tumors account for ∼0.1%–0.2% of all malignant tumors in the body, only ∼10%–20% of all primary retroperitoneal tumors are benign. 1 The most common malignancy is sarcoma, which accounts for >30% of all primary retroperitoneal tumors, 2 whereas fibromatosis, benign paraganglioma, lipoma, and schwannoma are considered as benign tumors. Spindle cell type tumors in retroperitoneal cavity are either benign or malignant depending on further tests such as immunostaining.
Robotic-assisted laparoscopic surgery system is a mini-invasive and precise operation platform, which has a great advantage in a limited area such as the retropubic space. Retroperitoneal cavity is a relatively small space especially when the mass has a big size. Traditionally three arms are used for the manipulation in retroperitoneal cavity, whereas it is still difficult when the small space is occupied by a big mass. Hence, the fourth arm was placed after pushing aside the peritoneum. We summarize our initial experience in placing the fourth arm for excision of complicated retroperitoneal tumors.
Methods
Approval was attained from the Ethics Committee of the First Affiliated Hospital, School of Medicine, Zhejiang University. Informed consent was signed by related patients. The diameter of the mass is >10 cm, and (or) it surrounds critical structures and organs are defined as complicated retroperitoneal tumor.
Surgical technique
The patient was in supine position before the general endotracheal anesthesia. After intubation, the patient was placed in a lateral position (the tumor was on the upside), and a cushion was used to elevate the waist part while the bed was folded in ∼15°. First, the camera port was placed in the midaxillary line between the coastal margin and the iliac crest, adjusting the port up or down according to the location of tumors. The retroperitoneum was entered under vision, and a self-made balloon was used to dilate the retroperitoneal cavity. An 8 mm trocar was placed in the posterior axillary line 3 cm higher than the camera port level using finger-guide technique. In brief, left-hand index finger touched the inner side of the 8 mm port through the camera