
Abstract
Introduction:
The safe introduction of transanal total mesorectal excision (taTME) has been documented by the Australasian group previously. The most important prognostic indicator for rectal cancer is the ability to achieve a clear resection margin. By utilizing false planes for taTME surgery, the endopelvic fascia and or presacral fascia can be resected en bloc.
Technique:
This case highlights the utilization of a taTME platform to perform a distal taTME with presacral fascial stripping and a lateral pelvic sidewall transanal-assisted dissection in a 53-year-old otherwise healthy woman with a mid-rectal tumor. Radiologically the tumor was staged as a T3c/T4 rectal cancer with an N1c deposit extending beyond mesorectal fascia abutting the left piriformis muscle. An extramural venous invasion positive tumor was evident with a positive circumferential resection margin at 4 o’ clock. In addition, the taTME platform was used to allow transanal intraoperative radiotherapy (IORT) delivery to the sacrum. An R0 resection was achieved and the patient recovered well without incident.
Results:
Total operative time was 250 minutes with the patient being discharged on day 7 postoperatively without complication. Macroscopic evaluation revealed a grade III mesorectal excision with en bloc removal of presacral fascia. On microscopic evaluation, revealed a T3N1b tumor with 2 of 14 positive lymph nodes (0/5 pelvic sidewall nodes).
Conclusion:
The case highlights a novel application of taTME and is to the authors' best knowledge the first described use of a transanal platform to deliver intraoperative radiation therapy in the literature.
Introduction
Locally advanced rectal cancer can be challenging and requires a combination of highly specialized and uniform imaging (particularly magnetic resonance imaging [MRI]), judicious use of neoadjuvant chemoradiotherapy, and a clear operative plan and execution to maximize the chance of cure. 1 Although all the separate components are equally important in achieving a good outcome, the risk of a close or involved margin is of particular importance. The beyond total mesorectal excision (TME) and PelveX collaborative highlight the importance of extended resections and removing contiguous organs where necessary to achieve an R0 resection margin.2–4 In some cases, the removal of the contiguous organ can be associated with increased morbidity. Furthermore, in cases of a potentially positive margin in a fixed bony location, additional boost radiation therapy can be delivered at the time of surgery to reduce the local relapse risk. 5
Transanal TME (taTME) surgery is an effective technique that has been continuously refined for the past decade for distal rectal dissection in select patients with challenging anatomical and tumor characteristics.6–9 It has been safely introduced and adopted into Australasia as highlighted by the current group previously.10,11 By utilizing false planes for taTME surgery the endopelvic fascia and or presacral fascia can be removed en bloc allowing extended resection. The authors also believe that in select cases, the R1 risk point is best seen transanally, and have published on this concept previously. 12
This article describes the novel utilization of taTME platform to assist with a lateral pelvic sidewall dissection en bloc as well as facilitating presacral fascial resection to avoid the potential risk of an R1 resection as this is better visualized from a “bottom-up approach” and describes the first use of intraoperative radiotherapy (IORT) utilizing a taTME platform and thus negating the need for a laparotomy in the medical literature.
Case description
A 53-year-old (body mass index 26) otherwise well woman presented with a 5-month history of right-sided abdominal pain and intermittent low volume hematochezia. Blood panels revealed a microcytic anemia. At endoscopy, a gastroscopy highlighted inactive gastritis with her colonoscopy demonstrating a 7 cm near circumferential posterior-based rectal cancer. After biopsy, this was revealed to be mismatch proficient and initial staging imaging revealed a locally advanced rectal cancer without distant metastatic disease. In particular, on MRI imaging a T3c/T4 rectal cancer, extramural venous invasion (EMVI) positive tumor was seen with a positive circumferential resection margin at 4 o’ clock.
After completion of standard neoadjuvant chemoradiation, the patient was restaged at 5 weeks in accordance with institutional protocols with a fluorodeoxyglucose-positron emission tomography-computed tomography and MRI scan of the pelvis. The MRI scan revealed an enlarged N1c deposit with left piriformis as well as presacral fascial involvement. Minimal response was noted radiologically and at both the multidisciplinary meeting and preoperative planning meeting a decision was to offer a combined laparoscopic ultralow anterior resection with left pelvic sidewall clearance and a taTME approach to aid en bloc resection of the presacral fascia and intraoperative radiotherapy delivery.
