
Abstract
Abstract
Introduction:
Transoral endoscopic thyroidectomy by vestibular approach (TOETVA) is a relatively new technique for the surgical treatment of thyroid diseases. We present the initial experience of a reference hospital of Mexico with TOETVA.
Materials and Methods:
This is a comparative retrospective study of cases (TOETVA) and controls (open thyroidectomy) treated by the endocrine surgeons between July 2017 and April 2019. Cases were patients of any gender, older than 18 years of age, with malignant thyroid nodules <2 cm or undetermined <5 cm without extrathyroidal extension and no lymph node or distant metastasis. Demographic, operative, and postoperative data were obtained and analyzed.
Results:
Twenty patients were surgically treated by TOETVA during the study period. Controls were paired based on type of surgery and dominant thyroid nodule. Ninety percent of the patients had a definitive diagnosis of malignancy. No statistically significant differences were found in age, BMI, length of stay, thyroid lobes size, and complication rates. Operative time was longer in TOETVA (216.7 ± 62.5 vs. 153.9 ± 49.25 minutes; t test P < .0001) and intraoperative blood loss was lesser for the TOETVA group (38.25 ± 38.9 vs. 101.8 ± 126.6 mL; t test P < .04).
Conclusions:
TOETVA is a feasible and relatively safe surgical technique for patients with benign and malignant thyroid diseases. Complication rates seem to be comparable with conventional open technique with lesser intraoperative bleeding; nevertheless, it requires longer operative times.
Introduction
Open thyroidectomy is currently the gold standard for the treatment of surgical thyroid disorders in many countries worldwide. Open thyroidectomy is generally a safe procedure with a low complication rate in experienced hands. However, a neck scar is unavoidable1,2 and it may have a negative impact on the quality of life for some patients.3,4 Techniques for remote access thyroid surgery have been mainly developed in the past two decades. With these techniques the neck scar is avoided and frequently smaller, offering better cosmetic results.5–9
Transoral thyroidectomy (TOT) is considered the first approach through a natural orifice transluminal endoscopic surgery. This was initially described by Wilhelm et al. in 2010, 10 subsequently modified and improved by Richmon 11 and Anuwong. 12 Such improvements included the use of the oral vestibule for the surgical access instead of the sublingual space, which gave a new name to the technique: transoral endoscopic thyroidectomy vestibular approach (TOETVA). Associated morbidity with this approach significantly decreased the injury of the floor of the mouth and hypoglossal nerves observed in TOT.
Prevailing indications for TOETVA include reluctance for a visible surgical scar and history of pathological or hypertrophic scarring in patients with small thyroid glands. On the contrary, contraindications for this approach include patients with a history of head and neck surgery or radiation, intolerance to general anesthesia, presence of an active oral infection, poorly controlled hyperthyroidism, suspicion or evidence of extrathyroidal extension of malignant thyroid lesions, and evidence of recurrent laryngeal nerve palsy (RLN). 13 Metastatic lymph node disease in the central neck compartment is considered a relative contraindication and up to now, metastases to the lateral compartment is a formal contraindication.14,15
In Latin America, the reported experience with TOETVA is still limited. Tesseroli et al. in Brazil 16 reported 9 patients with this technique and as far as we know there is no published experience in Mexico.
The aim of this study was to analyze our initial experience with TOETVA in a reference hospital for endocrine diseases in Mexico City and to preliminarily compare it with the conventional open technique.
Materials and Methods
This is a case–control study from a nested group of patients from a larger cohort with a prospective follow-up and ambilective collection of data. We considered as “cases” patients who underwent TOETVA, whereas “controls” were paired patients based on the size of the dominant thyroid nodule and type of surgical procedure, matched for a 1:1 ratio from our larger cohort. Selection criteria for TOETVA were patients older than 18 years, any gender, with malignant thyroid nodules <2 cm or undetermined nodules <5 cm documented by cervical ultrasound and cytology results between July 2017 and April 2019. Patients with previous thyroid surgery, history of cervical radiation, evidence of extrathyroidal extension or lymph node metastasis in the central or lateral compartments were excluded. All cases were discussed by a multidisciplinary team of experts on thyroid endocrinology, pathology, radiology, and surgical endocrinology. Our institutional review board approved the study (CIBH 3048).
