
Abstract
Background:
Endoscopic intervention through the natural foramen is becoming more and more interesting because of surgical treatment without any incision of the skin. In our center, transoral endoscopic thyroid surgery through vestibular approach (TOETVA) thyroid surgery may provide excellent results from a cosmetic viewpoint, which requires a learning curve. Generally, learning curve research for TOETVA could be benefit for investigating the surgical outcome for thyroid operation.
Methods:
This retrospective study investigated 204 consecutive patients, who underwent TOETVA performed by a single thyroid surgeon from November 2014 to June 2017. We divided the patients into hemithyroidectomy and total thyroidectomy, benign and malignant group. These groups were analyzed in terms of cut-suture time (CST) and cumulative sum (CUSUM) analysis, while accompanied with patient characteristics, perioperative clinical results, and operation-related complications.
Results and Conclusions:
The average CST of 204 cases was 147.99 ± 43.67 minutes. We observed that TOETVA enables a rapidly decreasing mean operative time after 40–50 cases to reach stabilized CST. Also, we compared the learning curve and CUSUM of the hemithyroidectomy and total thyroidectomy group, benign and malignant group, respectively.
Introduction
As with other cancers, the primary goal for thyroid cancer treatment is complete malignant lesion removal; complete surgical resection is the basic principle. In recent decades, thyroid cancer was proven as an excellent prognosis compared with other cancers, and for this reason, there is substantial interest in its treatment as well as in the quality of life, especially cosmetic result. Endoscopic neck surgery was first described by Gagner in 2001, 1 which avoids a 4–6 cm or even longer incision in the neck area after traditional surgery. Endoscopic thyroidectomy and robotic thyroidectomy (the da Vinci surgical system) allow surgeons to remove a thyroid tumor from a remote site, while providing excellent results from a cosmetic viewpoint.2,3 In our center, we carry out endoscopy thyroidectomy through breast approach since 2006. 4
However, some women were resistant to any little incisions on the anterior chest. Also, for the reason of sternum and clavicular obstruction, breast approach is more difficult to clean the lower central compartment lymph nodes. As a result, NOTES (Natural Orifice Transluminal Endoscopic Surgery) approaches through oral cavity may act as the prime solution for advanced scarless thyroid operation. Until now, TOETVA was commonly recognized as NOTES approaches for thyroid treatment. While one of the reasons for the initial obstacle is the technical difficulty of endoscopic resection that requires adequate experience both in open and endoscopic procedures, this study sought to evaluate the learning curve for TOETVA thyroidectomy performed in our department to better illuminate the practice process for transoral thyroid surgery.
Methods
Patient
From November 2014 to June 2017, 206 consecutive cases suffering from thyroid nodule receiving TOETVA at the department of thyroid surgery of the Second Affiliated Hospital, Zhejiang University College of Medicine, were enrolled. Among them, two cases were excluded from the group because of temporary transit open surgery for the reason of incredible unexpected tumor size and tracheal invasion, respectively.
All data for this study were collected from a prospective database approved by the Ethics Committee of Second Affiliated Hospital, Zhejiang University College of Medicine. The clinic pathological data for the patients including age, gender, tumor size, pathologic reports, cut-suture time (CST), postoperative Hospital stay, lymph node metastasis, and drainage was collected here. All the patients expected the cosmetic result of the neck and chose this procedure as their preferred surgical method and signed the surgery informed consent form before operation following Chinese thyroid operation guideline.
Operation indications were as follows: (1) benign nodules (solid portion) ≤6.0 cm on the largest diameter, (2) differentiated thyroid cancer, T1–T2 (tumor size ≤3.0 cm), and (3) lymph node metastasis: N0 or N1a without distant metastasis. Exclusion criteria were as follows: (1) nodules (>2 cm) in the upper pole of thyroid, (2) history of neck or oral surgery, and (3) grade III thyroid enlargement. All patients were accomplished by a single surgeon.
Operation procedure
In our previous report, we have demonstrated the operation procedure in our center. 5 Here, brief surgical procedure was illustrated. Under general anesthesia with oral intubation, the patient was in a supine position with neck extension. The oral cavity was rinsed thoroughly twice with povidone-iodine (PVP-I). Approximately 50 mL of expanded fluid (1:500,000 diluted adrenaline solution) was administered subcutaneously into the subplatysmal space until the anterior neck. The 10 mm incision was made in the center of the oral vestibule with the assistance of a suspension system, and a 10 mm threaded trocar was prepared for 30° endoscopy use. Another two 5 mm trocars were inserted at the level of the first premolars on both sides pointing down to the anterior neck. CO2 was insufflated and maintained at a pressure of 6 mmHg. Then the flap was dissected and lifted to expand the space by a suspension device (Fig. 1a). Thyroid dissection was implemented by tracing the direction of recurrent laryngeal nerve (RLN) carefully, while preserving the parathyroid glands in situ. The gland was removed and taken out in the specimen bag, and the ipsilateral central neck dissection (CND) that was performed in that case was considered to be a malignant tumour by FNA preoperation or frozen section intraoperation. A slender and porous drainage tube was placed beside the trachea. Then the linea alba cervicalis and the incisions in the mouth were closed (Fig. 1b–d).
