
Abstract
Purpose:
The aim of this study was to investigate the clinical effectiveness of azygos vein preservation when using a thoracoscope in the operation for type III esophageal atresia for children.
Materials and Methods:
We retrospectively analyzed the clinical data of 34 patients (group B) who underwent the thoracoscopic operation of type III esophageal atresia with azygos vein preservation from January 2017 to April 2018. The clinical data of 36 patients (group A) who underwent the thoracoscopic operation of type III esophageal atresia with azygos vein mutilation from April 2015 to December 2016 were selected as a control group.
Results:
All patients were successfully operated on. There was no significant difference in the operation time, amount of bleeding, mechanical ventilation time, and intensive care time between the azygos vein mutilation group and azygos vein preservation group. Compared with the operation severing the azygos vein, preservation of azygos vein has obvious advantages in postoperative hospitalization time, the incidence of anastomotic leakage (P < .05). The follow-up results for 1 year after the operation showed that the incidence of anastomotic stricture with preservation of azygos vein was significantly lower than that with azygos vein transection (P < .05).
Conclusions:
The thoracoscopic operation of type III esophageal atresia with azygos vein preservation can not only improve the edema of esophageal tissue around the esophagus, but also reduce the occurrence of esophageal anastomotic leakage and accelerate the postoperative recovery of children, and it has the same safety as the operation with azygos vein mutilation.
Introduction
Congenital esophageal atresia is a serious malformation of digestive tract caused by abnormal development of primary foregut in embryonic period with the incidence rate of about 1:2500–4500.1–3 Among them, cross type III is the most common, accounting for ∼85%, and surgery is the only way to treat it. 4 With the rapid development of surgical technology it is no longer difficult to restore esophageal continuity, but the postoperative complications still haunt the majority of pediatric surgeons. 5
The traditional esophageal atresia was described in the classic “three steps,” and the first step was to separate and ligate the azygos vein arch. 6 However, the azygos vein arch collects a significant portion of the blood from the esophagus and mediastinum, chylous eventually flows to the venous system, and part of the collateral lymphatic vessels of the thoracic duct flow directly into the azygos vein. 7 Therefore, the azygos vein arch is a vessel of considerable anatomical significance. The purpose of this study was to investigate the clinical effect of thoracoscopic treatment of type III esophageal atresia by retaining the azygos vein, and to provide a reference for the improvement of esophageal atresia.
Materials and Methods
This study was approved by the ethics committee of our university and strictly adhered to the tenets of the Declaration of Helsinki. All patients' guardians signed an informed consent form before the operation.
Patients
We began the thoracoscopic operation of type III esophageal atresia with azygos vein preservation in January 2017 at our hospital. We retrospectively analyzed the clinical data of 34 patients (group B) who underwent the thoracoscopic operation of type III esophageal atresia with azygos vein preservation from January 2017 to April 2018. The clinical data of 36 patients (group A) who underwent the thoracoscopic operation of type III esophageal atresia with azygos vein mutilation from April 2015 to December 2016 were selected as a control group. All the operations were performed by a team of pediatric surgeons in our hospital and the anastomoses was performed the same way with the same suture in all cases. The clinical data included preoperative general data, operation time, amount of bleeding, mechanical ventilation time, intensive care time, postoperative hospitalization time, postoperative complications, and postoperative follow-up data. All the patients' preoperative clinical data are shown in Table 1, and there were no statistically significant difference between the two groups.
Comparison of Preoperative General Data Between the Two Groups
Patients met the inclusion criteria if they presented with type III esophageal atresia. Patients were excluded from this study if they (1) had other types of esophageal atresia, (2) had a poor overall state of health (i.e., severe hepatic or renal insufficiency), and (3) refused to sign the consent form for surgery or refused to comply with the follow-up schedule.
