
Abstract
Background:
Although minimally invasive pancreatic necrosectomy (MIPN) is a new invasive technique for necrotizing pancreatitis, it has some disadvantages. This study aimed to improve the debridement technique with an ultrasonic pressure ballistic system. We hypothesized that this system would facilitate debridement and improve the safety of the procedure.
Materials and Methods:
Between October 2016 and January 2019, 5 patients diagnosed with necrotizing pancreatitis were enrolled in the clinical cohort. All patients underwent debridement due to infective necrosis. Access for debridement was typically established with percutaneous puncture. Then MIPN was performed. During the procedure, ultrasonic pressure was applied to liquefy the necrotic material and make it absorbable. The effect of debridement was assessed by analyzing the average bleeding volume, operation time, and complications. Postoperative clinical parameters were evaluated.
Results:
Debridement was performed successfully for all patients. Semisolid necrotic tissue was dissolved with ultrasonic pressure. Viscous pus was rapidly aspirated with the suction applied with negative pressure, which greatly enhanced efficiency. This approach enhanced the visibility of blood vessels, which improved safety. No major complications were encountered. Two patients (40%) developed puncture site infections. The average blood loss during the operation was 13 ± 6 mL. The average operation time was 78 ± 31 minutes. Postoperative APACHE II scores were significantly lower than preoperative scores (P < .05). White blood cells, C-reactive protein, and procalcitonin levels declined postoperatively.
Conclusions:
The ultrasonic pressure ballistic system could potentially enhance MIPN and make it safer.
Introduction
Acute pancreatitis is a very common disease. It is responsible for a large volume of hospital admissions and a high cost burden.1,2 Its severe form, necrotizing pancreatitis, has the most dreadful course, sometimes with a fatal prognosis. Infected necrosis is associated with high rates of morbidity and mortality.3–5 Necrotizing pancreatitis is characterized by infected necrosis in and around the pancreas. Therefore, necrosis debridement is necessary to stop the infection. 6 Conventionally, open surgery has had limited effects, and it is associated with various complications.7,8 With the recent advent of minimally invasive techniques, including endoscopic, interventional, and surgical procedures, the outcome has greatly improved.9–12
Among the various minimally invasive techniques available, minimally invasive pancreatic necrosectomy (MIPN) is a good approach for accessing necrotic material.13,14 Most MIPN requires flushing with water; however, necrotic tissues often consist of viscous fluids and pliable semisolid material; consequently, necrotic material cannot be easy to remove. Moreover, it is difficult to visualize blood vessels clearly enough to distinguish them from adjacent purulent necrosis.15,16 Considering these characteristics of necrotic material, in this study, we describe a new technique that can dissolve necrotic tissue and avoid damage to blood vessels; this approach utilizes an ultrasonic pressure ballistic system.17,18 This system facilitated the absorption of necrotic material, improved the safety of the procedure, and greatly enhanced debridement.
In this study, we describe 5 patients who underwent MIPN with the aid of an ultrasound pressure system. This system significantly accelerated the efficiency and effect of debridement. Moreover, blood vessels could be readily detected, which increased the safety of this interventional procedure.
To the best of our knowledge, this study was the first to report the use of an ultrasonic pressure ballistic system for performing MIPN and to describe its overt advantages.
Materials and Methods
Patients
Between October 2016 and January 2019, 5 patients diagnosed with necrotizing pancreatitis were enrolled into the clinical cohort. This trial was approved by the internal review board of our hospital. All patients diagnosed with infected necrotizing pancreatitis were included. The basic diagnostic criteria were severe acute abdominal pain, fever, serum amylase elevated more than threefold, and computed tomography (CT) findings of pancreatic enlargement. CT images also showed peripancreatic necrosis, with accumulated fluid in the peripancreatic space. Exclusion criteria were a lack of clinical data; previous pancreatic surgery; severe heart, liver, or kidney dysfunction; coagulation dysfunction, and so on.
Of about 96 patients diagnosed with acute pancreatitis in our center, only 5 cases (1 men, 4 women; mean age 62 years; range 45–80 years) were eligible for this study. Thus, the incidence of severe infected necrotic pancreatitis was about 5.2%. Demographic and baseline characteristics are summarized in Table 1. All patients were routinely treated for acute pancreatitis and infection.