port, the skin was incised and the 8 mm trocar was inserted into retroperitoneum guided by the finger. The second 8 mm port was placed in the anterior axillary line in the same level of the first 8 mm port under the same finger-guide technique. The assistant 12 mm port was placed 5 cm caudally to the second 8 mm port in the anterior axillary line. The third 8 mm port was inserted into the retroperitoneum under vision after the peritoneum was pushed away from the transversus abdominis, in the same level as the former two 8 mm ports and 6–8 cm medially to the second 8 mm port. The Da Vinci robot was docked over the patient's head, and 15° to the ventral side. Then 30° down camera was routinely used during the operation. A monopolar curved scissor was used in the right-hand arm, and a Maryland forceps was used in the left-hand arm. A ProGrasp™ forceps was used in the third 8 mm arm (the fourth arm) (Fig. 1).
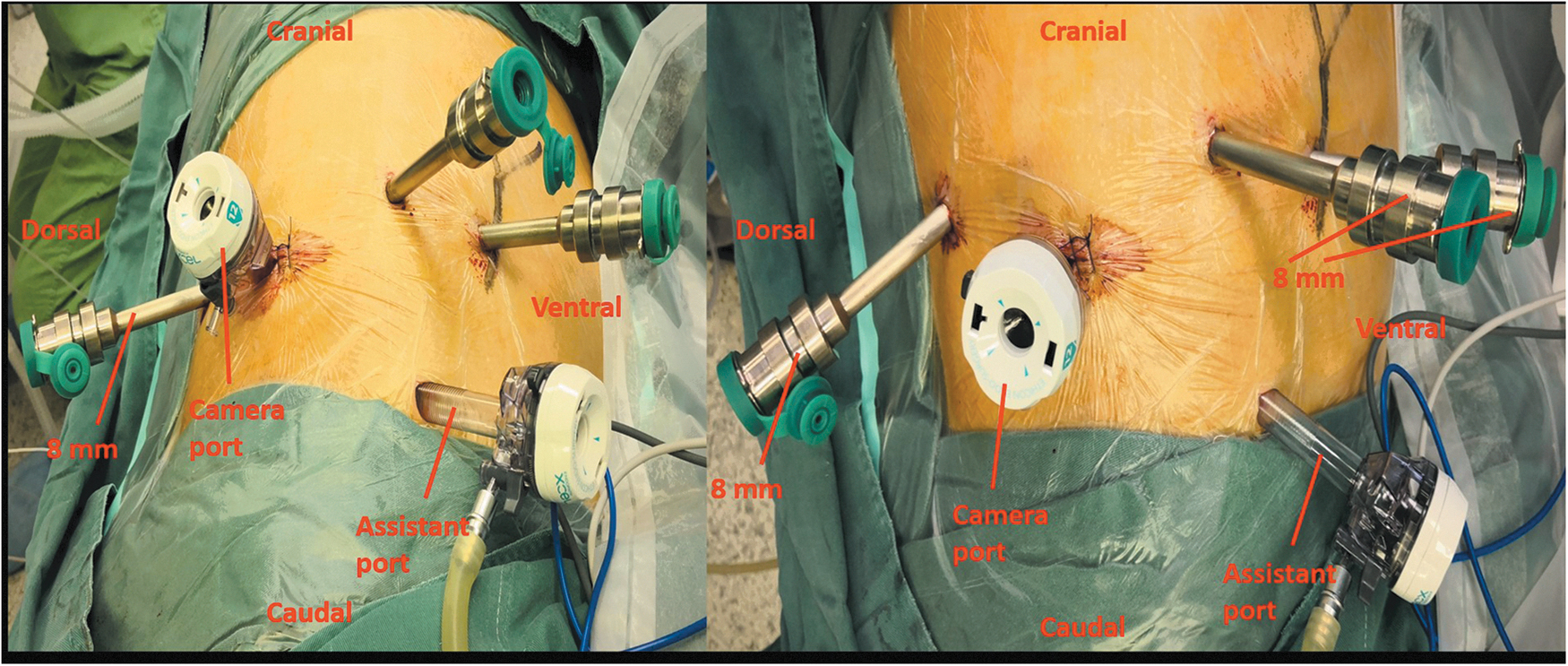
Patient's position and trocar placement.
After placement of instruments and docking, the fat tissue in retroperitoneum was cleared to expose Gerota's fascia. Then the fascia was incised using the monopolar scissor and separated the kidney from the psoas muscle. The ProGrasp forceps was inserted under vision, and it was routinely used to help exposure. Next, the important step was to find out the renal hilum. The fourth arm was used to hold or retract the kidney, which made much easier for surgeon to find the hilum. Once the hilum was safely exposed, the fourth arm was used to help expose the operation field, and the mass was carefully separated from surrounding tissue and removed.
Results
Result 1
Female, 39 years, a right retroperitoneal mass was found after health examination. The patient had no fever, no abdominal pain, nor dizziness. Ultrasound showed that there was a hypoechoic area between the right adrenal gland and inferior vena cava, ∼10 × 7.3 × 5.6 cm in size, highlight spots could be detected, and no obvious blood flow signal was found within the mass. Computed tomography (CT) scan indicated that there was a low-density mass between the right adrenal gland and inferior vena cava (Fig. 2).