Technology
After successful anesthesia, the left slope position was used and the right side was raised ∼45°. The bed was tilted slightly to the left and the right hand was raised naturally to the ear side, and routine disinfection was done. The incision of 0.5 cm on the intersection of the right subscapular angle line and the fourth intercostal was cut. Mosquito forceps were used to separate tissue layer by layer into the right chest cavity. Then a 5 mm trocar was inserted, whereas the artificial pneumothorax pressure was maintained at ∼7 mmHg. Under the guidance of thoracoscopy, a 3 mm trocar was placed on the intersection of the right midaxillary line and the third intercostal, then a 3 mm trocar was placed on the intersection of posterior axillary line and the sixth intercostal (Fig. 1). The pleura adhesion was separated by 3 mm forceps, a noninvasive gripper, and an electric hook. Then pleura around azygos vein was opened by right angle bending forceps. We opened a space close to the superior azygos vein with right angle bending forceps and blunted separation behind the azygos vein, and opened the inferior azygos vein in the same way. Then the azygos vein was exposed with no cutting of the azygos vein (Fig. 2).

The position of trocar.
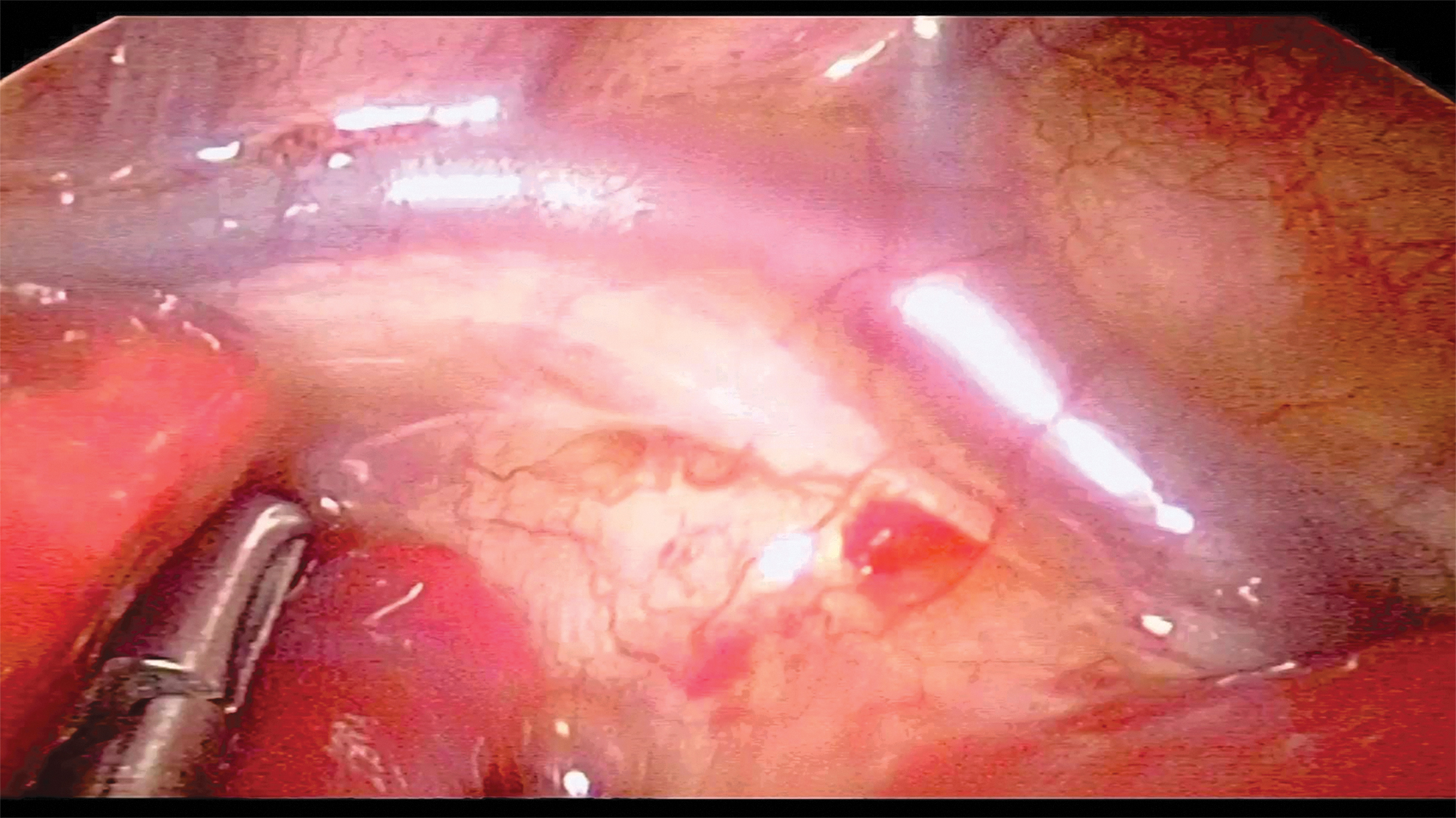
The azygos vein was exposed.