Patient Information Summation
Establishing debridement access
Access for debridement was typically established with percutaneous puncture. CT scans showed peripancreatic abscess formations, which often occurred in the retroperitoneal space. Ultrasound was used to determine the puncture site and route of entry. A 6–8F tube was inserted into the retroperitoneal necrotic space. Fluid excretion through the tube indicated puncture success. The fluid drainage gradually decreased. After 3–5 days, a sinus could be formed, which provided access for debridement. Occasionally, a laparotomy was performed to cure the emergent etiology of pancreatitis, such as clearing stones in the biliary tract. During the operation, drainage tubes were placed around the pancreas. These drainage tubes provided access to the site for debridement when a peripancreatic necrotic abscess had formed. In consideration of this scenario, the tubes should be placed as close as possible to the pancreas.
Debridement procedure
Four weeks after admission, MIPN was performed. In brief, the drainage tube was removed, and initially with a guidewire, the sinus was gradually enlarged from a small to large opening (i.e., from 6F to 24F; Fig. 1A). During the debridement, an Electro Medical Systems (EMS) ultrasonic pressure system was used to liquefy the necrotic material, which made it more absorbable with flushing water (See Supplementary Video S1, Pancreatic Necrosectomy assisted with an ultrasonic pressure ballistic system). The pressure for the ultrasonic fluid irrigated at was 12 kPa. After absorption, the remaining pliable fibrous necrotic tissue was removed with a grasping forceps (Fig. 1B).
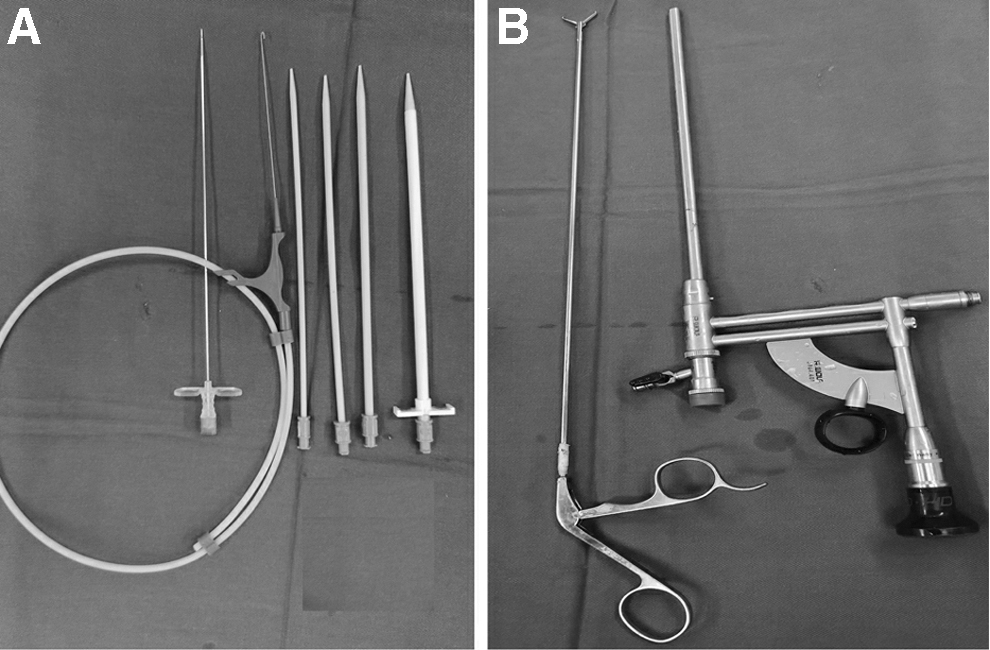
Tools used in debridement.
After debridement, access was maintained by placing a double-lumen drainage tube, which can be used to irrigate and drain simultaneously. After 2 weeks, CT was again performed to evaluate the infection focus. Depending on the condition of the patient, another MIPN might be planned.
Clinical parameters
We recorded the average bleeding volume and operation time. Complications were analyzed, such as bleeding, visceral injury, and wound infection. The effect of drainage after the operation was evaluated. We determined the APACHE II score and other inflammatory parameters19–21 to evaluate each patient's condition before the operation and 1, 3, and 7 days after the operation. Two weeks after the operation, another CT scan was performed.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation, and comparisons were evaluated with the Mann–Whitney U test. P values <.05 were considered significant. Categorical statistics are presented as the number (%). All statistical analyses were performed with SPSS® version 20 software (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.).