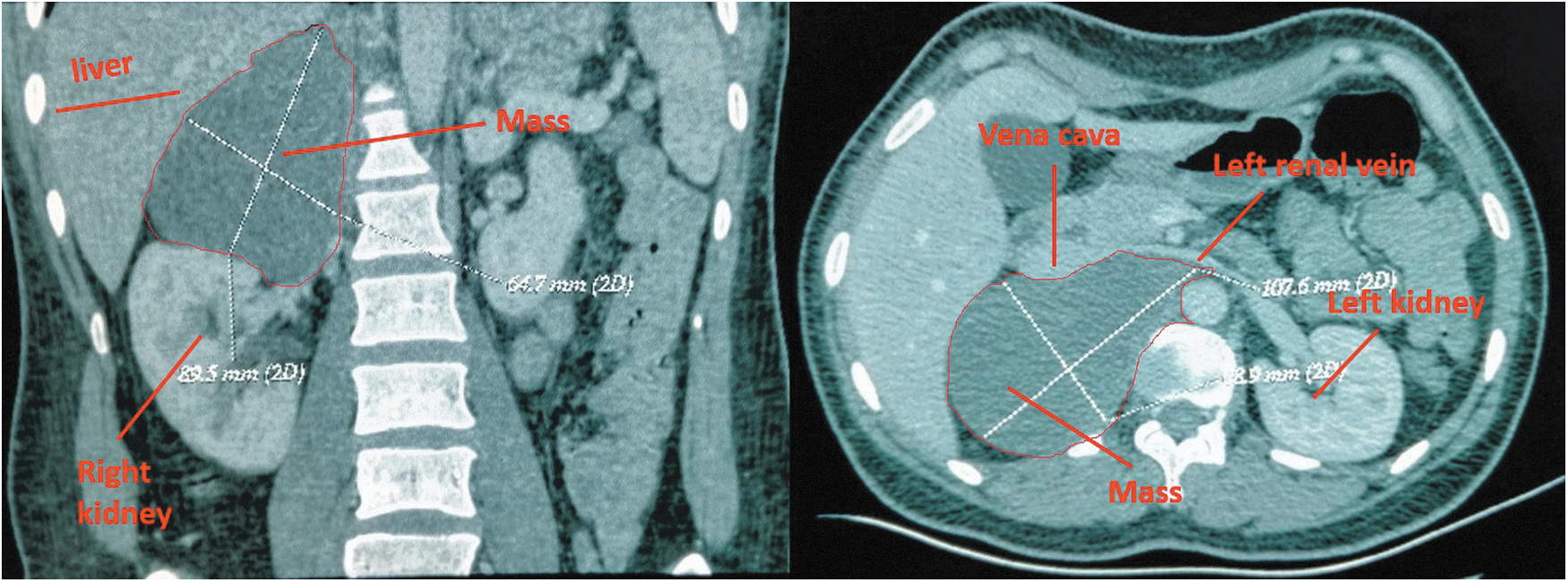
CT images showed the big mass in the right retroperitoneal cavity. CT, computed tomography.
The mass was removed under robotic-assisted laparoscopic surgery system (Da Vinci®) with four arms retroperitoneally (Fig. 3). The operation time was 141 minutes (the period was from skin sterilization to incision closure). Estimated blood loss was 50 mL. The pathology showed that the tumor cells were spindle shaped, well differentiated, and a spindle cell type tumor was considered (Fig. 4). The follow-up time was 23 months, and no recurrence was observed.
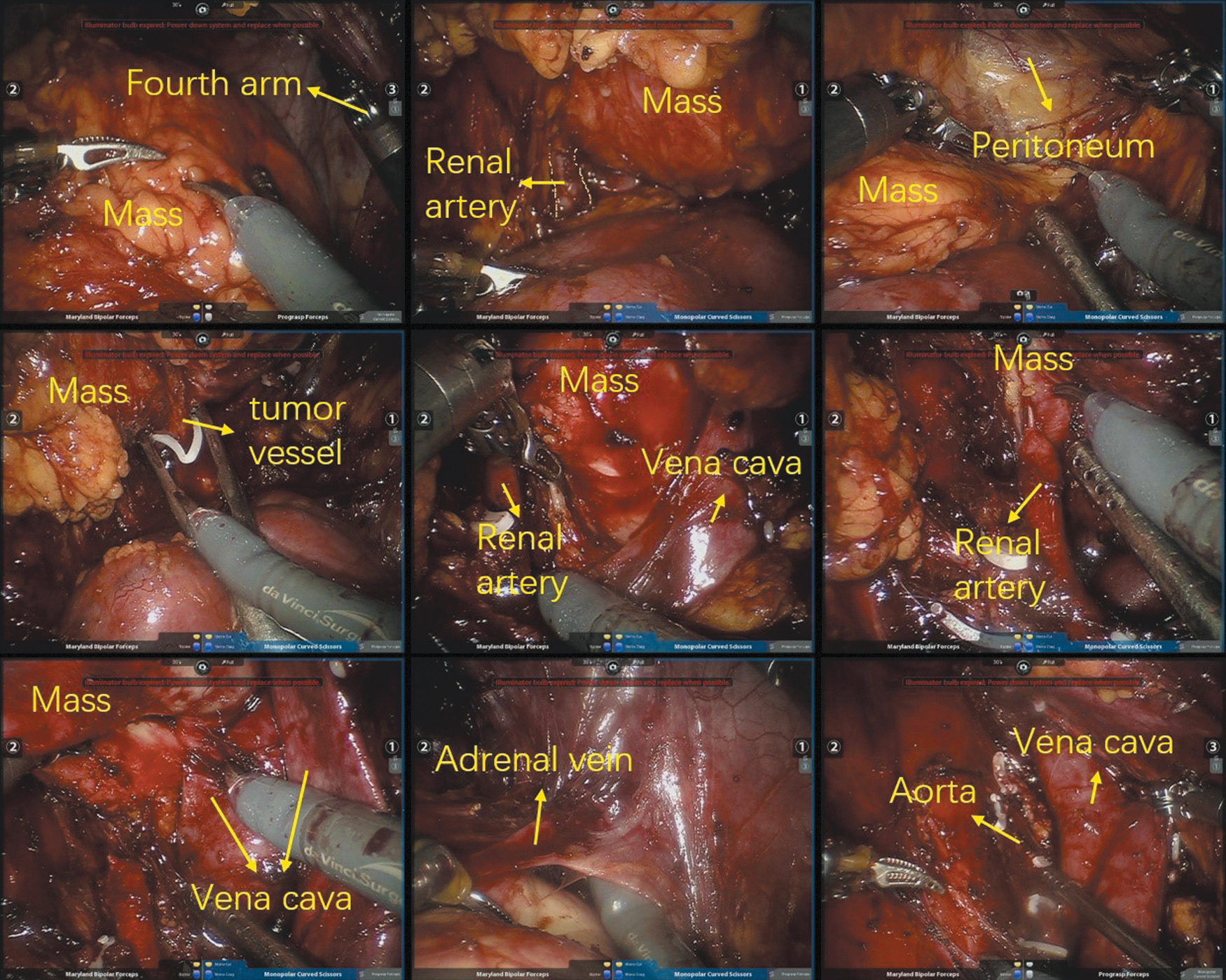
Robotic surgery of removing the big mass.
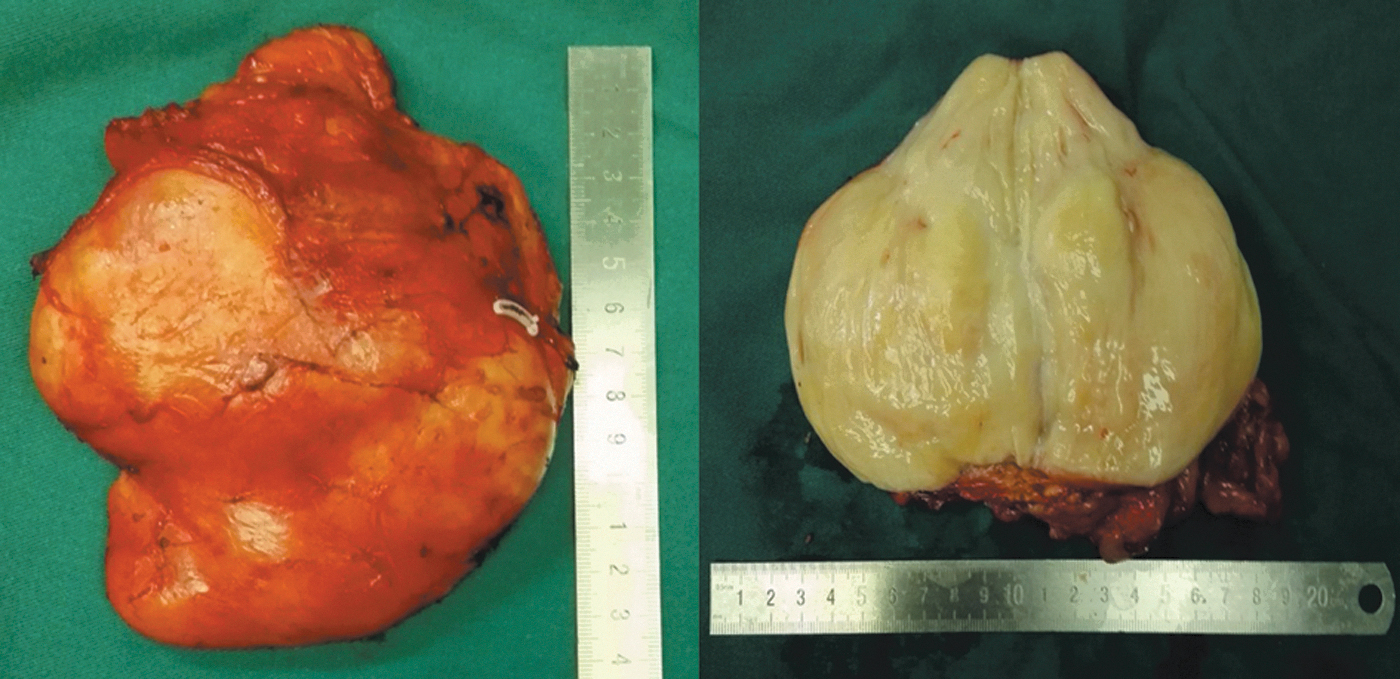
Gross specimen showed the mass was solid with light yellow.
Result 2
Male, 65 years, a left retroperitoneal mass was found after health examination, the patient had no symptom and no positive signs. Local hospital CT scan showed that there was a mass in