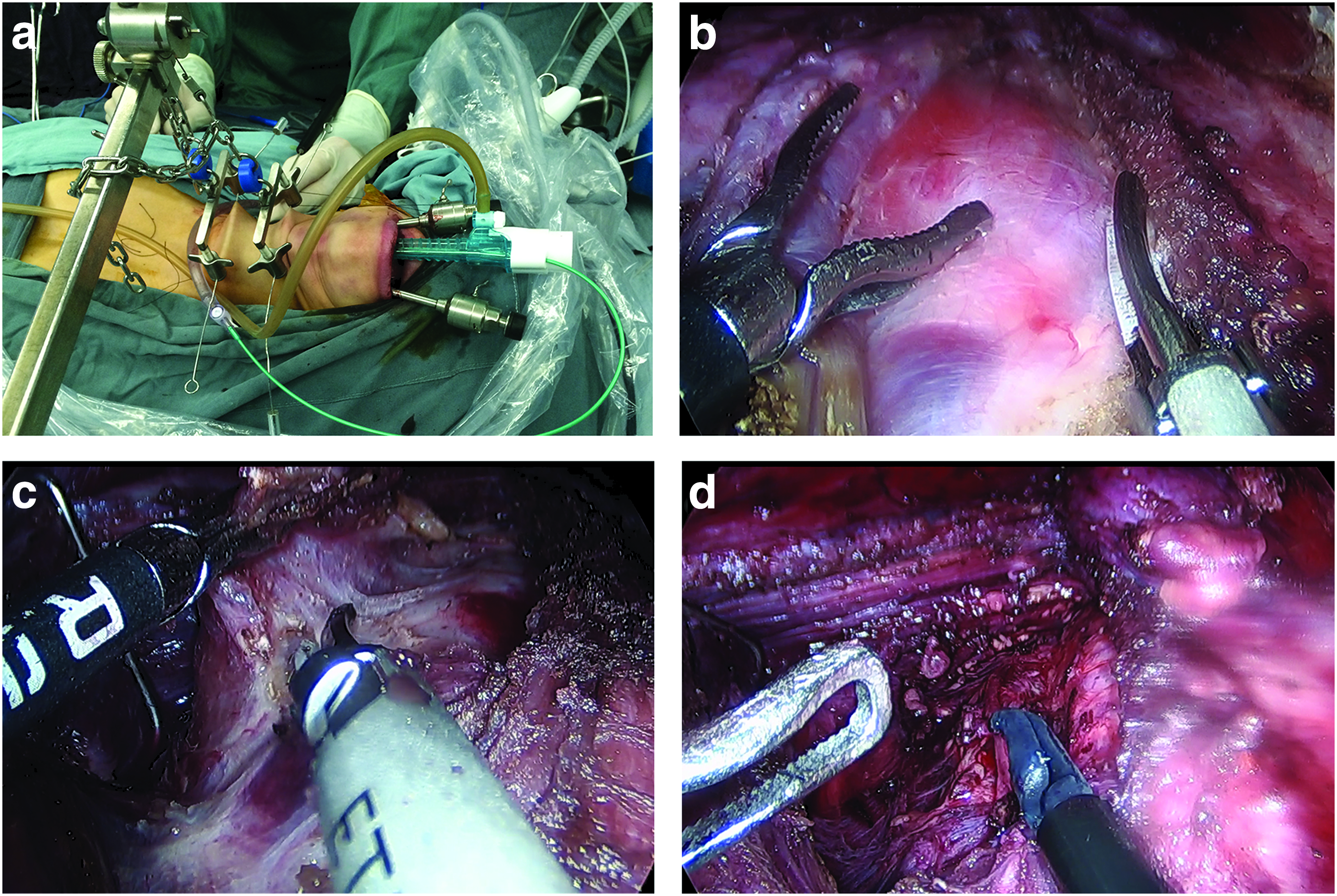
Patient position and the endoscopic view of the operation procedure.