Results
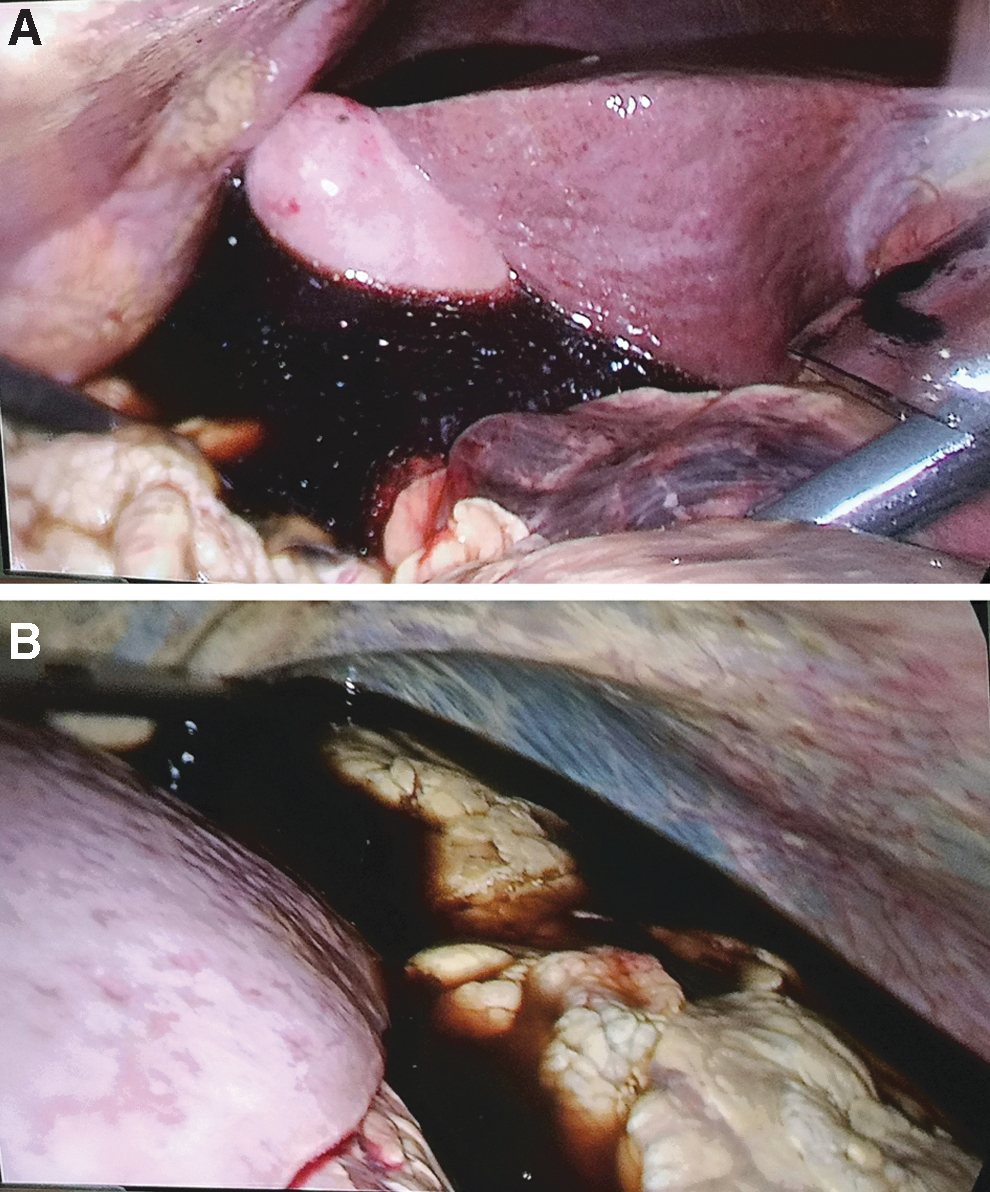
The debridement operation was successfully performed for all 5 patients. Access was established with ultrasound-guided percutaneous puncture into the necrotic space. One patient was laparoscopically converted to laparotomy. This patient was admitted with a diagnosis of biliary pancreatitis. A perforated gallbladder was suspected, due to the development of a serious acute abdomen and abundant peritoneal effusion (Fig. 2). During the operation, a large volume of effusion was drained, a stone was removed from the bile duct, and a T drainage tube was placed. The peripancreatic space showed no fluid accumulation; only two drainage tubes were placed above and in front of the pancreas. Four weeks later, the peripancreatic space harbored accumulated inflammatory necrotic material, and the peripancreatic drainage tubes were removed to gain access for debridement.
After access was established, the nephroscope was placed. Then, ultrasound pressure was applied to emulsify and dissolve the semisolid necrotic tissue (Fig. 3A). The necrotic tissue became liquefied, which greatly facilitated absorption. Viscous pus was rapidly aspirated with the negative pressure suction system of the EMS apparatus (Fig. 3B), which greatly enhanced efficiency. After the pus was aspirated, very little pliable fibrous tissue remained. Clamps were used to loosen and grasp necrotic tissue for removal (Fig. 3C).