Without cutting of the azygos vein, we bluntly separated tissue in the left edge of the spine next to the trachea with protection of vagus nerve. By lifting the azygos vein a little forward, in the posterior wall of the bifurcation of the left and right trachea, the tracheoesophageal fistula was seen. After fully dissociating the blind end of the distal esophagus and the tracheoesophageal fistula, the fistula was ligated with 3-0 silk thread and the fistula was ligated with 5-0 absorbable sutures at the distal end (Fig. 3). The anesthesiologist needs to expand the right lung and see that the right lung remains well inflated. The pleura of the wall layer was opened upward from the space above the azygos vein and we separated it to the top of the pleura. Under the guidance of the No. 10 gastric tube, at the level of the lower edge of the third thoracic vertebrae, the proximal blind end of the esophagus was found. The proximal and distal esophageal blind ends were then fully free, and the two ends of the esophagus were brought close to each end of the esophagus. The fistula was then resected. The proximal blind end of the esophagus was cut open, and then the posterior wall of the both ends of esophagus was intermittently sutured with 5-0 absorbable line. The No. 10 gastric tube was introduced into the stomach after the back half circle was sutured, and the anterior wall was properly sutured (Fig. 4).

Ligating tracheoesophageal fistula.
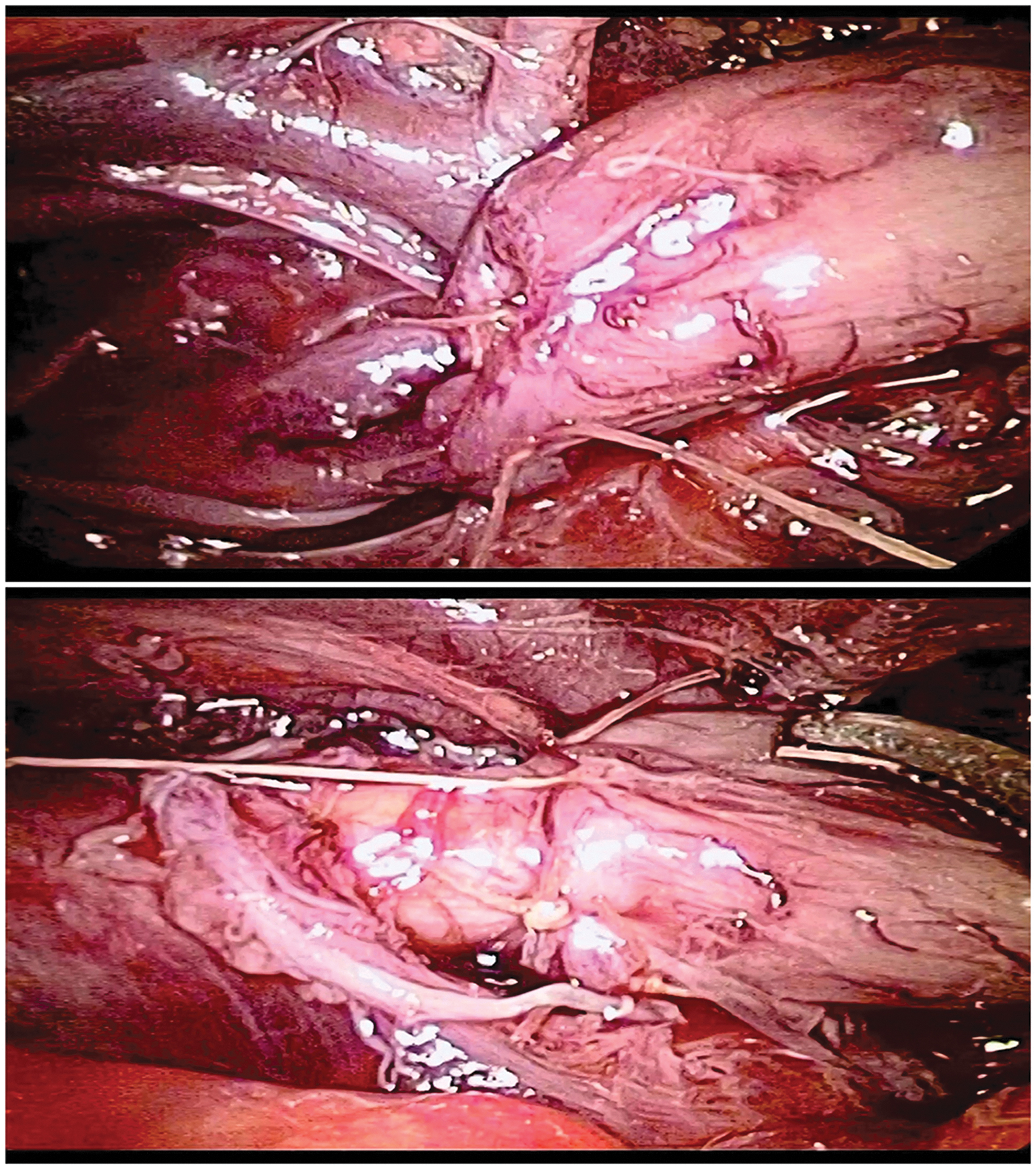
Anastomosing both ends of the esophagus.
After injecting saline into the chest cavity, the anesthesiologist was told to expand the lungs, and if no bubbles were found at the junction of esophagus and trachea fistula, the procedure was concluded. After the pleural cavity wound was examined for no active bleeding, each incision was closed layer by layer. A No. 20 thoracic drainage tube was inserted into the sixth intercostal trocar channel and properly fixed.
Statistical analysis
Continuous data are presented as mean ± standard deviation and range. Clinical parameters between the two groups were compared with the independent samples t-test and χ 2 or Fisher's test to categorical variables. A P value of <.05 was defined as statistically significant.