Cumulative sum analysis
The composition total of differences between the CST data point and the mean CST represents the CUSUM. All cases were evaluated by CST using CUSUM method and ordered with chronological order to calculate the CUSUM. To calculate the CUSUM, the cases were ordered in sequence. The CUSUM of the first case is the difference between the CST of the first case and the total average CST. The CUSUM of the later case was the previous case's CUSUM plus the difference between the next case CST and the total mean CST. The process was continued to the CUSUM for the last case as in previous study. 6
Postoperation follow-up and statistical analysis
The TOETVA was compared in terms of demographics, pathological features, operative outcomes, number of inadvertently excised parathyroid glands, and perioperative complications, including postoperative bleeding, infection, seroma, and vocal cord palsy. We assessed the incidence of postoperative seroma and hematomas for at least 2 weeks after operation. Operating time was defined from mucosa incision to closure interval. The drainage volume was summarized 3 postoperative days, and the drain was removed if less than 20 mL was collected during 24 hours. Vocal cord mobility was assessed with laryngoscopic examination preoperatively and postoperatively. Statistical analyses were carried out using SPSS 17.0 (SPSS Inc. Released 2008. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.), with Fisher's exact test or Chi-square test conducted for categorical variables and two-sample t-test or Mann–Whitney test applied for continuous variables; P < .05 was regarded as statistically significant.
Result
Patient characteristics and pathological findings
Two hundred four patients were included, who underwent the TOETVA as shown in (Table 1). There were 152 cases of lobectomy and 52 cases of total thyroidectomy. Among the 204 cases, the average age was 31.48 ± 7.66 years in total. Eighteen patients were male and 186 patients were female. Average CST was 147.99 ± 43.67 minutes. Regarding the transoral surgery patients, average postoperative hospital stay was 3.3 ± 0.76 days with 159 papillary thyroid carcinoma (PTC), 35 thyroid goiter, 5 adenoma cases, 4 Hüthle tumor cases, and 1 Grade II thyroid enlargement hyperthyroidism with thyroid nodule. The total drainage volume was 135.9 ± 63.5 mL, whereas the first 24-hour take-up was larger than 60 mL. Approximately 35.7% (10/28) total thyroidectomy patients had the complication of transient parathyroid gland dysfunction (parathyroid hormone [PTH] <15.00 mM, low PTH reference limit in our hospital) after thyroidectomy surgery. Although most of the patients recovered within 2 months, 1 patient became permanently hypocalcemic with low PTH levels, requiring long-term calcium maintenance. Three patients suffered from transient superior laryngeal nerve (SLN) injury and one patient had transient mental nerve injury, which were completely recovered after 3 months. Six patients (2.9%) had slight hoarseness after transoral thyroid surgery and 4 patients recovered within 2 months; another 2 patients remain with permanent RLN lesion. There was no case of RLN resection-induced dyspnea or tracheotomy (Table 1).
Patient Characteristics
PTC, papillary thyroid carcinoma; PTH, parathyroid hormone; RLN, recurrent laryngeal nerve.
Learning curves for the TOETVA approaches
Transoral operation was performed by a single high-volume (>1000) operation number surgeon in conventional thyroid surgery and breast approach endoscopic surgery. We analyzed the learning curves for the TOETVA approaches in hemithyroidectomy group and total thyroidectomy group together with malignant or benign group. At the first 15–20 cases, we mainly chose benign and hemithyroidectomy carcinoma patient with low complication risk. To analyze CST transfer, we used the moving average curve method. First, a total of 204 cases were listed; generally speaking, the CST significantly decreased from the 40th to 50th surgical operation for TOETVA and the CST steadied after 100 cases (Fig. 2a, b).