Materials and Methods
Transabdominal phase
The procedure was performed 8 weeks after completion of chemoradiation and was commenced as a synchronous two team Cecil approach. 13 The abdominal phase (previously described 12 ) involved medial to lateral mobilization of the sigmoid and left colon, including complete mobilization of the splenic flexure with proximal ligation of the inferior mesenteric artery and vein. Both vessels were controlled with haemolocs. The left ureter was visualized and preserved. Ensuring adequate mobilization of the left colon, pelvic dissection was commenced with preservation of the sympathetic nerve plexus.
The standard TME plane was initially found and then after minimal dissection caudally the left hypogastric nerve was divided with a Thunderbeat energy device, Olympus®. The presacral fascia was entered abdominally and subsequent caudal dissection was continued cautiously (one view from above). The lateral pelvic sidewall on the left was taken en bloc with medialization of the left ureter after dividing the ureterohypogastric fascia down to the vesicoureteric junction with identification and dissection of the external iliac vein and the psoas major muscle. The medial clearance included dissection of the anterior internal iliac branches. The left lateral pelvic sidewall dissection was also facilitated by the transanal phase.
Transanal phase
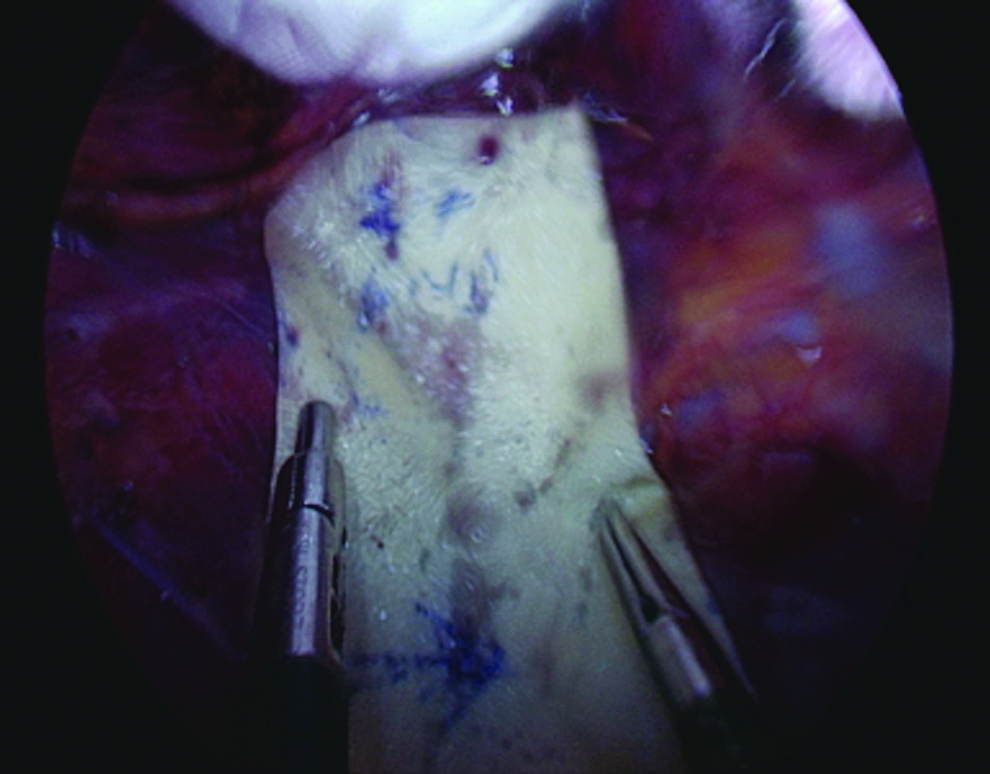
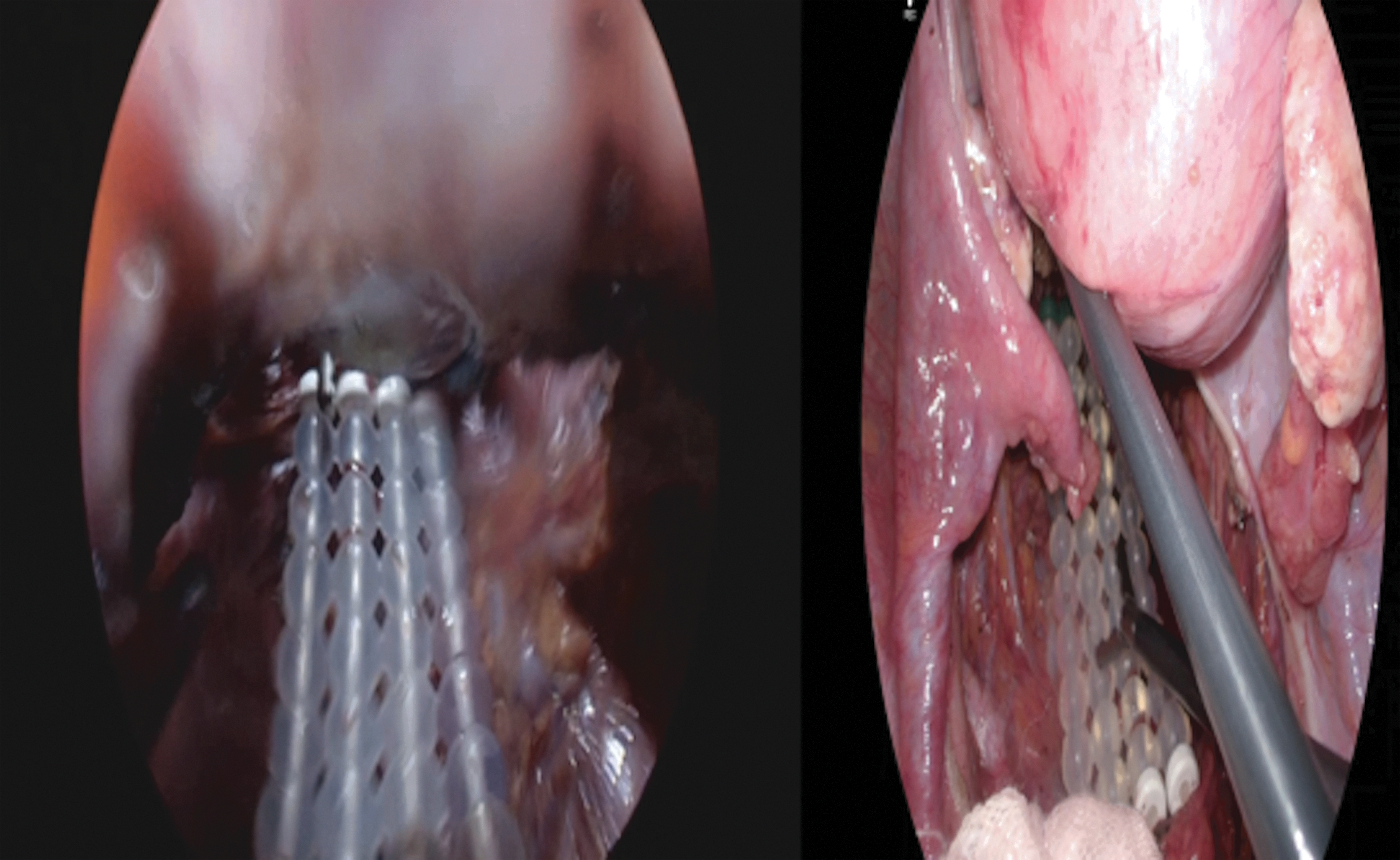
The taTME setup was performed synchronously with the patient in a Trendelenburg position (Supplementary Fig. S1). A Lone star retractor (Cooper Surgical) was applied allowing eversion of the anoderm. The GelPOINT® Path (Applied Medical) was placed in the anal canal and thoroughly washed with copious cidicidal wash. A gauze was placed in the anus. A clockwise 1–0 prolene suture with a 26 mm rounded needle was used inside the GelPOINT Path device to ensure an airtight seal at the distal margin. Three ports were used to facilitate the dissection and