Result
All patients had a successful operation. Compared with group A, group B did not have statistically significant differences in operation time, amount of bleeding, mechanical ventilation time, intensive care time, recurrence rate of tracheoesophageal fistula, and the pneumothorax incidence rate (P > .05). Compared with group A, group B patients had significant advantages in postoperative hospitalization time, the incidence of anastomotic leakage (P < .05) (Table 2).
Comparison of Intraoperative and Postoperative Parameters Between the Two Groups
Follow-up 1 year after operation showed that the incidence of anastomotic stricture in group B was significantly lower than that in group A (P < .05). There was no significant difference in chest wall deformity, gastroesophageal reflux, tracheomalacia, esophageal diverticulum, and achalasia between the two groups (Table 3).
Comparison of 1 Year Follow-Up Between the Two Groups
Discussion
Congenital esophageal atresia is a common and serious malformation of the digestive tract, which is often complicated with other organ and systematic congenital malformations.1,2 The survival rate of children with esophageal atresia has improved significantly for the past 20 years with the improvement of anesthesia, surgical techniques, neonatal monitoring, and treatment, and will continue to rise in the coming decades.8–11 However, because of the characteristics of esophageal atresia in newborns, it is easy to have various complications after the operation and these complications can threaten the recovery of children with esophageal atresia.12–14
Anastomotic leakage is the most common and serious complications after congenital esophageal atresia. 15 Although the majority of anastomotic leakage can be cured by strengthening thoracic drainage, fasting, parenteral nutrition support, anti-infection, and other conservative treatments, healing is slow, the treatment time is long, and the hospitalization cost is high.15,16 Improving the surgical method and the therapeutic effect while reducing postoperative complications has always been the goal of our pediatric surgeons.