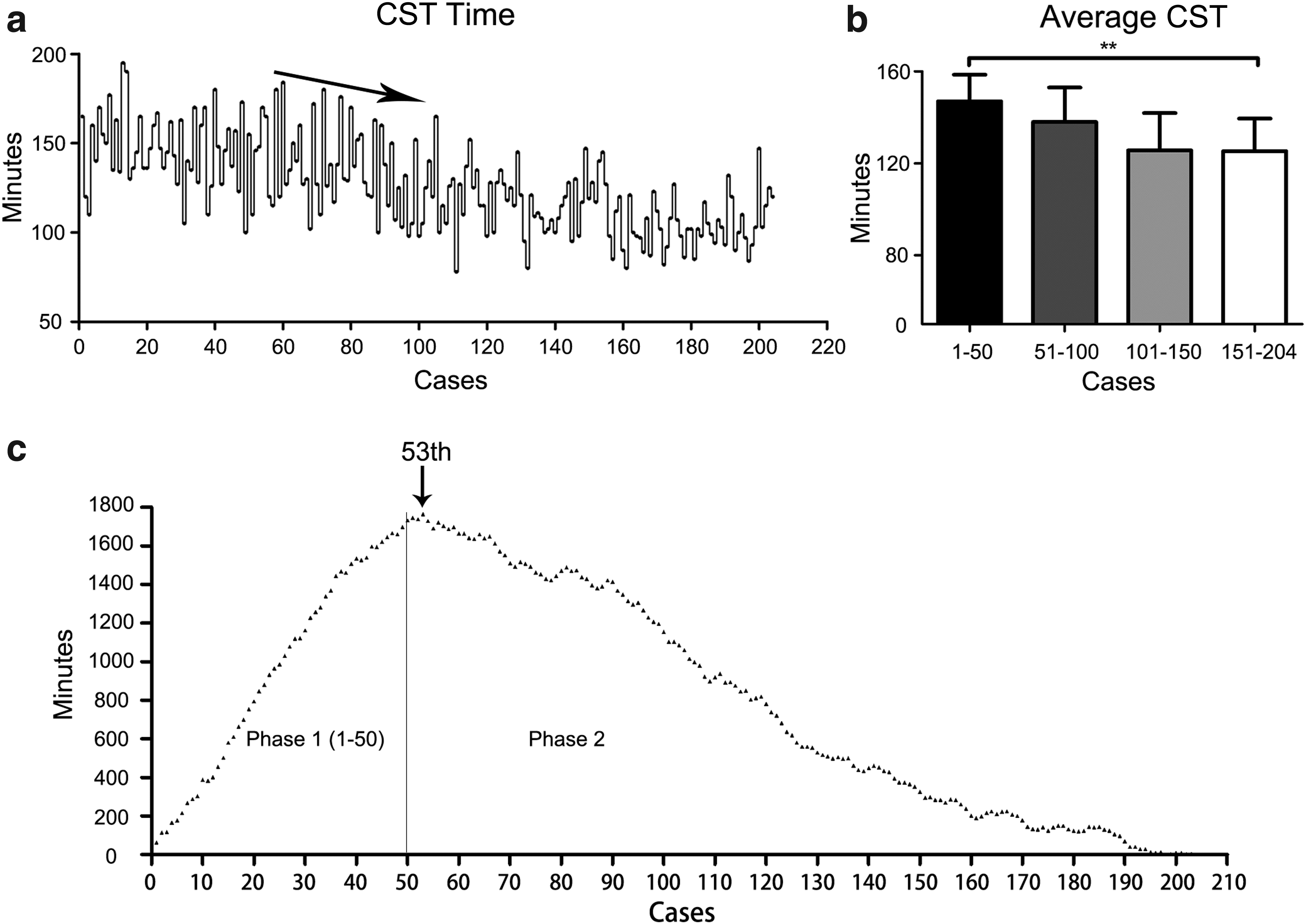
Cut-suture time and CUSUM analysis.
On the other hand, based on the CUSUM analysis, the CUSUM value reached the maximum turning point at 53rd case. Also, a comparison between phase 1 (1–50 case) and phase 2 (51–204 case) was made; a significant reduction in average CST was found between phase 1 (181.4 minutes) and phase 2 (135.5 minutes; P < .0001) average CST. The slope remained smooth, which stands for relatively steady CST in the phase 2 period (Fig. 2c). Next, we try to better demonstrate the variety of operative scheme. In our study, we divided the patients into distinct operation groups. Among them, 176 hemithyroidectomy (141.2 ± 27.4 minutes) and 28 total or subtotal thyroidectomy (178.3 ± 33.7 minutes) patients, 45 benign (129.1 ± 32.8 minutes) patients, and 159 thyroid cancer (153.3 ± 31.7 minutes) patients were included. For hemithyroidectomy, the surgical time decreased from the 20th operation and plateaued at ∼130–160 minutes (Fig. 3). Similar to hemithyroidectomy surgery, the surgical time for total thyroidectomy decreased approximately in the 10th case since we have overcome the difficulty point during the initial exploration of few cases with benign nodule and microcarcinoma, and an approximately plateaued 150–180 minute CST was in need. Similarly, we found ∼20–30 cases were in need to reach the initial learning stage in malignant and benign tumor group, while more fluctuation was found in malignant thyroid cancer operation because of additional unilateral or bilateral lymph node dissection procedure (Fig. 3b). Also, the lines of best linear fit for the four groups CUSUM CST learning curves are shown in (Fig. 4). Obviously, the slope of benign tumor group (Y = 15.75 × ) was relatively lower than the other group. It can be concluded that benign tumor operation was recommended for beginner in the initial learning curve period. The CST and amount of drainage gradually decreased with increasing surgical experience. Also, all complications, especially parathyroid gland hypofunction in total thyroidectomy and RLN lesion, show a relatively low and scattered incidence tendency for both the initial 50 cases and the latter case under our careful operation. At last, we analyzed some factors concerned with surgery difficulties and CST. It was found that Hashimoto thyroiditis, male patient, and right tumor location with right CND slightly increase the CST, while large tumor diameter (>1 cm) shows no influence on CST (Fig. 5).