an AirSeal® System (CONMED) used to help with pneumoinsufflation. Incremental increases in pressure are used according to the potential space created from 5 to 12 mmHg. An articulating single incision laparoscopy hook diathermy was used for dissection. After a circumferential rectotomy at 1 cm above dentate line, the dissection was continued cranially above the extrafascial plane and was continued above the endopelvic fascia for 2–3 cm until a decision was made to dissect through posteriorly. This enabled the surgeons to utilize a false plane to selectively remove the endopelvic fascia. The continuation of the false plane cranially allowed for easy removal of the presacral fascia and a relatively prompt rendezvous point (Fig. 1). The left pelvic sidewall dissection was then facilitated transanally as the left lateral dissection allows easy access to the piriformis and obturator internus muscles. Removal of the obturator lymphatic tissue was performed and the dissection was continued to clear the lymphatic tissue lateral to the medial umbilical artery (Fig. 2). Throughout the pelvic dissection there was concurrent dissection with continuous focused communication from both primary surgeon's (abdominal and transanal primary operators) concentrating on the area of potential R1 margin risk and lateral sidewall dissection (Fig. 3 and 4). After completion of the synchronous resection the specimen was extracted transanally through the GelPoint Path port and divided proximal to the IMA and reduced back into the abdomen to facilitate IORT delivery.
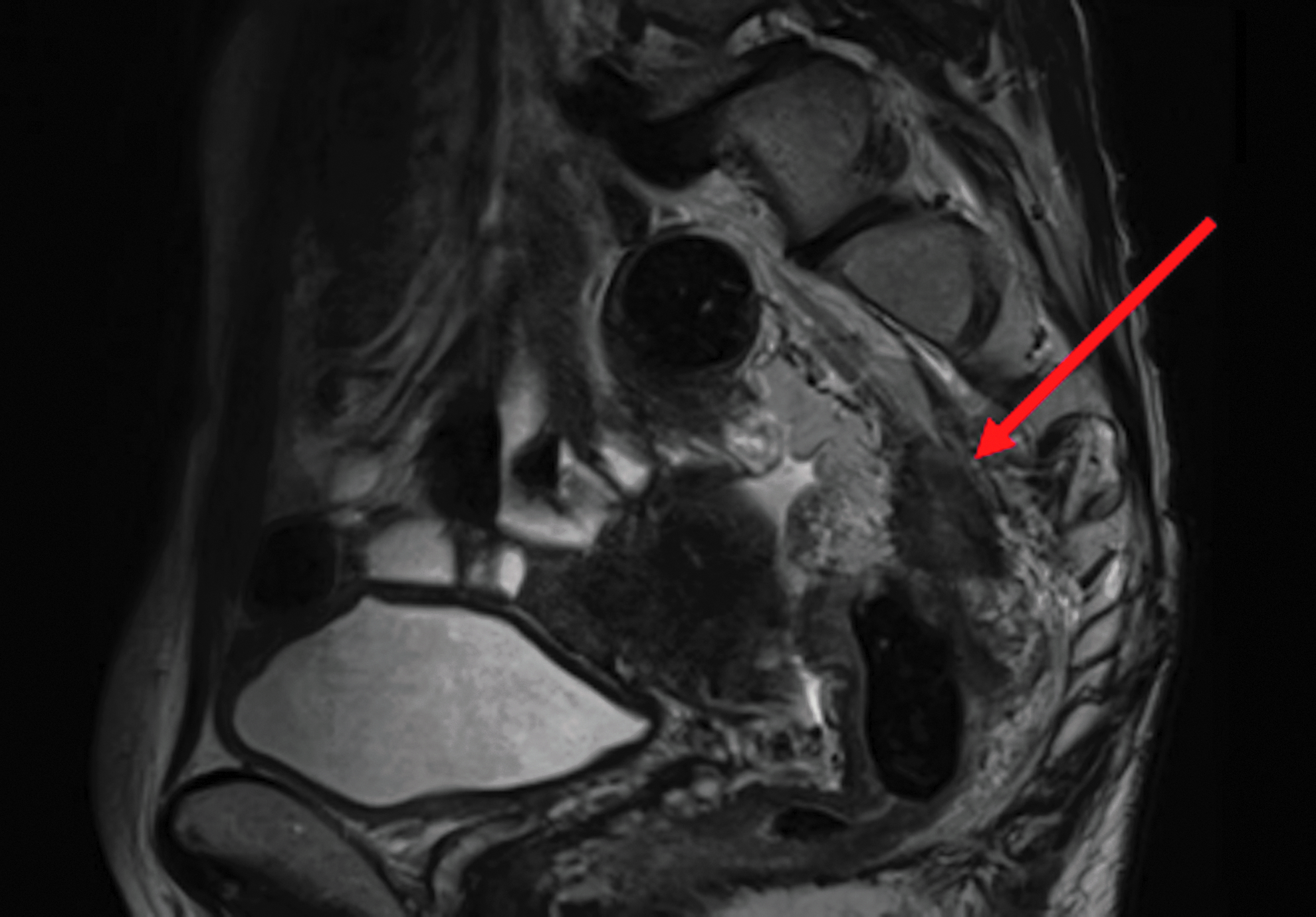
Postchemoradiation restaging MRI (T2 weighted imaging) sagittal section showing a large posterior mesorectal node with involvement of the presacral fascia (red arrow). MRI, magnetic resonance imaging.
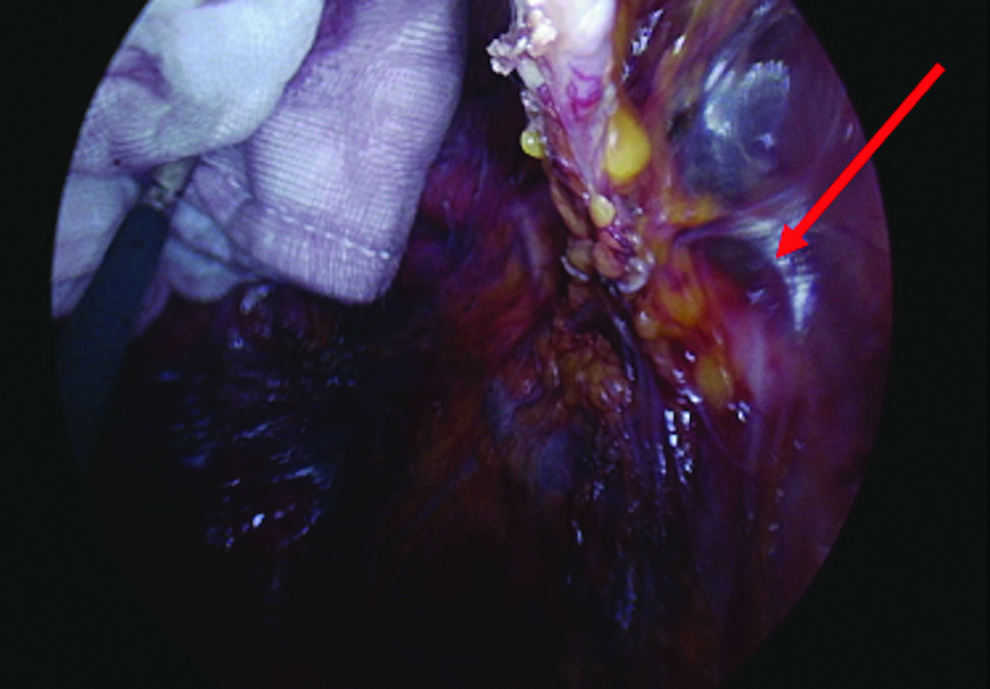
Transanal view of the left obturator internus and the lateral sidewall. The red arrow shows clear abutment and/or involvement of the presacral fascia on restating MRI scans.
