
Abstract
Background:
Can laparoscopic orchiopexy achieve a better testicular position and a higher success rate than open orchiopexy for palpable undescended testis in children? We conducted a prospective comparison study with a large volume of cases to answer this question.
Methods:
A total of 256 patients with palpable undescended testis who were admitted between January 1, 2017 and December 31, 2017 were included in this study. Among them, 124 patients underwent laparoscopic orchiopexy and 132 patients underwent open inguinal orchiopexy. The outcome evaluated index included final testicular position, success rate, and complications.
Results:
Of 256 patients, the mean age was 2.4 years; 218 patients had unilateral palpable testis, and the other 38 patients had bilateral palpable testis. There were no significant differences between laparoscopic orchiopexy group and open orchiopexy group with respect to age, side, preoperative testicular position, and testicular volume. The final testicular position in laparoscopic group was better than that in open group (lower position rate: 89.3% versus 77.9%, P = .01). There was no significant difference in success rate (laparoscopic group: 100%; and open group: 98.5%). There were 3 complications in the laparoscopic group and 6 complications in open group (P > .05). No testicular atrophy was found in either group. No testicular ascent occurred in laparoscopic group while there were 2 cases in open group, which required additional surgery for correction. Of patients who underwent surgery at the age of 3 years or older (n = 75), laparoscopic surgery was associated with markedly better testicular position than open surgery (lower position rate: 88.1% versus 69.6%, P = .03).
Conclusions:
Laparoscopic orchiopexy is associated with better testicular position and comparable success rate comparing to open orchiopexy for palpable undescended testis in children. This procedure could be recommended for palpable undescended testis, especially in older children.
Introduction
Undescended testis is one of the most common congenital abnormalities in male children, with an incidence rate of 1%.1,2 The universally accepted and recommended treatment is orchiopexy. In the past decades, open inguinal orchiopexy has been the routine procedure for palpable undescended testis, and laparoscopic orchiopexy for nonpalpable testis. However, for the high inguinal testes, the success rate of open orchiopexy usually is not satisfactory due to difficult surgical mobilization. 3 Docimo reported that success rate of open orchiopexy for high inguinal testes was only 82.3%, which was much lower than the rate for testes beyond the external ring (92.6%). 4
Recently, He et al. pioneered the approach of laparoscopic orchiopexy to treat palpable testis for 90 cases, and its success rate reached nearly 100%. 5 The advantage of laparoscopy is extensive dissection of spermatic cord in retroperitoneum, it may provide good mobilization of testis and pull it down to the bottom of scrotum. 6
Can laparoscopic orchiopexy achieve a better testicular position and a higher success rate than open orchiopexy for palpable undescended testis in children? There has been limited studies with small sample sizes and without persuadable conclusions.3,7,8 We conducted a prospective comparison study with large volume of cases to answer this question. The work evaluated final testicular position, success rate, and complications.
Materials and Methods
Study design
Patients were included if they had palpable undescended testes, and the affected testes were located in the inguinal canal. Exclusion criteria included (1) testicular position in the root of scrotum; (2) history of inguinal surgery; and (3) history of hormonal therapy.
From January 1, 2017 to December 31, 2017, 357 patients with undescended testis were admitted to our department. Among them 65 cases of nonpalpable testis and 26 cases of low undescended testis (below external ring) were excluded. Ten cases with a history of inguinal region surgery were also excluded. For the included 256 cases of inguinal palpable testes, the surgical procedures were performed per guardians' or patients' requests. A total of 124 patients underwent laparoscopic orchiopexy and 132 patients underwent open inguinal orchiopexy. The patients were followed up by outpatient clinic after discharge.