The classic “three-step” description of traditional esophageal atresia plasty includes a first step to ligate and sever the azygos vein arch. 6 However, the azygos venous arch collects a considerable amount of blood from the esophagus and mediastinum. 7 Chyle is eventually transported to the venous system, and some collateral lymphatic vessels of the thoracic duct flow directly into the azygos vein, making conservation of the azygos venous arch important. Although the veins and lymph of the chest return from other collateral circulation elements in children with azygos vein disconnection, this does not achieve a new balance in a short time. Sharma et al. 17 suggested that the azygos vein should be retained to prevent early esophageal anastomotic edema by maintaining venous drainage, thus forming additional protective factors that reduce the risk of an anastomotic leak. Upadhyaya et al. 18 found that the incidence of pneumonia decreased in an azygos vein preservation group.
In this study, the surgeon took measures to protect the azygos vein during thoracoscopic esophageal atresia plasty to maintain the stability of the chest microcirculation as far as possible. During the operation, we found that it was easier to display the proximal esophageal blind end under the guidance of a gastric tube without transection of the azygos vein, and it was not a difficult operation (Fig. 5). Although the confluence of the tracheoesophageal fistula is located on the dorsal side of the azygos vein, good anatomical exposure can also be achieved by pulling the tracheoesophageal fistula (Fig. 6). When anastomotic esophagus was anastomosed, the distal and proximal end of the traction esophagus was close to the anterior edge of azygos vein with the line of 5-0. As long as it was free enough, the anastomotic tension will not increase due to the existence of the azygos vein. Because the esophagus anastomoses was on the anterior edge of azygos