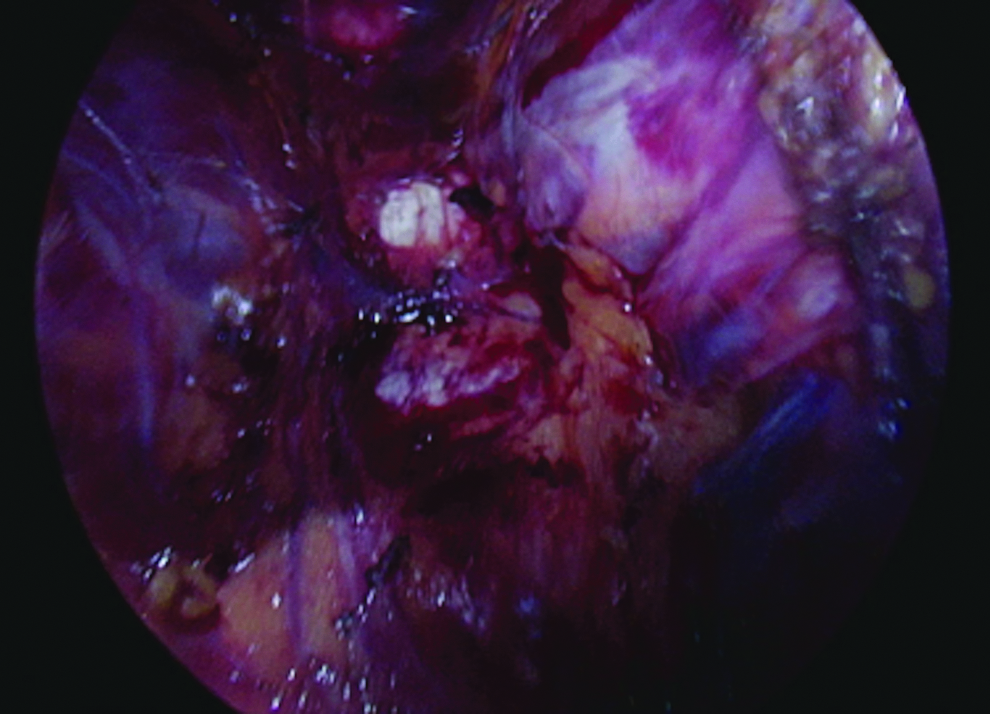
Presacral fascia removal at the site of the presacral node.
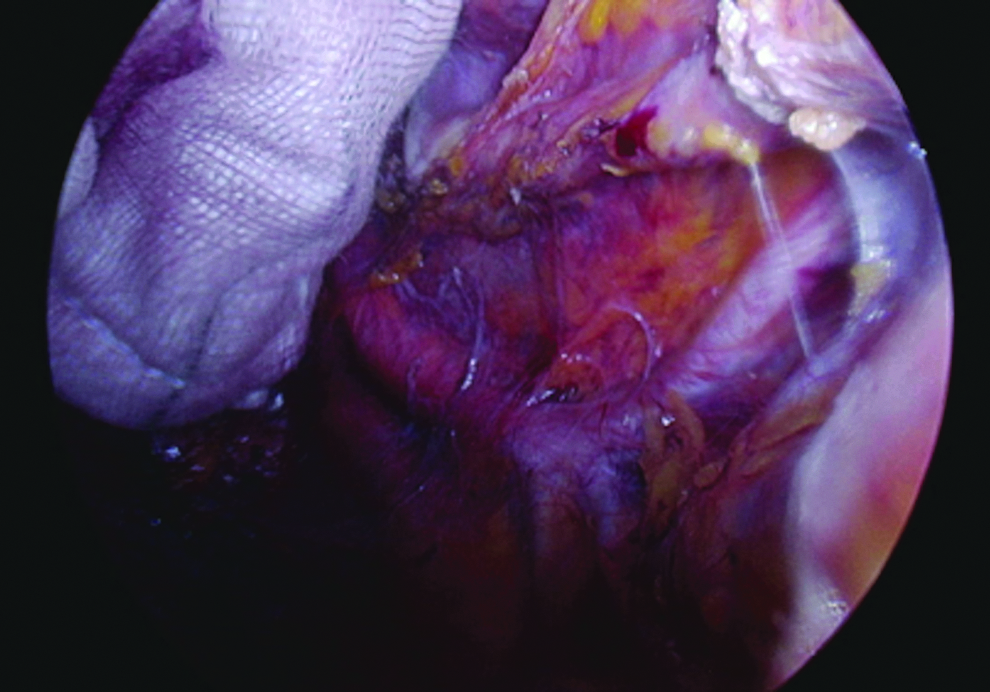
Transanal view of left pelvic sidewall after taTME-assisted resection. taTME, transanal total mesorectal excision.