The variables for comparison included operating time, cost, success rate, complications (classified by Clavien–Dindo system), testicular volume tested by ultrasound, final testicular position, and testicular ascent. We also compared the variables in different age groups. Success was defined as proper testicular position without atrophy or ascent. Final testicular position was assessed clinically by another doctor (Jiaqiang Li) who did not perform the surgery, and classified as lower position (low scrotum) or upper position (mid scrotum or high scrotum). Low scrotal position means that the testis is in the bottom of the scrotum without tension. Postoperative testicular atrophy was defined as presence of a nubbin or impalpable testis on follow-up visit, which was confirmed by Doppler ultrasound. 9
Surgical procedure
Laparoscopic orchiopexy: All patients underwent general anesthesia in supine position with 30° elevated on the affected side. The first port for the laparoscope was placed in the umbilicus. Two 5 mm ports were introduced on either side in the lower quadrants at the level of umbilicus along the mid clavicular line (Fig. 1). During the laparoscopy, the internal ring was usually open (Fig. 2A). Peritoneum over the testicular vessel and vas deferens was incised and dissected at the level of internal inguinal ring. Releasing the testicular vessels from the peritoneum and retroperitoneum increased the length of the testicular vessels (Fig. 2B). The testis was taken to the abdominal cavity and the gubernaculum was transsectioned. The scrotal skin was incised at the bottom of scrotum and subdartos pouch was created. A laparoscopic dissector was introduced through the internal ring to the scrotum. It served as a guide to pass a forceps through the scrotum. Then, the testis was grasped at the gubernaculum by the forceps and it was pulled down to the subdartos pouch (Fig. 2C–E). Based on our experience, the testis was mobilized to the contralateral internal ring to check the tension of spermatic cord (Fig. 2F). If there was any tension on vessels, the peritoneum over the testicular vessels could be further dissected to higher level with laparoscopy (Fig. 2G). For the high position testis or short spermatic cord, the testis would be brought down through the medial side of inferior epigastric vessels (Fig. 2H), which shorten the distance from abdomen to scrotum. We did not close the ipsilateral internal hernia ring during surgery.

The trocars position for left undescended testis; (1) a 5 mm port for the laparoscope, (2, 3) two 5 mm ports for instruments.
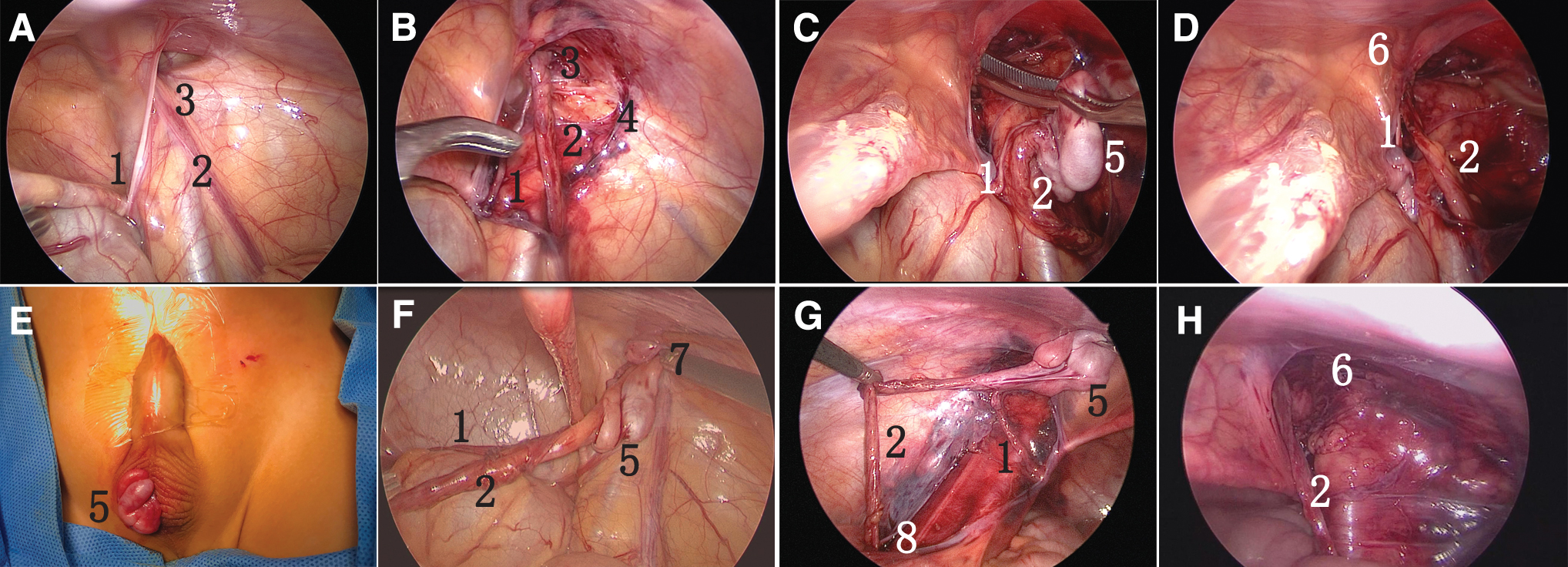
The surgical procedure of laparoscopic orchiopexy.