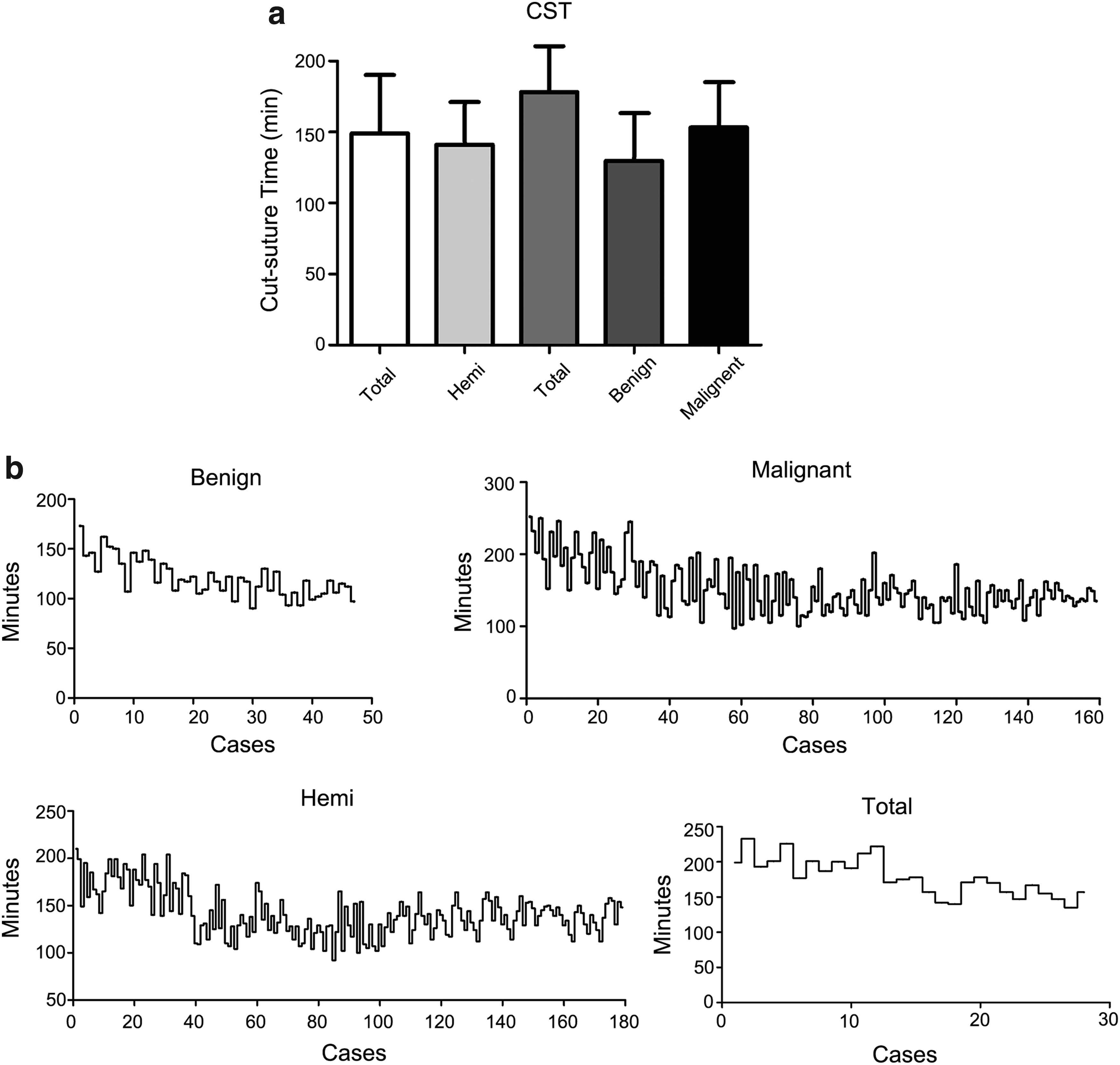
Learning curve for subgroup operation method.