Descriptive and inferential statistics were performed in accordance to the variable's natural scaling by means of IBM® SPSS© Statistics version 20 software (SPSS© Chicago, IL). For mathematical contrast we opted for parametric tests (Student's t-test for dimensional and chi-square test for categorical) and nonparametric (Mann–Whitney U test for dimensional variables and chi-square or Fisher's exact test for categorical) based on the variable data statistical distribution. Any value of P ≤ .05 or 5% (for an alpha or type 1 error) was considered statistically significant for a two-sided hypothesis test.
Surgical technique
Equipment needed for TOETVA conformed by standard videoendoscopic devices, instruments, and intraoperative neuromonitoring system (EMG endotracheal tube of NIM Trivantage® 8.0 mm ID × 10.7 mm OD; Medtronic Xomed, Inc., Jacksonville, FL). Endoscopic instruments included endograspers, Marylin dissectors, a 30-degree scope, and ultrasonic energy (HARMONIC ACE® +7 shears). For intermittent intraoperative neuromonitoring, we used either a long probe or a neuromonitoring cable coupled to a monopolar energy endoscopic hook. A Tenckhoff's catheter tunneling device with a blunt tip was used for the initial mechanical dissection of the subplatysmal surgical workspace. Specimens were retrieved in a sterile plastic bag.