Importantly, this EMS ultrasound system was safe. It revealed the blood vessels, and damage could be avoided (Fig. 3D). When the local abscess wall appeared pink, debridement was stopped. No active hemorrhage ensured, the dilator was removed, and a drainage tube was inserted along the sinus tract. No severe complications occurred, including major bleeding and visceral injury. Only 2 patients (40%) developed puncture site infections. These features are shown in Table 1.
The average amount of bleeding during the operation was 13 ± 6 mL. The average operation time was 78 ± 31 minutes (Table 1). Postoperative APACHE II scores were significantly lower than preoperative scores (P < .05), and the APACHE II scores gradually declined at 3 and 7 days postoperatively. White blood cells, C-reactive protein, and procalcitonin also declined postoperatively. After 2 weeks, some patients experienced recurrent necrotic infections, and another MIPN was performed. For these patients, debridement was performed one to three times.
Two weeks later, CT scans were conducted. Most images showed the collapse of the abscess. Fluid accumulation in the peripancreatic space was substantially reduced (Fig. 4). When a drainage tube was in place and the abscess had collapsed, clear draining fluid indicated that the necrotic infection was effectively controlled. At this time, the tube was gradually withdrawn and the patient healed. The patient with pancreatitis caused by choledochal cyst stones underwent a choledochal cyst excision and choledochojejunostomy 3 months later.

Fluid accumulation substantially reducing before
Discussion
MIPN is one of most commonly used minimally invasive clinical techniques. The application of MIPN in patients with acute necrotizing pancreatitis infections has achieved remarkable results. In this study, we developed a new method for facilitating this technique. The EMS ultrasonic pressure ballistic system greatly increased the efficiency and safety of debridement.
In pancreatic necrosis, necrotic tissue typically accumulates around the pancreas. Over time, a discrete wall is gradually formed. 22 Within the wall, a large volume of necrotic tissue accumulates. When this tissue gets infected, a pancreatic abscess forms. The abscess consists of fluid and more solid material. Moreover, blood vessels and myenteric tissue are involved. These tissues are relatively pliable and tough, and thus, they are very difficult to convert to fluid. 23 Consequently, it is difficult to clear necrotic tissues.
In this study, we developed a creative system for clearing necrosis. We applied a pneumatic ultrasonic endoscopic lithotripter (EMS-IV). 24 This system was initially developed by EMS (a Swiss company) to facilitate lithotripsy for removing urolithiases. 25 It comprises a highly effective ultrasonic pressure system, which can drive energy generated by compressed gas. This pneumatic ballistic energy liquefies solid and semisolid materials to render them absorbable. Moreover, this ultrasound device was combined with a suction system. This combined system could remove pus very effectively. 26 In addition, the EMS ultrasound system was safe. The pneumatic pressure ballistic technology did not require energy conversion, and it produced little heat. The amplitude before and after impact did not exceed 2 mm. The mucosa only sustained a slight transient injury, slight edema, and minimal bleeding; thus, the system did not incur long-term damage.27,28 Moreover, it rendered blood vessels clearly visible and reduced intraoperative bleeding; in particular, major hemorrhages could be avoided. The separated fibrous tissues could be grasped rapidly, which could shorten the operation time.
Typically, this technique can reduce the occurrence of postoperative complications. In this study, we encountered only slight complications, such as wound site infections. The efficiency of this method was greatly enhanced by the complete removal of pancreatic necrosis tissue. Thus, the frequency of repeated MIPN was reduced, and operation times were shortened. Complete safe debridement created favorable conditions for patient recovery.
We should pay special attention to the etiology of necrotizing pancreatitis. Unlike in western countries, in our country, pancreatitis is often caused by acute biliary disorders.29,30 Importantly, biliary obstructions can lead to critical outcomes. However, due to the poor condition of patients, endoscopic retrograde cholangiopancreatography (ERCP) is the preferred treatment.31,32 Nevertheless, we showed that, for the patient in our series, laparotomy was the treatment of choice for alleviating biliary obstructions, particularly in patients with large effusions. This approach facilitated the proper placement of drainage tubes to ensure adequate drainage. This method showed good results, and it improved the efficiency and safety of debridement surgery.
The main study limitation was the small number of patients in this case series. In future, more procedures should be performed to gain experience with this method.
Conclusions
MIPN has been widely used for treating necrotizing pancreatitis. We preliminarily demonstrated that the EMS ultrasonic pressure ballistic system remarkably improved the effects of this invasive technique. It made necrotic material more absorbable and blood vessels were clearly visible, which greatly improved the efficiency and safety of debridement. This technique is currently in the exploratory stage, and there is room for technological improvement; thus, more experience and study are needed to establish the efficacy of this procedure.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.