Institutional Review Board approval
This study was approved by the Institutional Review Board of our hospital, and informed consents were obtained from the guardians of all patients.
Statistical analyses
The comparison of continuous data was conducted with t test or covariance analysis. Categorical variables were compared with the use of chi-square test or logistic regression. All statistical analyses were performed with a two-sided significance level of 0.05 and conducted with SPSS 17.0 software.
Results
A total of 256 patients were included; 124 patients (140 testes) underwent laparoscopic orchiopexy and 132 patients (154 testes) underwent open inguinal orchiopexy. The demographic data and evaluated parameters are summarized in Table 1. The mean age was 2.4 years, ranging from 8 months to 11 years; 218 patients had unilateral palpable testis, and 38 patients had bilateral palpable testis (16 in laparoscopic orchiopexy group [LG] and 22 in open orchiopexy group [OG]). There were no significant differences between LG and OG with respect to age, side, and testicular volume. No patients converted from laparoscopic surgery to open surgery. There was no significant difference between LG and OG for operating time. In LG, we identified the contralateral inguinal hernia in 15 cases and repaired them simultaneously.
Demographic Data and Outcomes Evaluated Parameters of Laparoscopic Orchiopexy Versus Open Orchiopexy Group
The mean period of follow-up was 12 months, ranging from 11 to 14 months. During the follow-up visits 245 testes were examined to have low scrotal position, 125 in LG and 120 in OG. The final testicular position in LG was better than that in OG (lower position rate: 89.3% versus 77.9%, P = .01). No testicular atrophy was found in either group. No postoperative hydrocele or inguinal hernia was found in either group. No testicular ascent occurred in LG while there were 2 cased in OG, which required additional surgeries for correction. The success rate was 100% in LG and 98.5% in OG (2 patients with testicular ascent were considered unsuccessful in OG), respectively (P > .05). Ultrasound revealed the testicular volume increased by 0.10 mL (31.2%) in LG and 0.14 mL (37.6%) in OG after surgery (P > .05). Moreover, the vascular flow was normal in all testes.
There were 6 complications in OG (4.5%), including 3 inguinal hematomas, 1 wound infection, and 2 testicular ascents. Surprisingly, there were only 3 complications in the LG (2.4%), including 2 scrotal hematomas and 1 wound infection. Two out of the 6 complications in OG were Grade III and the rest were Grade I or II (OG and LG) according to Clavien–Dindo classification. No significant difference was found between the 2 groups for complication rate. LG had higher cost than OG (¥8357 ± 485 versus ¥7004 ± 310, 95% CI: ¥1184–¥1521, P = .001). However, most of the increased costs were paid by medical insurance.
The subgroup of older patients was further investigated (Table 2). Of patients who underwent surgery at age 3 years or older (n = 75), laparoscopic surgery was associated with markedly better testicular position than open surgery (low scrotal position rate: 88.1% versus 69.6%, P = .03).