All patients underwent 3 mouth washes with diluted 0.12% chlorhexidine gluconate. The combination of ceftriaxone 1 g or cephalotin 1 g plus metronidazole 500 mg was intravenously administered as antibiotic prophylaxis. Balanced general anesthesia was provided using nasotracheal or oral intubation. Patients were placed in the supine position with partial cervical extension and both arms in complete adduction. After standard skin preparation and placement of sterile surgical drapes, we injected local anesthesia (2% ropivacaine +0.5 mg of epinephrine solution) in the incision sites of the oral vestibule and the subcutaneous tissue of the chin. Surgical incisions were performed with a surgical scalpel at the junction of the inferior lip with the vestibule mucosa. One in the midline and 2 lateral in front of the canine teeth.
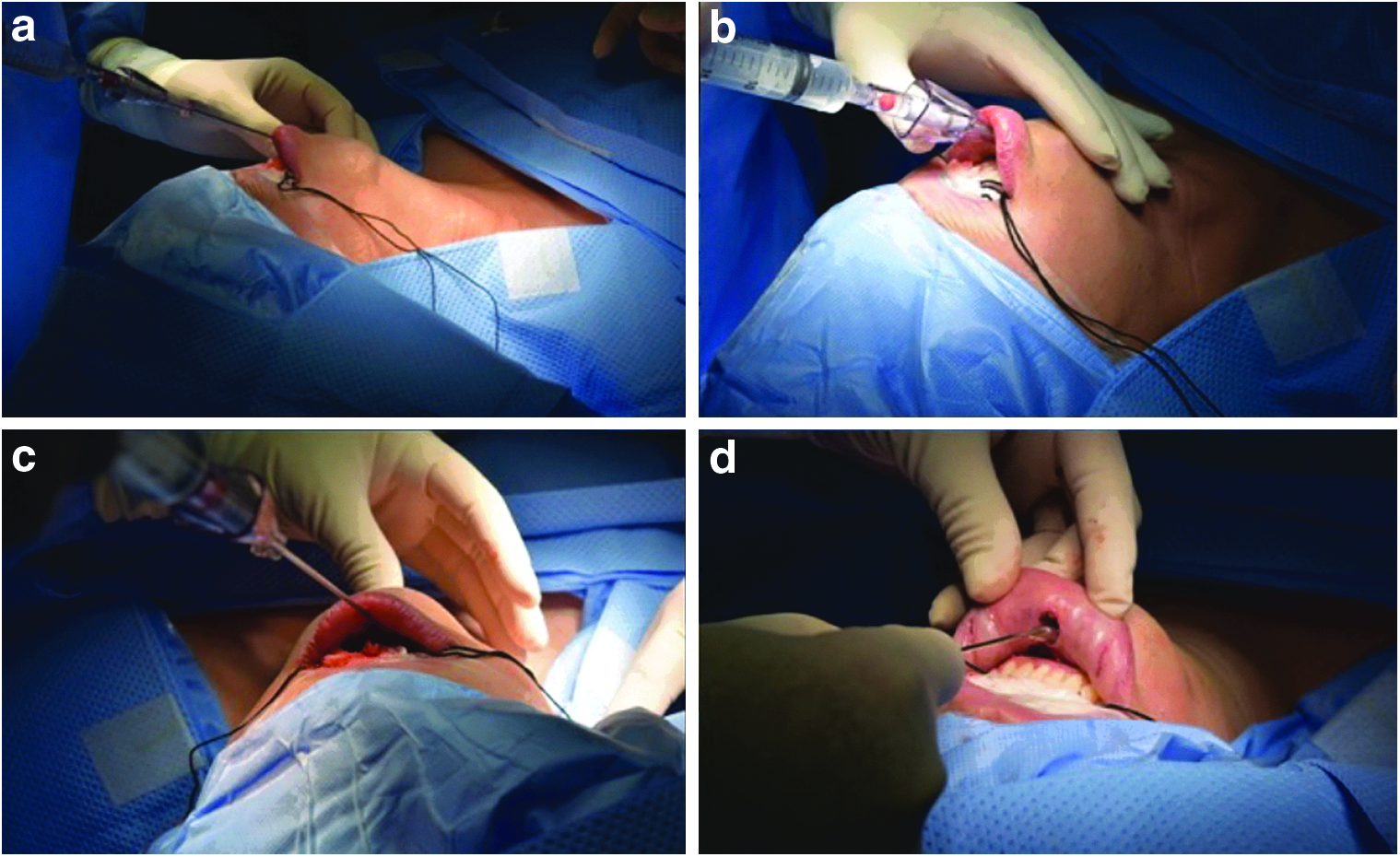
Blunt dissection to access the subplatysmal space was performed with Kelly clamps. Subplatysmal hydrodissection of the anterior cervical region up to the sternal notch was initially performed using a Veress needle with 500 mL of 0.9% saline plus 1 mg of epinephrine (Fig. 1a–c). Dissection was then completed mechanically with the Tenckhoff's catheter tunneling device (Fig. 1d). One 10 mm (midline) and two 5 mm (lateral) surgical trocars were placed and carbon dioxide was insufflated at a pressure ranging from 6 to 8 mmHg. Dissection between the platysma and the strap muscles was completed using the ultrasonic energy device. Linea alba cervicalis was identified and incised to expose the trachea and the thyroid gland. With the endoscopic dissection instruments, a tunnel was formed between the thyroid isthmus and the anterior wall of the trachea. Berry's ligament was divided, transecting the thyroid isthmus (Fig. 2a).