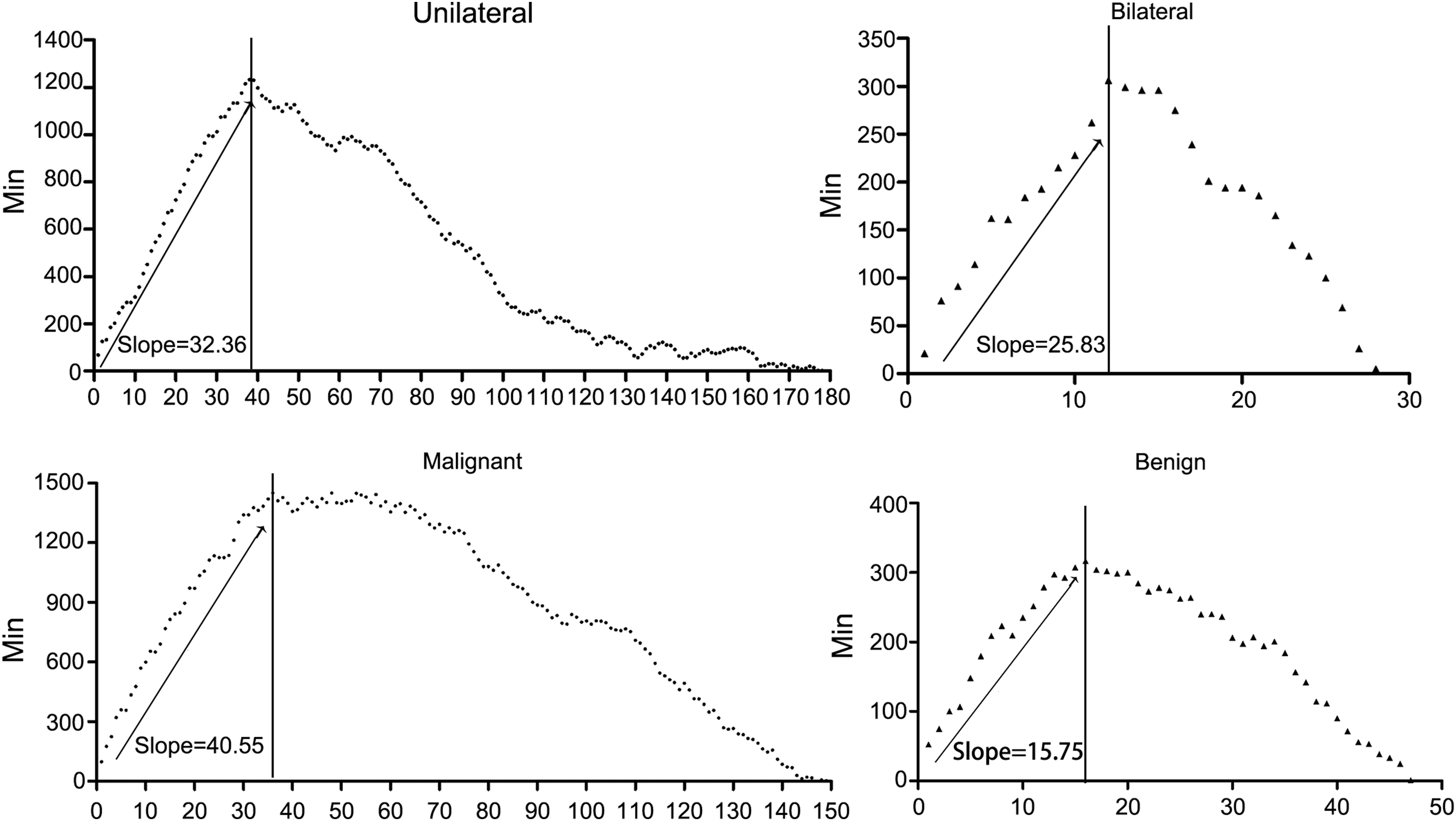
CUSUM cut-suture time of benign, malignant, unilateral, and bilateral thyroidectomy operation.