soft connective tissue medial-superior to the left kidney, the mass density was a little higher after enhancement (Fig. 5). The mass was irregular and part of it was surrounded by left renal artery and vein. The retroperitoneal biopsy was performed in local hospital, the result indicated that it was a connective tissue tumor, neurogenic tumor should be considered.

CT scan showed the mass closely attached to aorta and surrounded left renal artery. CT, computed tomography.
The patient received operation under robotic-assisted laparoscopic surgery system (Da Vinci) with four arms. The mass was taper, ∼15 cm in length and 6 cm in width. The whole surgery time was 219 minutes, estimated blood loss was 200 mL. The pathology showed that it was a spindle-shaped cell tumor (Schwannoma) (Fig. 6). Immunostaining result S-100(+), Nestin(+), Ki-67(+), CD34(−), SMA(−), DOG-1(−), CD117(−). The follow-up time was 23 months, and no recurrence was observed.

Gross specimen was irregular and yellow.
Result 3
Male, 70 years, left lumbar pain for 8 months, it became worse after a long time sitting. Magnetic resonance imaging and CT scan showed that the mass located on the left side of second lumbar, closely attached to the beginning part of the left renal artery and aorta and pushed them forwardly, part of the mass was under the psoas major (Fig. 7). It was also considered as a neurogenic tumor.

CT images showed the mass hidden under the psoas major and stuck to the lumbar vertebra. CT, computed tomography.
Robotic-assisted laparoscopic surgery was performed for this patient with four arms through retroperitoneal approach (Fig. 8). The operation time was 164 minutes, estimated blood loss was 50 mL. The pathology result showed that it was a schwannoma (Fig. 9). Immunostaining showed CD117 (−), S-100 (+), Desmin (−), CD34 (−), SMA (−), DOG-1 (−), Ki-67 (+low), CK (−). The follow-up time was 22 months, and no recurrence was observed.