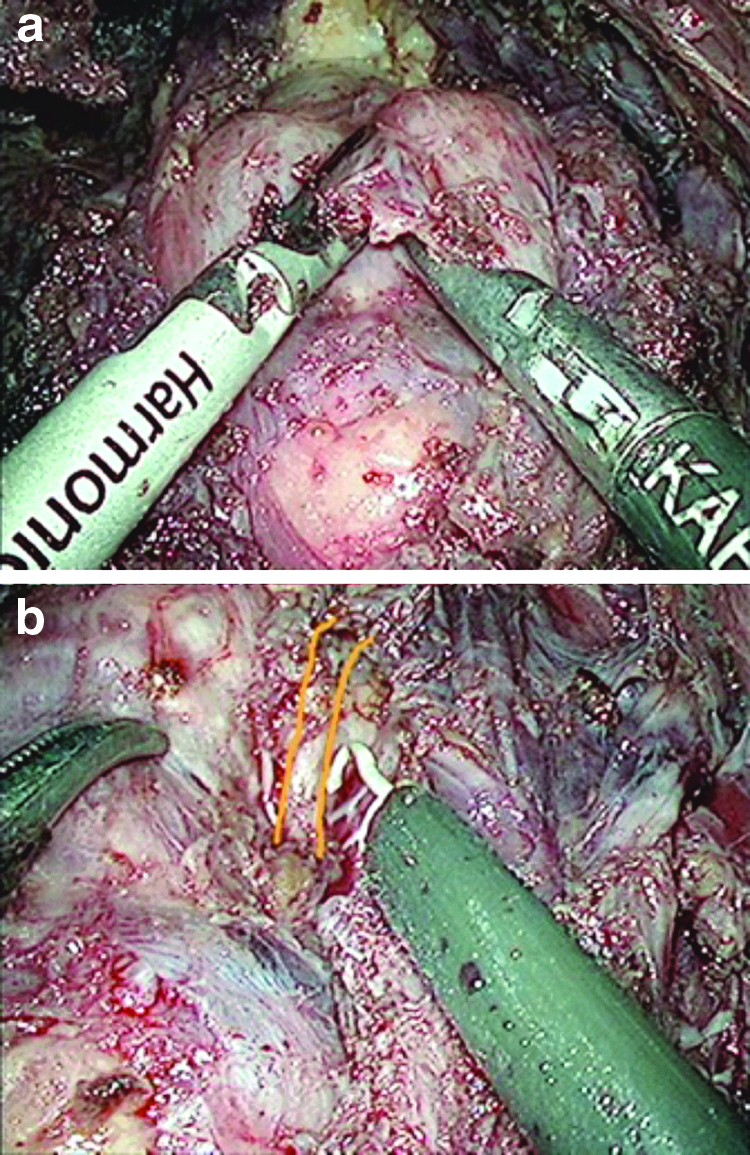
Systematically, the lobe with the dominant or suspicious nodule was dissected first. A skin traction suture and a lateral suture involving the strap muscles were placed to enhance the workspace and improve visualization. Medial traction was applied while the lobectomy was carried out after the same principles as a conventional open procedure: displacement of the strap muscles, dissection of the superior vascular pedicle, identification and preservation of upper and lower parathyroid glands, and RLN using the neuromonitoring equipment to facilitate its proper identification (Fig. 2b). Contralateral lobectomy was carried out in the similar way when total thyroidectomy was required. Thyroid lobe was extracted through the 10 mm trocar incision made on the midline of the oral vestibule.
The strap muscles were sutured with a 3-0 absorbable monofilament barbed polyglecaprone-25 (Stratafix™ Spiral Monocryl; Johnson & Johnson Medical Devices—Latin America, LLC). Vestibular incisions were closed in 2 layers with a 5-0 absorbable monofilament suture based on polyglecaprone-25 (medical devices Monocryl; Johnson & Johnson— Latin America, LLC).
After patient extubation, a compressive dressing on the anterior cervical and mandibular region was placed. Two additional doses of antibiotic prophylaxis were administered. Amoxicillin/clavulanic acid 875/125 mg per os was prescribed for 5 more days. Liquids were started on the same day and normal diet on postoperative day 1.