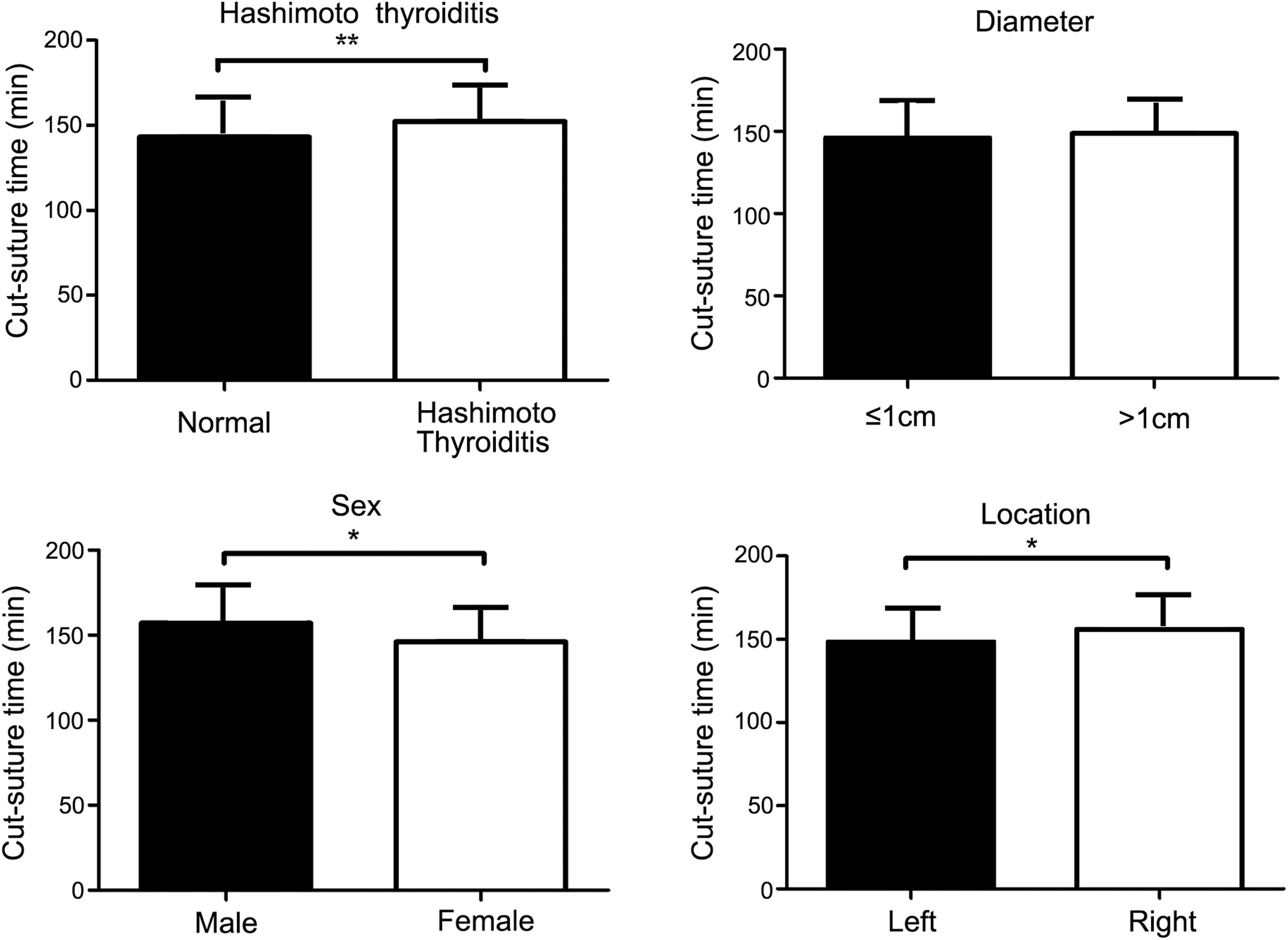
Cut-suture time influence factors: Hashimoto thyroiditis, tumor diameter, sex, and tumor location. *P < 0.05; **P < 0.01.
Discussion
As endoscopy with minimally invasive operation for thyroid cancer treatment is becoming more popular.7–9 Since transoral thyroidectomy was performed into clinical use since 2009, 10 the operation skill required to manage transoral thyroidectomy seems to be the main obstacle for surgeries. To the best of our knowledge, this is the first study to demonstrate the learning curve for the TOETVA with a single thyroid surgeon.
In general, thyroidectomy procedure was composed of several steps such as working space creation, thyroid dissection, RLN and parathyroid recognition and protection, specimen removal, and so on. Usually, oral working space preparation takes up over 30% CST for less experienced surgeons. The working space respects natural anatomical surgical planes, which avoid dermatological and platysma dissociation that minimized surgical trauma and decreased the probability of neck discomfort after surgery. The initial tunnel was performed by the usage of a traditional dissection stick for blunt dissection. During operation, one 10 mm incision and bilateral 5 mm incisions were localized between the center of oral vestibule and premolar, respectively. Expanded fluid was administered subcutaneously into the subplatysmal space until the anterior neck as previously reported. 5 Correct isolation layer is the first obstacle during TOETVA; less experienced surgeons usually suffer from misidentification of platysma and sternocleidomastoid. Particularly, in male patients, prominent thyroid cartilage may be considered a further difficulty in the achievement of the thyroid boundary. Under this condition, it is time taking to protect epidermis in case of piercing, which may easily lead to deep isolation of operation space. As a result, anterior cervical vein injury and muscle hemorrhage exudation lead to blurred vision, which influences surgical field; additional management of bleeding vessel significantly increased CST. At the same time, the vestibular approach exposes the patient to the possible injury of the mental nerve (MN), which is a sensory nerve that provides sensation to front of the chin area.11–14 During our early phase operative, individual patients sometimes call for decreased sensation of the lower lip, which correlates with MN lesion. Thereafter, the lateral vestibular incision was carried out relatively high at premolar level. In this condition, we chose an entrance route between the camera monitor and the clamp which slightly increased the operation difficulty for the chopsticks effect. However with skill accumulation, it is feasible to overcome this difficulty after the learning curve. After which, ∼20 minutes is enough to dissociate linea alba cervicalis and expose the thyroid gland.