vein, the difficulty of stitching will not increase. In this study, there was no significant difference in operation time, amount of bleeding, postoperative mechanical ventilation time, postoperative intensive care time, and recurrence of tracheoesophageal fistula between azygos vein preservation group and azygos vein cutting group.
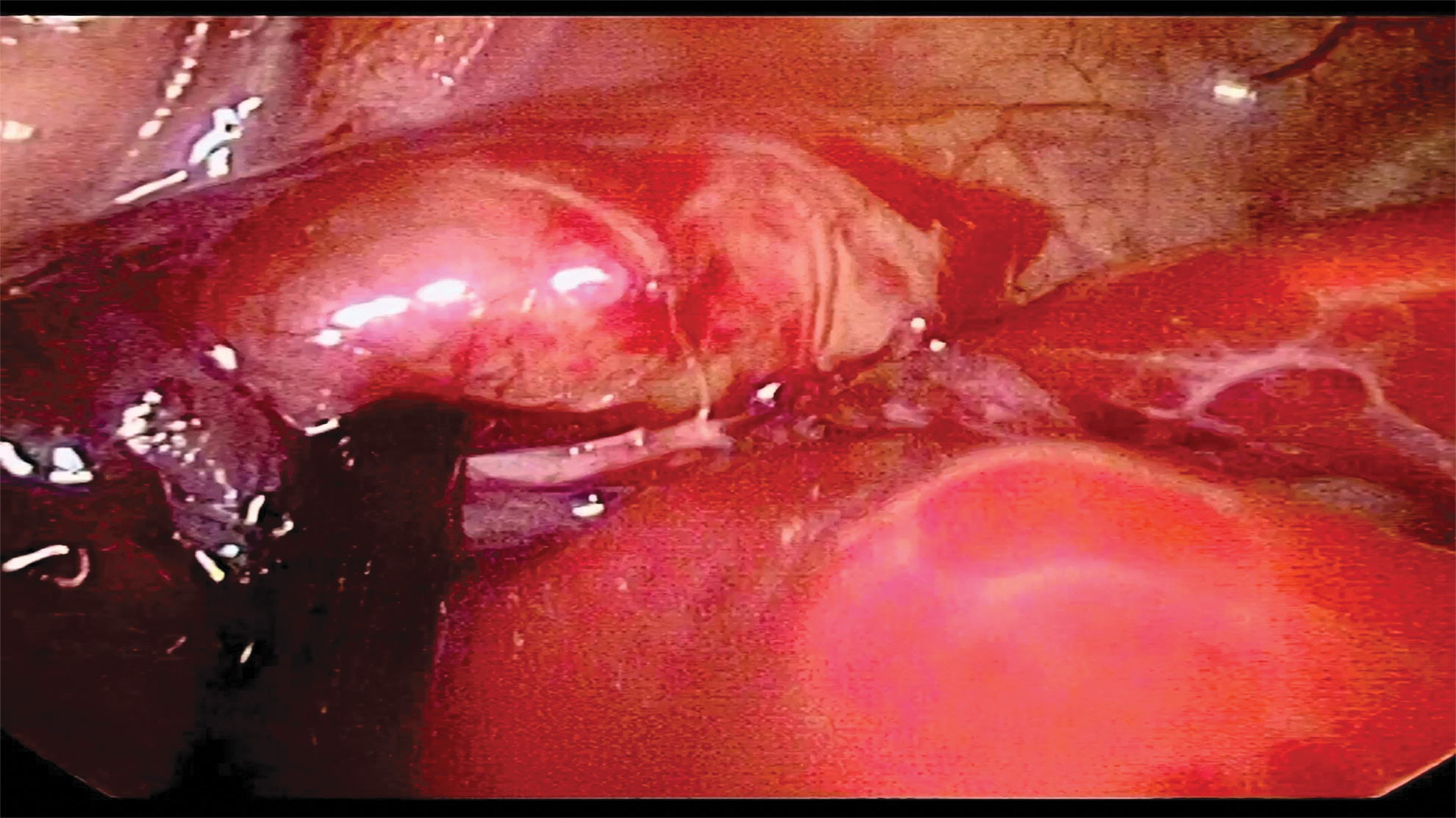
Without cutting azygos vein, under the guidance of gastric tube, it was easy to display the blind end of the proximal esophagus.
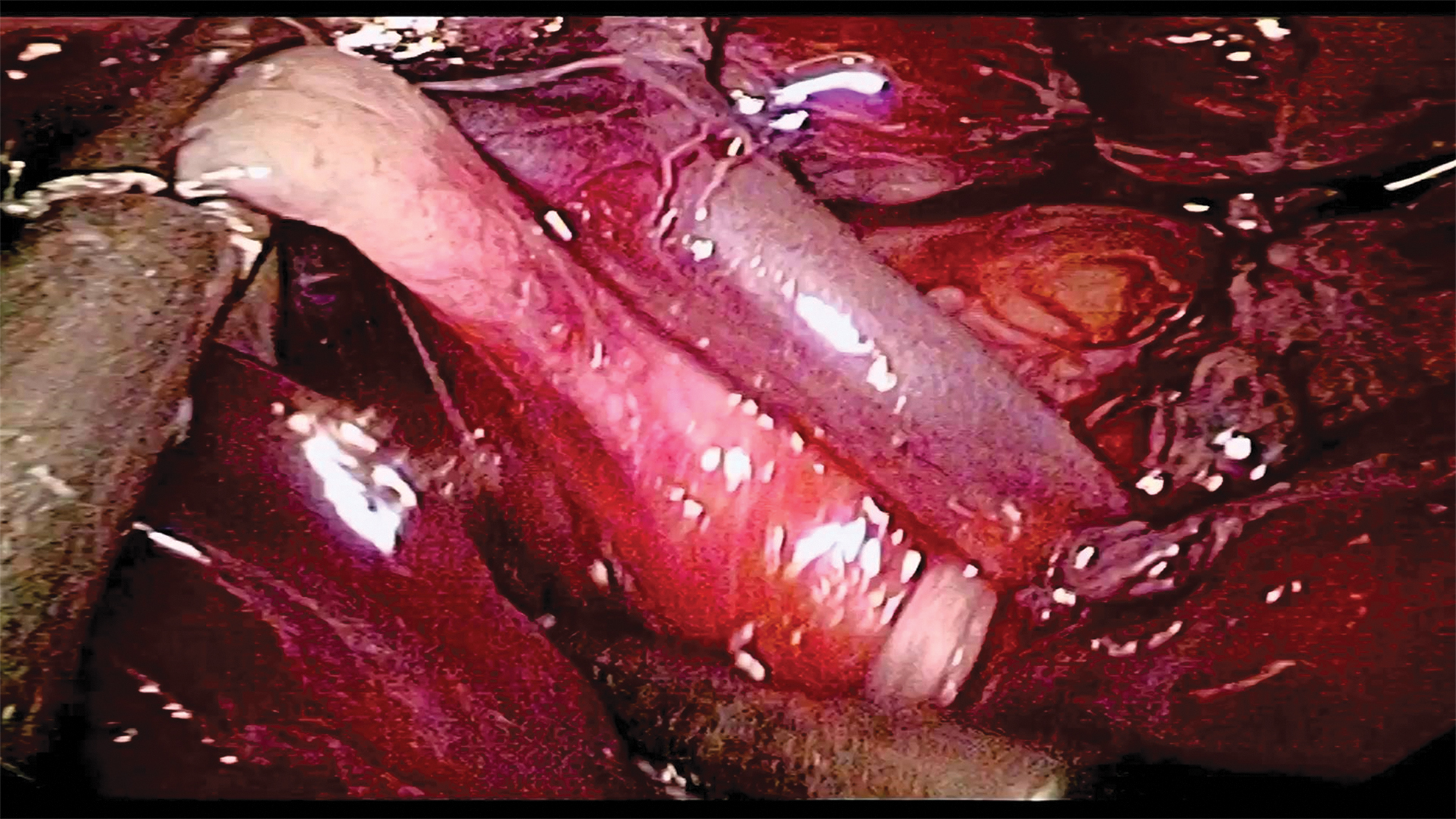
Without cutting azygos vein, good anatomical exposure can also be achieved by pulling esophageal and tracheotracheal fistula.
Anastomotic leakage was the most common complications after the operation of esophageal atresia. The occurrence anastomotic leakage was not only related to anastomotic technique and anastomotic tension, but also closely related to the amount of exudate on the anastomotic site, the degree of tissue edema, and the abundance of blood supply. The incidence rate of anastomotic leakage was 5.9% in azygos vein preservation group, and 19.4% in cutting azygos vein group, and the difference is statistically significant between two groups (P < .05). We consider it was related to the following reasons. First, by retaining azygos vein, the blood supply of local tissue and the accompanying lymphoid duct beside azygos vein were also retained. This is beneficial to the reflux of the mediastinal vein that can reduce pleural effusion and tissue edema. Second, the blood supply of anastomotic tissue can be increased by retaining azygos vein. Third, the preserved azygos vein arch can form a barrier between the esophageal anastomosis and the tracheal fistula ligature, so that the anastomosis of the two positions was no longer in contact, and the effect of exudate from the tracheal fistula ligature on the healing of the esophageal anastomosis was reduced. Studies have shown that anastomotic stricture was closely related to anastomotic inflammation and scar hyperplasia caused by anastomotic leakage. 