
Abstract
Aim of the Study:
Esophageal dilatations are commonly performed in pediatric patients who have undergone an esophageal atresia/tracheoesophageal fistula (EA/TEF) repair or following caustic injury. We sought to compare the practice of esophageal dilatation across different specialties.
Methods:
We analyzed all patients who had an esophageal dilatation at our center between April 2014 and December 2018. Patients were identified via prospectively maintained databases and clinical coding records. Patients had a combination of dilatations under each specialty: interventional radiology (IR), surgery, and gastroenterology.
Results:
Thirty-five individual patients underwent 226 dilatations, median dilatations per patient was 3 (1–40). The median age at first dilatation was 18 months (1–194 months). Sixty-eight percent of patients had a previous EA/TEF repair. IR performed 59% of dilatations, surgeons 26%, and 15% by gastroenterologists. Surgeons more frequently were performing initial dilatations (P < .05) and performed more dilatations in EA/TEF patients (P < .0001). There was a significant difference between the time from a surgical dilatation until the next dilatation, 3.7 months, compared with an IR dilatation, 1.8 months (ANOVA, P < .05). Surgeons more frequently increased the size of balloon used (57% versus 33% versus 39%, P < .01). There was no significant difference in balloon size between specialties or in the incremental increase in size between subsequent dilatations. There was one postprocedure perforation, managed conservatively (complication rate = 0.4%).
Conclusion:
We have demonstrated that on average, patients wait longer after a surgical dilatation until their next procedure, and surgical teams are more likely to increase the size of the dilating balloon. Surgeons tend to be more involved in their postoperative patients in the initial phases of stricture management. Our results suggest the feasibility and safety of a multispecialty approach for these patients.
Introduction
Pediatric esophageal strictures are most commonly encountered in children following esophageal atresia (EA) repair, or in those who have sustained caustic ingestion injuries. For such children, they are often a long-term source of morbidity and frequently require multiple interventions to improve their symptoms.
Even in expert hands, strictures at the site of esophageal anastomosis following surgery for EA are not uncommon, cited as symptomatic in more than one third of patients presenting with symptoms to clinic 1 but seen in more than 60% of patients on barium swallow assessment. 2 There are a number of factors known to influence the risk of stricture formation, and careful attention to anastomotic integrity as well as aggressive management of gastroesophageal reflux disease have been thought to reduce the risk. 3 Caustic ingestion is another common indication for stricture dilatation, and a recent study has indicated that it represents an underappreciated global health burden. 4
Patients with esophageal stricture may require extensive treatment over many years to manage their symptoms, and the majority of patients with stricture will undergo dilatation, which has been shown to manage symptoms effectively. 5 Previously, strictures were treated with dilatation with rigid bougie; however, management has generally moved forward to balloon dilatation, with the theory that the radial force applied may reduce the risk of esophageal damage and stricture recurrence. 6
Historically, management of postoperative strictures following EA repair was performed by the operating surgeon. More recently, patients with other disease etiology such as inflammatory or reflux-related strictures have been referred to gastroenterology services, and interventional radiology (IR) services have expanded in pediatric practice. These changes have led to a cross-specialty management of esophageal stricture emerging in our center, as with many others.
Previous studies have analyzed single-center outcomes for dilatations in EA.5,7–10 However, to the best of our knowledge, no previous article has studied if there is a difference in practice or outcomes between IR, surgery, and gastroenterology.
Methods
Pediatric patients undergoing esophageal dilatation at our center between April 2014 and December 2018 were identified via retrospective analysis of prospectively maintained databases and clinical coding records. Graded esophageal dilatations were performed with the use of appropriate balloon catheter sizes for the patient's weight, age, and stricture severity. The size of the balloon used was up to the discretion of the attending clinician. The balloon catheter was inserted across the stricture after placement of a guidewire under either fluoroscopic or endoscopic guidance and inflated using a radiopaque contrast material, and obliteration of the “waist” on fluoroscopy was deemed to indicate successful dilatation. In patients in whom esophageal injury was suspected (i.e., blood noted on the balloon), a postdilatation contrast study was performed to assess for any evidence of esophageal perforation.
Data were collected on age at presentation, underlying diagnosis, medical specialty, balloon size, increasing size of balloon, interval to subsequent dilatation, and complications. Data are displayed as median with accompanying range, or mean with standard deviation and are denoted in the text of the results. Appropriate statistical testing of categorical data, mean comparison, and distributions were performed using a combination of GraphPad© QuickCalcs and SPSS v23.0 (IBM™).