Transanal intraoperative radiation therapy
Copious amounts of cytocidal agents were used transanally and hemostasis was fully achieved. The brachytherapy sizer planning pad was delivered through the transanal platform and placed into the space posteriorly (Fig. 5). After this, the appropriately sized brachytherapy beads were constructed and placed transanally (Fig. 6). Surgical gauze packs were used to protect the ureters and the small bowel from the radiation field. 10 Gy of additional boost radiation therapy for 30 minutes was delivered safely through the transanal platform using the Elekta flexitron® brachytherapy system. Finally, an end-to-end anastomosis was performed through the transanal platform using a 33 mm ethicon circular stapler, with excellent donuts, good blood supply, and a fully intact staple line circumferentially. Four × 3-2-0 polydioxanone sutures were placed at each quadrant transanally to the circumferential suture line. A defunctioning loop ileostomy was fashioned as standard and a 12F drain placed into the pelvis.
IORT sizer placed transanally. Packs delivered up into the abdomen transanally before transanal sizing for IORT. IORT, intraoperative radiotherapy.
Intraoperative visualization of brachytherapy beads placed transanally and manipulated laparoscopically.
Results
Total operative time was 250 minutes with the patient discharged on day 7 postoperatively.
Pathology
Macroscopic evaluation revealed a grade III mesorectal excision with en bloc removal of the presacral fascia. On microscopic evaluation, a T3N1b tumor was diagnosed with 2 of 14 positive mesorectal lymph nodes with no lateral pelvic sidewall nodal involvement (0 of 5 pelvic sidewall lymph nodes). The proximal and distal resection margins were clear of malignancy and the potential site of R1 margin was 1.5 mm clear. Lymphvascular invasion and EMVI were present. DNA mismatch repair immmunohistochemistry revealed normal pattern of staining of MLH1, MSH2, MSH6, and PMS 2.
Discussion
The current case highlights the importance of using a synchronous abdominal and transanal approach to achieve an R0 resection in a patient with a locally advanced rectal cancer with presacral fascial involvement. The presacral fascia is resected en bloc by extending the application of taTME with the selective utilization of “false” planes. To the authors' best knowledge this case describes the first use of brachytherapy/IORT delivery using this platform in the literature.
Beyond the normal taTME plane, planned false dissection planes can be utilized to help achieve an R0 resection. In this case the presacral fascia is selectively removed from the sacrum and hence the S2,3 periosteum is seen. This case again highlights that the R1 risk point of a tumor can be best seen transanally in selected cases. We have published on this concept previously. 12 The taTME platform also assisted in both the left-sided lymph node clearance as well as the delivery of additional radiation therapy to sterilize the R1 risk point site despite an R0 resection being achieved.
The authors do not advocate that all surgeons should utilize this technique for T4 tumors but demonstrate that in select cases that the technique can be safely deployed to achieve an R0 result. Meticulous preoperative planning, thorough evaluation of preoperative imaging, and having an experienced team are the keys to achieve a successful outcome. In this particular case, the primary surgeons were advanced high-volume exenterative surgeons (S.K.W., A.G.H., and J.J.M.) and run Australasian courses and are proctors for taTME (S.K.W. and A.G.H.).
It would recommend that such approaches are performed in specialist high-volume rectal cancer centers where the appropriate expertise exists to deliver such care.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.