One of the most common complication after thyroid surgery is RLN injury, after the midline linea alba cervicalis separation and the deep fascia; by hanging suture, strap muscles are retracted laterally. Generally, visual identification of RLN is considered the gold standard in prevention of nerve injury. In transoral procedure, the exposure and anatomy of the RLN were craniocaudal. Causally, for beginners, the inverse presentation causes difficulty to manage the upper pole and RLN laryx entry point attached to tracheal and cricothyroid surface. Through our experience, cutting the inferior thyroid artery and vein should be performed close to the gland to avoid nerve injury. Also, we were the first to report a clinical application of IONM in transoral endoscopic thyroid surgery. 5 The major advantage of implementing IONM in TOETVA is to identify RLN and confirm its integrity. IONM has been proven to be effective and widely used in traditional open thyroid surgery. In this study, we developed a vestibular approach for thyroidectomy with CND and successfully performed IONM to explore and identify RLN. Careful separation between superior thyroid and trachea in learn curve until complete RLN is identified is recommended. In 204 cases, preoperation hoarseness was found in 6 patients, while 2 patients (<1%) experienced permanent RLN palsy identified by postoperation laryngoscope observation; the complication incidence was not higher than traditional open thyroidectomy based on previous report. 15 Although IOMN technique is still controversial and needs modification in preventing RLN complications, we began to implement this technique since the 40th case from August 2015. Before the implementation, identification of RLN from vessel was the main obstacle in operation. In our experience, we found the postoperation hoarseness most probably happened before IONM implementation, despite no statistics significant for incidence and case number limitation. More importantly, it was beneficial to affirm uninjured RLN function, which could avoid bilateral RLN signal loss. On another aspect, persistent RLN monitoring gives surgeons significant information at the RLN “signaling lost” point, which helps to shorten the learning curve of TOETVA. Although SLN injury happened less compared with RLN injury, it can never be ignored. In our study, three patients suffered from transient SLN injury postoperatively; at the beginning, we were not precise enough in identifying the superior pole of thyroid and handling the superior thyroid artery not close to the superior pole. After the initial case experience, SLN injury did not happen afterward.
For a transoral procedure to gain universal acceptance, the intrinsic goal of the treatment should not be compromised in pursuit of less invasive surgery. Recurrence and complication rates should be at least comparable with those of conventional surgery and the procedure should take additional benefits to patients for cosmetic results. The training is a crucial step, while gaining any video-assisted surgical technique, and it should be defined in detail to exploit it completely.
After training, with improvement of operation skills and clean dissection, a shorter and more stable CST was reached for transoral thyroidectomy operations. However, there is possible bias regarding the endoscopic thyroidectomy experience. In our center, surgeons had performed traditional thyroidectomy for several years and then began with the breast approach endoscopic thyroidectomy. In accordance with CST, the amount of drainage follows a similar learning curve for transoral approaches. Although not reported before, we observed a confused anatomy layer dissection during the early learning period of endoscopic surgery because the surgeon was unfamiliar with the surgical anatomy and wide exposure was mandatory. After learning curve, the precise facial cleft dissection avoids tissue contusion, which might be the reason for decreased drainage.
A learning curve for a specific surgical procedure can be defined as the number of cases needed before the operative time and complication rate are stabilized and minimized. However, more detailed definition is needed based on the development of different operation styles. The learning curve should take into account the appropriateness of the chosen operation indications, efficiency of the procedure steps, quality of the manipulation, recovery of the patient, and quality of postoperative life. Our study is limited in this regard as our main interest was regarding the learning curve concern about CST. Generally, ∼40–50 cases are needed for an experienced thyroid surgeon to reach a stabilized transoral operation procedure and 100 cases to reach the proficient skilled level based on our experience. Also, we recommend that less experienced surgeons start with lobectomy for benign nodule or hemithyroidectomy for early-phase PTC in case of severe complications. On the other hand, Hashimoto's thyroiditis and male patients would increase the operation difficulty. Beginner was proposed to avoid these characteristic patients in first dozens of cases for surgical safety guarantee. For another, right tumor location (posterior recurrent laryngeal CND in needs) would increase the CST. We suggest less experienced surgeons dissect the posterior and anterior lymph node, respectively, rather than en bloc procedure resection.
In addition, the main surgeon in our study had large volume of breast approach endoscopic and open thyroidectomy experience before initiating the transoral approach. This prior experience could have affected the period needed for TOETVA stabilization.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Zhejiang Provincial Basic Public Welfare Project (grant numbers: LGF18H160002).