Results
Over the 4-year study period, 35 patients were identified, and all were included with complete records. Patient diagnoses are shown in Table 1, with approximately two-thirds having had previous EA repair. Age at presentation was median 18 (1–194) months. Single strictures were found in 85%, in the proximal (31%), mid (37%), and distal (17%) esophagus, with the remaining 15% of patients presenting with multilevel disease. Of note, there were two patients presenting with type 1 achalasia cardia, one has been referred for peroral endoscopic myotomy and the other has been managed with dilatations alone and is currently symptom free and under routine follow-up.
Stricture Etiology
EA/TEF, esophageal atresia/tracheoesophageal fistula.
A total of 226 dilatations were performed. Patients underwent a median 3 (1–40) dilatations; 26/35 (74%) patients required multiple dilatations, including 17/24 (71%) patients with EA. IR were responsible for 133 (59%) dilatations, whereas surgeons performed 58 (26%) and gastroenterologists performed 35 (15%).
Each individual patient's dilatations are demonstrated in Figure 1. As is demonstrated, surgeons were more frequently involved in cases of EA versus other diagnoses (41% dilatations versus 13%, P < .0001), and correspondingly, IR and gastroenterology were more frequently involved in non-EA diagnosis patients (IR 65% versus 51%, P < .05; gastroenterology 22% versus 8%, P < .001). A surgeon most commonly performed the first dilatation in any patient compared with IR or gastroenterology (51% versus 37% versus 11%, χ2 = 8.7, P < .05). Surgeons were more likely to plan a longer interval before a subsequent dilatation compared with either IR or gastroenterology, 3.8 (7.3) months versus 1.8 (3.95) versus 1.3 (1.14) (ANOVA, P < .05).
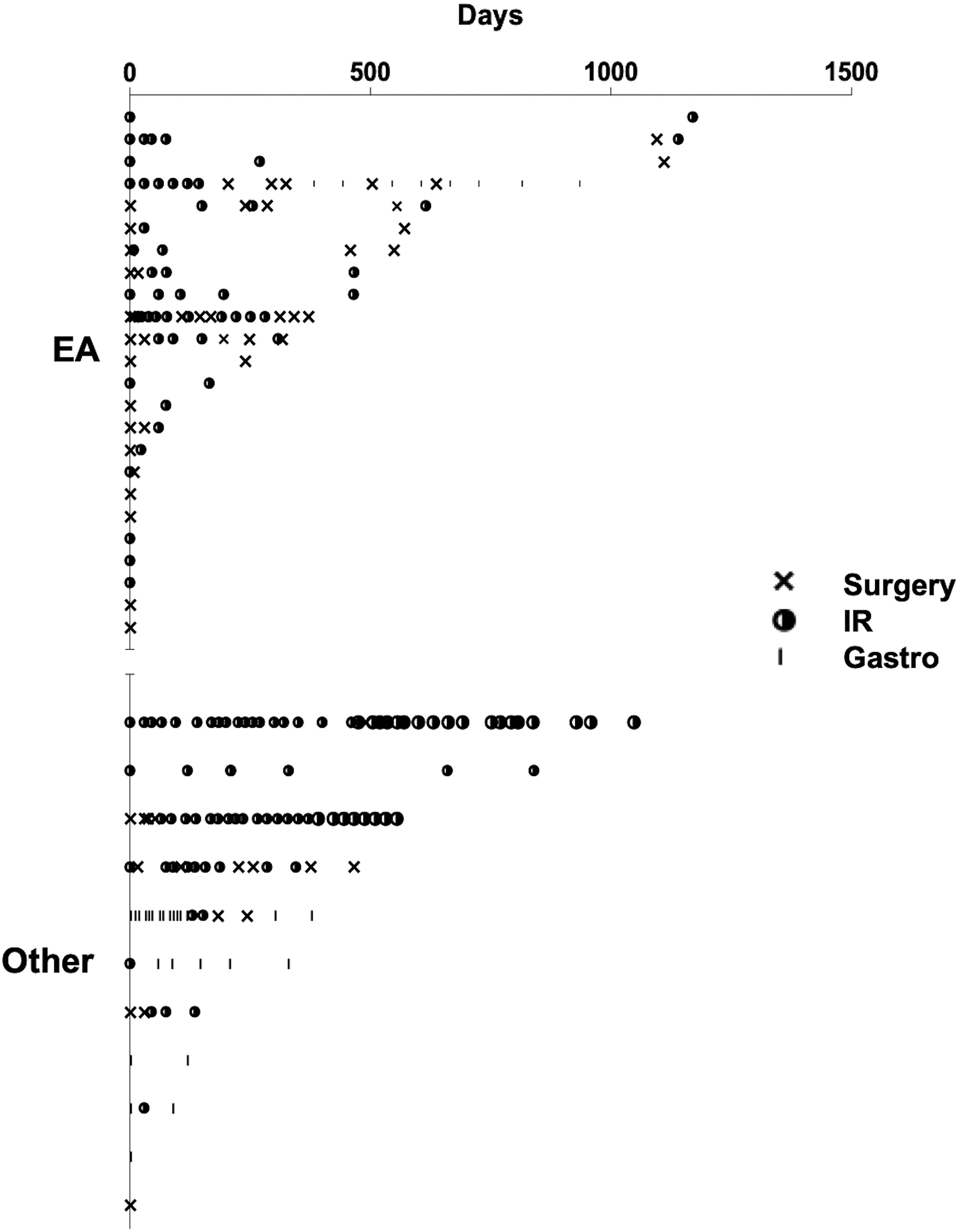
Esophageal dilatations by patient, grouped by esophageal atresia and other diagnoses. The individual dilatation protocols for each patient are demonstrated, separated into those with EA and those with other diagnoses. Surgeons tended to be involved in patients with EA more than other specialists, also tending to be performing the initial dilatations, before other specialists take over once the need for routine dilatation has been established. EA, esophageal atresia; IR, interventional radiology.
There was no significant difference in the balloon size used between specialties (Table 2); however, surgeons were more likely to progressively increase the size of balloon as shown in Table 3 (χ2 = 9.55, P < .01). In terms of complications, one patient had a radiological evidence of perforation, which was successfully managed conservatively with observation alone; therefore, our complication rate was 1/226 (0.4%).
Balloon Size Used and Increase in Balloon Size by Specialty
Dilatations with Change in Balloon Size (Increase Versus No Change/Smaller, Chi-Square = 9.55, P < .01)
IR, interventional radiology.
Discussion
We believe this to be the first study to compare the practice of pediatric esophageal dilatation across three specialty groups. We have demonstrated that division of this work within our center is a safe and feasible practice, with a complication rate that is comparable to the published literature. 11 We demonstrate a variation in practice regarding intervals between dilatations and serial increase in balloon sizes between the services at our center.