Results
Twenty patients underwent TOETVA from July 2017 to April 2019. There were 18 (90%) women and 2 (10%) men, with a mean ± SD age of 48.1 ± 15.67 years (range = 19–77) and mean ± SD BMI of 27.97 ± 5.6 kg/m2 (range = 21.48–40.99). Thyroid nodule mean ± SD size was 17.1 ± 18.57 mm (range = 7–90). Thirteen (65%) patients underwent total thyroidectomy, 3 (15%) hemithyroidectomy, 2 (10%) near-total thyroidectomy, 1 (5%) subtotal thyroidectomy, and 1 (5%) total thyroidectomy plus prophylactic central compartment lymph node dissection. Three (15%) of 13 total thyroidectomies were converted into conventional Kocher's incision, 2 because of problems with the nasotracheal intubation and 1 because it was impossible to remove the specimen through the vestibular incision. Mean ± SD operative time was 216.7 ± 62.55 minutes, whereas estimated blood loss was 38.25 ± 38.9 mL. Mean 24-hour postoperative pain was 2.65 ± 1.6 points according to the Numeric Rating Scale for Pain (NRS-Pain) and mean length of stay (LOS) was 2.0 ± 1.4 days.
As surgical complication, 1 (5%) patient developed a cervical hematoma and a subsequent surgical site infection, requiring antibiotic treatment and drainage with subsequent satisfactory evolution. Postoperative transient hypoparathyroidism was observed in 5 patients (25%), requiring oral calcium supplementation and vitamin D analogs. No permanent hypoparathyroidism was recorded. Two patients (10%) presented temporary postoperative hoarseness, recovering during the first 6 months after surgery but no permanent vocal cord palsy was recorded. Three patients (15%) presented transient paresis of the mental nerve with decreased mobility of the lower lip, with full recovery. It is important to point out that 2 patients were converted to open surgery because of troubles related to the nasotracheal intubation. Nevertheless, on the second half of our experience we have used oral intubation instead without any further issue.
Comparative demographic and operative-related variables between cases and controls are given in Table 1. Groups were statistically similar in terms of age, BMI, thyroid nodule size, thyroid size, and LOS. Estimated blood loss was lesser in the TOETVA than in the conventional group (38.25 ± 38.9 vs. 101.8 ± 126.6 mL respectively; t test, P < .04). However, operative time was significantly higher in the TOETVA group (216.7 ± 62.5 vs. 153.9 ± 49.25 minutes, respectively; t test, P < .0001) (Figure 3).

Boxplot for operative time and intraoperative bleeding among groups. TOETVA, transoral endoscopic thyroidectomy by vestibular approach.
Demographic, Operative and Postoperative Features Among Contrasted Groups
LOS, length of stay; LTL, left thyroid lobe; RTL, right thyroid lobe; TOETVA, transoral endoscopic thyroidectomy by vestibular approach.
Thyroid cancer and nodules suspicious for malignancy (Categories V and VI of the Bethesda System) were the most common indications for surgery in both groups (75% in TOETVA group and 70% for the control group). Thyroid cancer was the definitive diagnosis in 90% of the patients (Table 1), being papillary thyroid carcinoma, the most common type as expected.
Postoperative complications did not reveal any statistically significant difference among groups as given in Figure 4. Mean ± SD follow-up in our studied patients was 47.85 ± 49.3 (range = 1–181 months).