19 Because the incidence anastomotic leakage after operation in the azygos vein preservation group was significantly lower, the incidence of anastomotic stenosis was also significantly lower.
There are several limitations in this study. First, this was a nonrandomized retrospective study. Second, the historical controls were used, and we will further carry out a prospective randomized controlled study to evaluate the clinical effectiveness of this technique more objectively. Third, this was a single-center study, and more research from multiple centers is mandatory to assess the effectiveness of this technique at further study. Fourth, the follow-up period of this study was brief, and a longer-term follow-up period is needed.
Conclusions
By summarizing the experience of the thoracoscopic operation of type III esophageal atresia with azygos vein mutilation, we have improved the technique of operation by retaining the azygos vein in operation, and it has achieved a good clinical effect. It can not only improve the edema of esophageal tissue around the esophagus, but also reduce the occurrence of esophageal anastomotic leakage and accelerate the postoperative recovery of children, and it has the same safety as the operation with azygos vein mutilation.
Footnotes
Acknowledgments
We highly acknowledge the contribution by the participating doctors Dianming Wu, Yifan Fang, Bing Zhang, Mingkun Liu, Jiancai Chen, Jianxi Bai, and Wen-chen Xu.
Authors' Contributions
X.C. and C.Z. designed the study, collected the clinical data, performed the statistical analysis, participated in the operation, and drafted the article. Y.H., L.C., Y.L., Y.W., and J.Z. participated in the operation and revised the article. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was sponsored by the hospital project of Fujian Provincial Maternity.