The Data of Laparoscopic Orchiopexy Versus Open Orchiopexy Group in Patients Older than 3 Years
Discussion
This comparative study reveals that laparoscopic orchiopexy is a better method for palpable undescended testis in children, as it has better final testicular position and comparable success rate compared to open orchiopexy.
There are several reasons for the superior testicular position outcomes in laparoscopic surgery. First, laparoscopy could provide a wide range of testicular dissection and complete releasing of spermatic vessels, which allow for satisfactory orchiopexy.6,8 By this way, it can improve the length of spermatic cord and bring down the testis to the button of scrotum without tension. Conversely, in open surgery the dissection is difficult in the retroperitoneum close to the lower pole of the kidney. In addition, the testis could easily go through the inguinal canal by the medial side of inferior epigastric vessels, which shorten the distance from abdomen to scrotum. 7 For high position testis, the advantage of laparoscopy becomes more obvious. Extensive dissection could provide a good testicular position in laparoscopic surgery. The success rate of laparoscopic orchiopexy for high palpable testes is high (up to 97%), with extensive anatomical retroperitoneal dissection of spermatic vessels. 10 Riquelme et al. treated 192 cryptorchid palpable testes with laparoscopy and found the excellent outcomes – only 2 (0.4%) testicles had reascended, and there was no testicular atrophy. 8 Similarly, Elderwy et al. revealed that laparoscopic orchiopexy had a comparable success rate with open orchiopexy, and laparoscopy was relatively more effective, as it had less redo cases. 3 A study from He et al. reported 103 inguinal canalicular palpable undescended testes that were managed with laparoscopy. Only 1 complication was encountered and all of the testes had adequate size and intrascrotal position. 5
One of the limitations of open surgery is the increased risk of recurrence and testicular malposition, especially in older children who have long distance from inguinal to scrotum. In the present study, the final testicular position of OG is markedly inferior to that of LG in the patients older than 3 years (Table 2). Thus, for patients older than 3 years with undescended testis, laparoscopic orchiopexy may be recommended for better outcomes.
Since most practitioners would consider a secure upper scrotal position as a successful outcome, 11 both of the 2 groups have excellent success rates. Either procedure is acceptable for palpable testis. Nevertheless, in clinical practice, if the surgeon wants to achieve a favorable scrotal position, laparoscopic surgery may be the better option.
The previous studies did not identify significant differences between laparoscopic and open orchiopexy for palpable testis. Pastor Escarcega-Fujigaki et al. compared the outcomes of laparoscopic versus open orchiopexy for 75 palpable testes, and found that the results were almost equal. 7 Our findings differ from those early studies about the final testicular positions, probably due to a larger number of patients in present study.
Laparoscopy has a trend of fewer complications than open surgery. In our study, we found that no Clavien–Dindo Grade III complications in laparoscopic surgery, while there were 2 in open surgery. A possible reason for this may be the magnification of laparoscopy during surgery, which provides a better visualization and wider dissection of the anatomic structures, allowing the descent of testis without injury of the spermatic cord. Moreover, the wounds are small in laparoscopic surgery, so this method reduces bleeding and other complications. On the contrary, there is limited vision and dissection in open procedure because of the small working space, which challenges surgeon to avoid lesions of nearby structures, including the testicle.
In laparoscopic group, there were 2 patients with scrotal hematoma, which was likely caused by the injury of small vessels in the inguinal region and scrotum. After that, we confirmed the hemostasis during surgery and compressed the wound to prevent bleeding. No wound bleeding happened again.