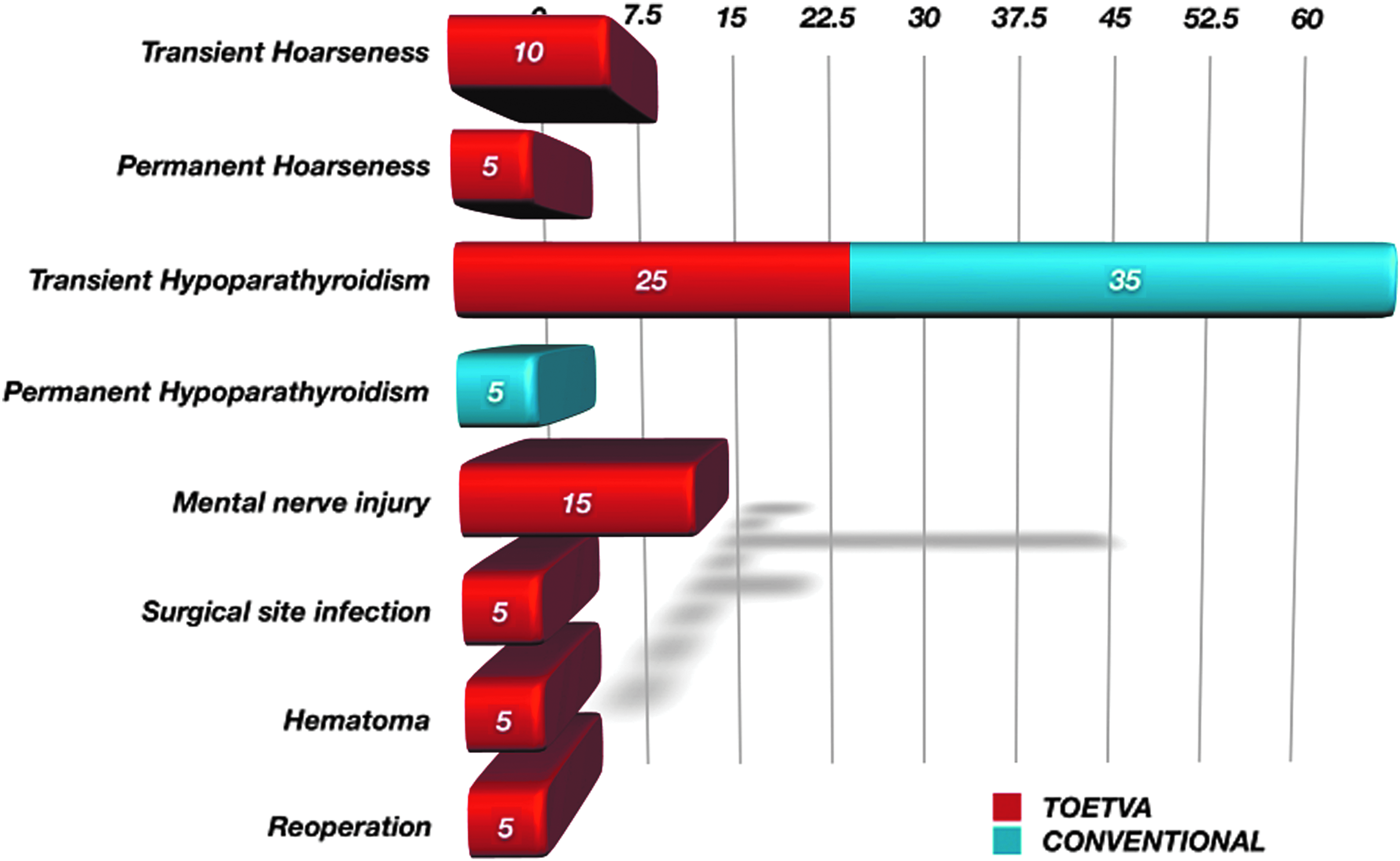
Percentage of complications for each surgical technique group. TOETVA, transoral endoscopic thyroidectomy by vestibular approach.
Discussion
After the sublingual transoral technique was initially described by Wilhelm et al., 10 the transvestibular modification also known as TOETVA made this approach more attractive for many surgeons. In an initial comparative study, Anuwong 12 reported a significant decrease in morbidity, SSI (2.5% vs. 0%), mental nerve injury (75% vs. 0%), transient RLN injury (25% vs. 3.3%), and permanent RLN injury (12.5% vs. 0%) when sublingual approach was compared with TOETVA. The potential advantages of the TOETVA are as follows: (1) It avoids a visible scar improving cosmesis, (2) it requires nonextensive flap dissection to access the anatomical workspace, (3) it allows direct access to both thyroid lobes, (4) it avoids transection of the platysma muscle with the potential pain reduction, (5) it does not require any additional or special devices other than the common laparoscopic instruments, and finally (6) it provides magnification of the surgical field by means of the endoscopic optical equipment.