We have identified that surgeons are more likely to increase the balloon size used. The reason behind this is unclear, but capability to manage complications, alongside a more historied acquaintance with the patient and their condition may explain a more “aggressive” approach in this regard. Comparatively, interventional radiologists may be more hesitant to rapidly upscale the balloon size in surgical patients, especially if they have not previously been involved in their management.
Surgeons were also more likely to leave a longer interval before reattempting dilatation than either of the other two specialist services. We speculate that this may be a selection bias since patients requiring regular frequent dilatations are commonly referred to the IR service. Surgeons' use of a slightly smaller balloon size may be explained by the fact that they are commonly the individuals performing the initial dilatations, especially following EA repair (Fig. 1), and these patients are then referred to IR in later life. We would point out that although our case series is smaller than that of other centers reporting from within the United Kingdom,5,8 the 4-year period of data collection denotes a relatively high throughput. We believe that our multispecialty approach may allow better management of this case volume.
This study bears the limitations of its retrospective nature, and the relatively small size of the cohort may mean that the variability in practice represents variation at an individual level as opposed to between specialties per se. Our single-center data may also not be representative of the wider practice across the specialty; this may be true in fact as the rate of EA patients undergoing multiple dilatations exceeded 70% compared with approximately half of the patient series reported in other centers,5,7–9 suggesting a difference in threshold for intervention. The heterogeneous nature of this cohort may also confound our findings, as different management plans in terms of frequency and size of dilatations may be instigated for strictures of different etiologies.
Esophageal strictures are a source of significant morbidity, and as patients often require repeated procedures, timely management is critical. Our study suggests that such a multidisciplinary approach can be adopted successfully, with similar practices demonstrated between specialist teams and an overall complication rate in keeping with the published literature. We hope that this work will expand upon the existing knowledge available and help other centers to consider a cross-specialty approach in these patients.
Footnotes
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Disclosure Statement
No competing financial interests exist.
Funding Information
J.R.D. is part-funded by the NIHR Academic Clinical Fellowship Scheme through the UCL-GOS Institute of Child Health. All research at Great Ormond Street Hospital NHS Foundation Trust and UCL Great Ormond Street Institute of Child Health is made possible by the NIHR Great Ormond Street Hospital Biomedical Research Centre.