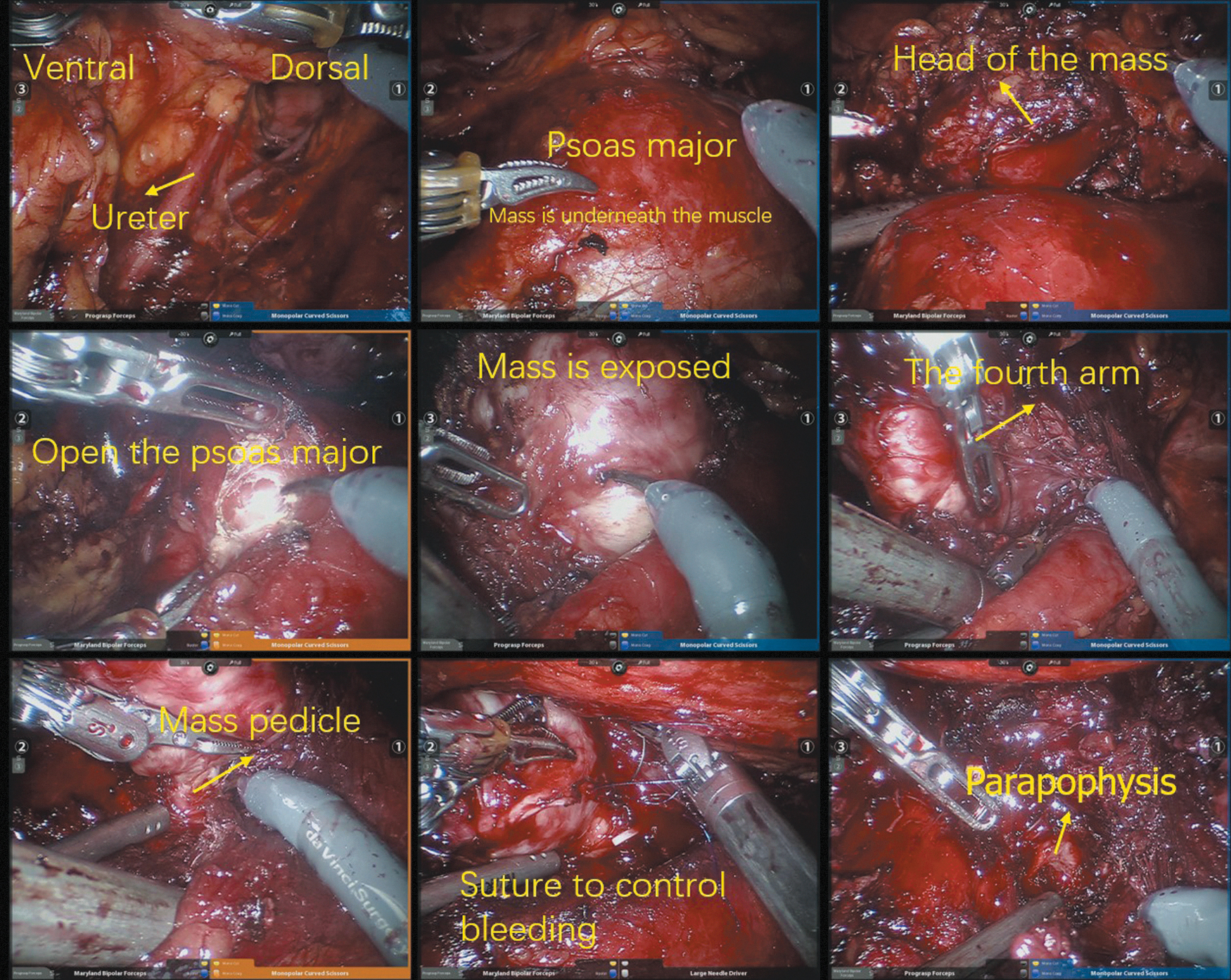
Robotic removing of the mass.

Gross specimen showed the mass was a yellow and white solid.