On the contrary, the technique has its limitations. The main disadvantage, at least at the beginning of the learning curve is that the visualization and dissection from top to down necessary in the TOETVA technique is different from the standard approach (lateral vision) and therefore most surgeons are unfamiliar with this new technique. The workspace with this technique is also limited, it requires CO2 insufflation and the proximity between the labial incisions restricts the mobility of the trocars.
Two existing comparative studies between the conventional open approach and TOETVA have been published by the same group.17,18 The first study, compared 216 patients in both TOETVA and standard group using a propensity score pairing. Anuwong's cohort included patients with benign and malignant thyroid disease with heterogeneity in the type of thyroid resection. Results showed a longer operative time for the endoscopic technique in contrast to the open procedure for both hemithyroidectomy (78.6 ± 20.8 vs. 64.2 ± 20.7 minutes, respectively) and total thyroidectomy (135.1 ± 37.6 vs. 103.3 ± 23.9 minutes, respectively). In addition, pain on the first, second, and third postoperative day was lower in the endoscopic than in the open group (1.1 ± 1.1 vs. 2.8 ± 1.2 points, respectively). There were no statistically significant differences between both groups in terms of complication rates. In the second study, only patients undergoing total thyroidectomy for Graves' disease were included. Results were consistent with the previous study. Operative time was longer in the TOETVA group with less postoperative pain and similar complication rate.
Three systematic reviews have been also published.19,20 The first two are difficult to interpret because a cohort of patients treated with the sublingual transoral approach 21 was also included. In the third systematic review performed by Chen et al., 22 11 publications (7 case series, 2 randomized clinical trials, and 2 retrospective cohorts) of TOETVA were analyzed. Their findings pointed out that the endoscopic approach required longer operative times, but it was associated with less postoperative pain and a similar rate of complications. The findings led the authors to conclude that TOETVA compared favorably with the standard approach.
A common question when a new procedure is added to the surgical armamentarium is the number of surgical procedures that are required to complete the learning curve. Razavi et al. 23 found that after 11 cases, both the operative time reached a plateau and the number of complications and the length of hospital stay were similar to those of open lobectomy, when the procedure was performed by a surgeon with experience in thyroid surgery. Qu et al. 24 from the analysis of 2 surgeons with experience in endoscopic surgery who performed both, total thyroidectomy and lobectomy, found that operative time became stable after 20 procedures.
As aforementioned, one of our patients developed a surgical site infection, requiring re-intervention for drainage, irrigation, and drain placement, and proper antibiotic therapy. As well known, TOETVA should be considered a clean-contaminated procedure, therefore it would be expected that despite the use of appropriate antibiotic prophylaxis, a small number of infections may occur. The prophylactic antibiotics strategies in the published literature range from a 2-day intravenous (IV) antibiotic scheme recommended by Chai et al. 25 to an extended period of oral antibiotics after the IV regimen, suggested by Anuwong et al. 17 and Dionigi et al. 26 Guidelines for antibiotic usage will be developed as more experience is gained in this field.
Contrasting with our postoperative complication rate that was relatively high, we were not able to demonstrate any mathematical differences between both groups, although this could represent clearly a Type II error. As a consequence, our series most probably represents our learning curve that may explain longer operative times and higher complication rates. However, it also behaves as a proof-of-concept demonstrating the feasibility and safety of TOETVA in our population.
In conclusion, TOETVA is a feasible and relatively safe surgical technique in patients treated for benign and malignant thyroid tumors. However, a steep learning curve is necessary to reach similar results than the standard technique. Endoscopic magnification of the surgical field and the limited surgical space compared with other endoscopic techniques might in the near future reduce complication rates, postoperative pain, and surgical time.
Footnotes
Disclosure Statement
No competing financial interest exists.
Funding Information
No funding was received for this article.