There is also an advantage of being able to repair the contralateral inguinal hernia simultaneously in the laparoscopic orchiopexy. This way can prevent the occurrence of metachronous contralateral hernia in the future and reduce the medical care costs. 12
In the present study, the testicular volumes were checked by ultrasound, which provided objective index for testis development. In the previous studies, the testes were usually measured by clinical palpation or orchidometer. 11 Such methods were not so accurate as ultrasound and they could not check the vascular flow. Our study demonstrated the testicular volume increased after surgery in both groups. This indicated the clinical efficacy of orchiopexy. However, there was no significant difference for testicular volumes growth between the 2 groups.
In the laparoscopic group, it is unnecessary to repair the associated ipsilateral hernia during surgery and no hernia occurred on follow-up. As the peritoneum around internal ring has been adequately dissected, no repair of the hernia is necessary. Khairi et al. performed 210 laparoscopic orchiopexy and left the internal ring open, found that there were no cases of inguinal hernia, and concluded that closing the peritoneum over the area of the deep inguinal ring may not be necessary. 13
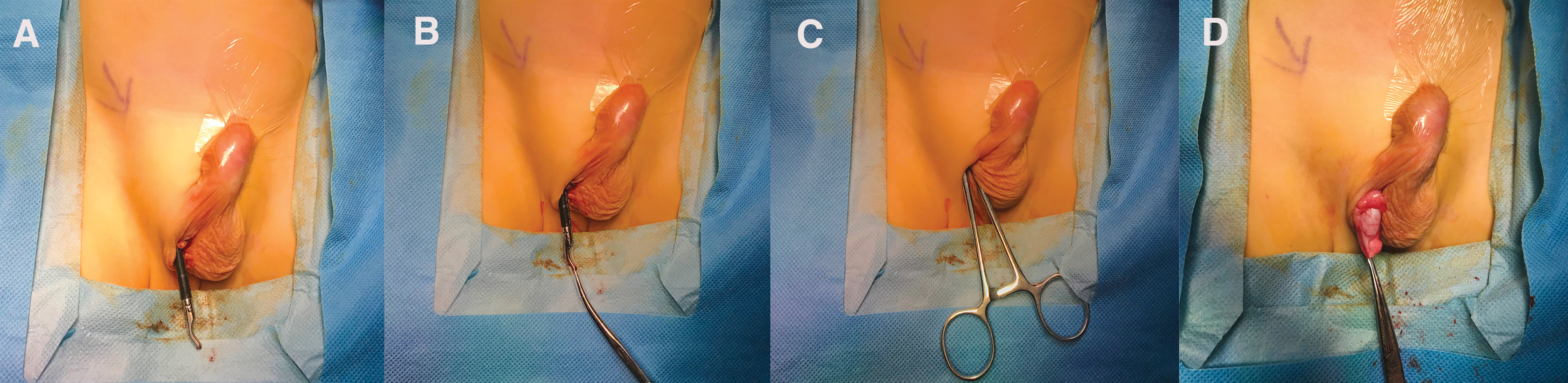
We prefer to pass a laparoscopic dissector from the port on the affected side and pass through the inguinal canal and externalize through the scrotum to guide a forceps from the scrotum (Fig. 3A–D). It is a simple and safe approach to pull down the testis through the inguinal canal without unexpected injury. In the previous study, a trocar was introduced through scrotum to the peritoneal cavity.7,8
One advantage of our study is that it is a prospective study. Moreover, it was conducted to study a large number of cases, and the outcomes were evaluated by the third blind doctors. Finally, all the testes were measured by ultrasound before and after surgery. Thus, the data are objective and reliable.
We acknowledge that there are some limitations in the present study. First, it is not a randomized study. In addition, long-term follow-ups are needed to confirm these initial outcomes.
Conclusions
Laparoscopic orchiopexy is associated with better testicular position and comparable success rate compared with open orchiopexy for palpable undescended testis in children. This procedure could be recommended for palpable undescended testis, especially in older children.
Footnotes
Acknowledgments
The authors acknowledge Pan Zhao, Guanglun Zhou, Weiguang Zhao, and Yingtian Zhang for their refinement of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by Sanming Project of Medicine in Shenzhen (SZSM201612013).