Discussion
To date, limited reports upon the minimal-invasive surgery for larger or complicated retroperitoneal mass, open surgery is still the major approach. Although several reports mentioned that they performed laparoscopic surgery3,4 or robot-assisted excision 5 for retroperitoneal tumors, transperitoneal approach were commonly used. Bindal et al. and Yang et al. reported a complicated right retroperitoneal mass was resected under robotic-assisted laparoscopic surgical system through transperitoneal way.6,7
To the best of our knowledge, no literature report robot-assisted surgery for complicated retroperitoneal tumor through retroperitoneal way. Compared with transperitoneal approach, retroperitoneal way can expose the mass more directly, shorten operation time, little interrupt intestine, and reduce the length of hospital stay. 8 Although the retroperitoneal space is relatively small, the application of the fourth arm can perfectly solve this problem. Especially for those mass hidden behind vena cava, which is difficult to be exposed through transperitoneal way.
Schwannoma is composed of Schwann cells of the peripheral nerve sheath. 9 It is usually benign and has a surgical capsule. 10 Schwannoma contains compact cellular lesions, 11 and it is usually solitary, firm, well–circumscribed, and smooth-surfaced tumors. 9 It is not as fragile as we thought. The color of cut section is light tan and glistening, and sometimes shows yellow patches. In our operation procedure, we carefully free the mass with robotic instruments. Maryland forceps is in the left hand, monopolar scissor is on the right hand, and the ProGrasp forceps is in the fourth arm. The ProGrasp plays a significant role during the operation. It immobilizes the mass or keeps the adjacent tissue away, which helps exposure of the surgical zone. Under the help of the fourth arm, it does not need to grab the mass by hand or use “closed handed retraction” technique.
There is a controversy upon the biopsy for retroperitoneal mass. Some experts believe that it will cause tunnel metastasis if it is highly malignant. And keeping the integrity of the whole mass is in the first place. Chew et al. reported that biopsy led to ∼11.1% false negative results and some received an error in management. 12 The sensitivity of diagnosis between biopsy and nonbiopsy group was similar. Furthermore, the biopsy might cause the injury of ureter. And the specimen got from the needle biopsy is usually not sufficient to clarify the subtypes pathologically. 13 So, Chew et al. thought that biopsy did not make any sense for those resectable large retroperitoneal mass. Other specialists thought that biopsy is safe and useful to identify retroperitoneal sarcomas. 14 The accuracy of core biopsy ranges from 84% to 97% in determining retroperitoneal sarcoma. 15 Patients who fall into categories listed as follows should receive biopsy 16 : (1) the diagnosis is uncertain according to clinical and radiological appearance, and (2) pathology is mandatory before management (neoadjuvant therapy or chemotherapy).
In our case series, pathological property of these tumors is considered to be nonmalignant. Some centers report that retroperitoneal tumors are mostly malignant.17,18 Malignant mass would be more challenging to manage since they attach to surrounding critical structure or organs more closely. Thus, it is important for the surgeon to have a first impression: What is the nature of the mass? And realize the relationship between critical vessels and organs. Sometimes, it needs multidiscipline cooperation during the surgery. At the beginning of this century, there was a debate on the surgical region of malignant tumor. Some experts thought that an extended resection should be performed, which meant that adjacent organs and soft tissue without gross invasion should also be removed simultaneously. 19 Although the 5-year recurrent rate was higher in extended resection group, the overall survival was similar compared with standard resection. 20 A more “personalized” histology-based management strategy is recommended. In our second case, if it was malignant, a more radical resection would be performed, including the adjacent kidney. If the pathology indicates that the mass is highly malignant and it can be removed radically from the radiologist's perspective, we recommend neoadjuvant therapy first.
Conclusion
Surgical management of retroperitoneal mass under robotic surgical platform through retroperitoneal approach is feasible and safe, especially using the fourth arm in the retroperitoneal space.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the Ethical Standards of the Institutional Research Committee (The Ethics Committee of the First Affiliated Hospital, School of Medicine, Zhejiang University) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This program was supported by National Natural Science Foundation of China (No. 81800558 and No. 81772270), Zhejiang Provincial Natural Science Foundation of China (No. LQ16H030002), and Zhejiang Medical and Health Science and Technology Project (No. 2016KYB086).